
Mohammad Irfan Akhtar1, Mohammad Hamid2
1Assistant Professor; 2Associate Professor
Department of Anesthesiology, Agha Khan University, PO Box 3500, Karachi (Pakistan)
Correspondence: Dr. Mohammad Hamid, Associate Professor, Department of Anesthesiology, Aga Khan University, PO Box 3500, Karachi (Pakistan)
ABSTRACT
Central venous access is still the standard of care in critically ill patients despite several controversies.Ultrasound guided central venous access is now considered to be the standard of care practice due to its better safety and accuracy profile.
Ultrasound guidance not only reduces the number of attemptsbut also the associated complications reported for landmark technique. Adequate training is mandatory to achieve desired results,but the learning curve is highly variable from person to person. It is recommended that at least 10 supervised ultrasound-guided vascular access procedures must be done by a physician to show competency. Two techniques are suggested for central venous cannulation, static or prescan technique and real time or dynamic technique. The vessel can be targeted in short axis or in long axis plane.Linear transducers with higher frequencies between 7.5 and 12 MHz are preferred for vascular access procedures.To remember the procedure steps, a mnemonic abbreviated as 4P’s is suggested which indicate prescanning, preparation of patient and probe, poke in and path identification.Sterility must be observed during the ultrasound guided central venous access. Appropriate documentation is an essential part of the procedure.
Real-time ultrasound guidance for cannulation of the IJV is supported by current literature. It has managed to reduce the complications associated with central line insertion and clearly improves the success rate.
Key words: Ultrasound; Ultrasonography;Central Venous Catheterization;Central Venous Catheter; Central Venous Pressure;Jugular Veins; Subclavian Vein;Review
Citation:Akhtar MI, Hamid M. Ultrasound guided central venous access; a review of literature.Anaesth Pain & intensive Care 2015;19(3):317-322
INTRODUCTION
Central venous access is still the standard of care in critically ill patients despite several controversies.In USA approximately 5 million catheters are placed each year to manage critically ill patients.1Recently, there has beena decreasing emphasis on central venous access for hemodynamic monitoring due to lack of clear evidence and associated complications.Most of the societies discourage the routine use of central venous access. Introduction of ultrasound for central venous access has managed to reduce the complication rate. Ultrasound guided technique has now overtaken the previously used blind technique for central venous access due to its safety and limited attempts.
Ultrasonography for central venous access was first described by Ullman and Stoeltingin 1978. They marked the skin overlying the internal jugular vein (IJV) by using Doppler localization. It wassuggested that this new technique would increase the success rate andlower the incidence of accidental carotid artery puncture in comparison with the traditional technique using only anatomical landmarks.2 The real-time ultrasonographic guidance for the IJV cannulation3was first introduced in 1986 by Yonei and his colleagues, since thenultrasound guidance for vascular access has been increasingly utilized.The Agency for Healthcare Research and Quality (AHRQ) also recommended the widespread use of ultrasonography during central venous access based on the available evidence in the literature.4Ultrasound guided central venous access is now considered to be the standard of care practice due to its better safety and accuracy profile.
PRINCIPLES OF ULTRASOUND
Ultrasound is the sound above the audible capacity of human ear (>20 KHz).The ultrasound waves, which are beingused for medical practice, range from 2 to 12 MHz.When a sound wave is produced by ultrasound probe and aimed at a target, it strikes the target and is reflected back to its origin. The phenomenon of piezoelectric effect needs to be understood to describe the process of ultrasound image formation.Piezoelectric effect is conversion of electric impulses into ultrasound waves, created by vibration of crystals (present in the ultrasound probe) and vice versa.These two principles are utilized in creating an image on the screen. A probe containing piezoelectric crystals is stimulated by electrical signals, sends a series of short sound wave pulses into the body and then waits in between pulses to listen for the returning sounds.Different structures have variable impedancefor ultrasound sound waves. Direction and depth of each returning sound wave is received by the US machine and coverts this into a point of light on a monitor. Thousands of these pulses are computed and displayed every second on the monitor to create a real time image.
Comparison between Landmark Technique and Ultrasound Guided Technique
The incidence of complications during central venous cannulation (CVC) is reported to be 2-15%.5 There are several factors which influence these complications including the experience of physician and the overall status of the patient.6,7 Common complications of CVC are pneumothorax (0-6.6%), carotid artery puncture (6%), subclavian artery puncture (0.5-4%), and hemothorax (1%).5 The failure rate with traditional technique is also quite high (approximately 12%).6 Several studies have demonstrated that ultrasound guidance increases the success rate of CVC insertion and may reduce the frequency of complications.7 Ultrasound guidance not only reduces the number of attempts but also helps in protecting the adjacent artery from injury.8
TRAINING ISSUES
Individuals acquire the required knowledge and skills with varied learning curve. Troianos et al. have recommended that at least 10 supervised ultrasound-guided vascular access procedures must be done by a physician to show competency.9While Kaye et al. observed that fewer complications are noticed when anesthesiologists were able to perform at least 20 supervised central venous insertions under ultrasound guidance than lesser experienced physicians.4
Two-dimensional ultrasound, color flow Dopplerand spectral Doppler are commonly usedin this technique to recognize vessels and surrounding anatomical structures. The operatormust have a complete knowledge of ultrasound machine, probe manipulation, image display, the physics of ultrasound, mechanisms of image production and their interpretation.
Level of evidence for the clinical practice
The committee of American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists reviewed the scientific evidence (between year 1990 to 2011) for ultrasound guided vascular access and they recommended the use of ultrasoundon the basis of category A andlevel 1 evidence (multiple randomized controlled trials supported by meta-analysis).9
The two meta-analyses which have been published, comparing the landmark technique versus the ultrasound-guided technique,concluded that the ultrasound-guided technique leads to fewer failures and a lesser number of attempts than the traditional technique.10,11 In the pediatric setting as well, literature suggests the advantage of ultrasound technique over the traditional technique.12 The Agency for Healthcare Research and Quality of the USA and the UK National Institute of Clinical Excellence,13 both recommendedCVC with ultrasound guidance as one of the safest practices to augment better patient care.
Qualifications of the ultrasound user for vascular access
Training of ultrasound guided central venous access includes didactic teaching in physical principles of ultrasound, knobology (noun, (uncountable); the functionality of controls on an instrument as relevant to their application; www.yourdictionary.com) of ultrasound machine and hands on training of different techniques. Competency can be assessed on a simulated patient or in an actual patient care setting.14,15For trainees, direct observation of procedural skills (DOPS) can be formulated and implemented to ensure standardized ethical training.
PROCEDURE
Selection of Central Vein
Right internal jugular vein (RIJV) is commonly used for this purpose. RIJV runs a straight course in the neck and continue as superior vena cava (SVC) after joining with innominate vein. RIJV is preferred because the right pleural dome is lower than left, its diameter is generally larger than the Left IJV, absence of thoracic duct and ease of insertion by right handed physicians. There are two angulations on the left side which makes the catheter placement in LIJV slightly difficult. First angulation is at the level of LIJV and innominate and second one at innominate and superior vena caval junction. Femoral vein is rarely used due to infection related issues. Subclavian veins can also be used for central venous access but this vein should be avoided in chronic dialysis patients as the potential subclavian stenosis or thrombosis may compromise ipsilateral arteriovenous fistula in these patients.
Techniques for Ultrasound Guided Vascular Access
Basically, two techniques are suggested for central venous cannulation, static or prescan technique and real time or dynamic technique.The vessel can be targeted in short axis or in long axis plane. All these techniques have their own pros and cons which are described below.
Real time versus static technique
Real time ultrasound guidance is the most effective technique as the needle advancement can be visualized. It is a sterile technique which utilizesdrapes, sterile gloves, gel and sterile probe cover.The needle can be observed on the monitor and simultaneously positioned towards the intended vessel, away from adjacent structures, and penetrated to an appropriate depth as assumed by ultrasound depth scale displayed on the machine.
Static or prescan ultrasound image identify the skin puncture site over the underlying vessel, which saves time by eliminating the need for sterile probe covering and gel.In this technique the ultrasound workonly as a vessel locator, obviating the requirement of locator needle as used in landmark technique.
Both static and real time ultrasound approaches are superior to a traditional landmark guided approach. Real time ultrasound guidance is superior to the static ultrasound approach butthe incidence of complication is similar.16
Short Axis Vs Long Axis Visualization
Vascular structures may appear in short axis (SAX) or long axis (LAX) depending on the ultrasound plane orientation in relation to the vessel.
In a SAX view, theprobe and image plane is perpendicular to the course of the vessel.17 The vessel appeared as an anechoic circle on the screen and the needlevisualized as a small hyperechoic point (Figure 1). Out of plane technique is commonly used with SAX view. The surrounding structures are better visualized in this view.The advantage of the SAX view is that you can also visualize an artery, which is in close proximity to central vein. This identification will help the operator in avoiding inadvertent cannulation of the artery. In addition, SAX approach is easy to learn and the cannulation time is much shorter when compared with LAX approach.18
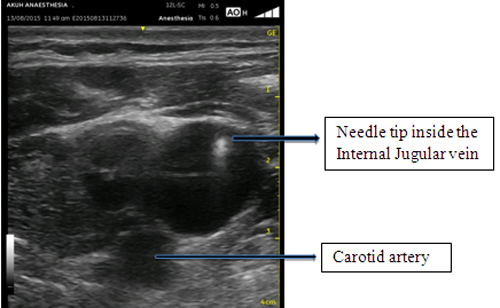
Figure 1: Showing a short axis view of internal jugular vein, needle tip and carotid artery
In a LAX view, the probe and the image plane is parallel to the course of the vessel. The image shows the course of the vessel across the screen and the whole needle can be visualized as it is advanced.In plane approach is usually used with LAX view.LAX view of the vessel has the advantage of needle visualization throughout its course. Other advantages include better assessment of the depth of needle tip and avoidance of needle placement beyond the central vein.
Aligning the ultrasound probe and needle during vascular access requires operator’s hand-eye coordination. Although SAX view is easier to adopt and enables the performer to visualize surrounding structures in relation to central vein but still the needle path and depth cannot be visualized. Lax view is preferred as the entire needle length is visualized and once the central vein is accessed;the performer can see the guide wire entrance into the vein in real time (Figure 2).
Lateral in-plane technique has also been described in literature. In this technique IJV is visualized in short axis and the needle is introduced in plane from lateral side of transducer.19
Differentiating an Artery from a Vein
Arteries and veins appear as an anechoic (black) lumen with relative hyperechoic margins. However, arterial margins are slightly brighter due to thicker walls than the veins. Arteries are pulsatile and less compressible than veins, but both can be compressed with enough pressure.Doppler imaging can be used to locate blood flow and to help differentiate arterial from venous flow.Use of color Doppler will help in identification of a vessel (Image 3) but remembered color on Doppler only indicates flow towards the probe and blue color is suggestive of flow away from the probe. This will depend on probe orientation with respect to target structure. Veins are easily compressible, non pulsatile and usually larger than an artery. Use of pulse wave Doppler is very helpful in differentiating an artery from vein.
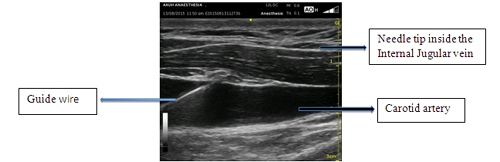
Figure 2: Long axis view of internal jugular vein with guide wire
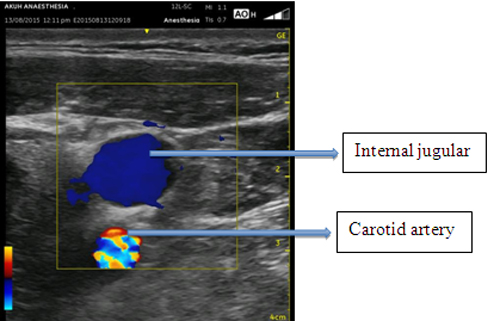
Figure 3: Showing color Doppler image of internal jugular vein and carotid artery in short axis view
Equipment Specification
Linear transducers with higher frequencies between 7.5 and 12 MHz are preferred for vascular access procedures. Lower frequencies are used for deeper vessels. Hockey stick typesof probes are preferred in children or in areas wherethe space is limited. Color flow or spectral Doppler imaging is very helpful in differentiating an artery from vein.
Sterility must be maintained during the procedure. Sterile probe covers should be available for all central venous access procedures. Other requirements include adequate lighting and space, monitoring of ECG, BP, SaO2 and access to emergency equipment.
Setting up of ultrasound machine for the procedure includes selection of CVC option for examination, adjustment in the depth and gain.
Performing the Procedure
To remember the procedure steps,a mnemonic abbreviated as 4P’s is suggested which indicate prescanning,preparation of patient and probe, poke in and path identification.
Ultrasound gel must be placed inside the sterile sheath while sterile gel used on the outside. Avoid air bubbles between the probe and the inner surface of the sterile sheath interface, as this will lead to artifacts and suboptimal visualization because air interfere with ultrasound and deflect the ultrasound waves.Prescanning is usually very helpful in positioning the head in such a way that artery and vein are maximally separated.
Point of skin puncture should be away from probe and the distance between these two should be the same as the depth of the vessel.Middle of the vessel should be targeted and the tip of the needle must be visualized throughout the procedure.Direct visualization of the guide wire within the vein will confirm the proper placement.Hand eye coordination is very important while performing the procedure.Nowadays, needles with hyperechoic tips are in use to accurately target the intended vessel.
Central vein can be access by using two persons’ technique or single person technique.In two person technique, one person holds the probe while other one concentrates on performing the procedure.20 More experienced physicians prefer single person technique which requires better hand eye coordination.21
Confirmation and Documentation
Central venouscannulation must always be confirmed by ultrasound.Before inserting a CVP catheter, use ultrasound probe to visualize the presence of guide wire within the central vein. Injection of agitated saline can also be used to produces hyperechoic contrast within the lumen of the vessel.
Appropriate documentation is essential for both, the procedure and the ultrasound. Documentation includes procedural consent, indication, sterility precautions, any sedation provided, local anesthetics infiltrated at puncture site, number of attempts and type, gauge and length of the central line. In addition, ultrasound image utilized (SAX vs LAX), technique (In plane vs Out of plane) and confirmation of successful placement should also be documented.
Infection Control
Sterility must be observed during the ultrasound guided central venous access. Sterile probe covers are recommended for performing these procedures with adequate sterilization thus avoiding central line related blood stream infections. Use of cap, mask, sterile gloves and gown, skin preparation with chlorhexidene along with full body drapes contribute significantly in reducing the central vein related infection rate.
CONCLUSION
Real-time ultrasound guidance for cannulation of the IJV is supported by current literature. It has managed to reduce the complications associated with central line insertion and clearly improves the success rate. The ultrasound assistance is especially helpful in difficult scenarios like unusual positioning of the vein, coagulopathic and pediatric patients.Standardized training is suggested in the literature to improve patient safety and outcomes.
REFERENCES
- McGee DC, Gould MK. Preventing complications of central venous catheterization. N Engl J Med 2003;348(12):1123-33.[PubMed][Free full text]
- Ullman JI, Stoelting RK. Internal jugular vein location with the ultrasound Doppler blood flow detector. Anesth Analg 1978;57(1):118.[PubMed]
- Yonei A, Nonoue T, Sari A. Real-time ultrasonic guidance for percutaneous puncture of the internal jugular vein. Anesthesiology 1986;64(6):830-1.[PubMed][Free full text]
- Kaye AD, Fox CJ, Hymel BJ, Gayle JA, Hawney HA, Bawcom BA, et al. The importance of training for ultrasound guidance in central vein catheterization. Middle East J Anaesthesiol 2011;21(1):61-6.[PubMed]
- Domino KB, Bowdle TA, Posner KL, Spitellie PH, Lee LA, Cheney FW. Injuries and liability related to central vascular catheters: a closed claims analysis. Anesthesiology 2004;100(6):1411-8.[PubMed][Free full text]
- Bo-Linn GW, Anderson DJ, Anderson KC, McGoon MD. Percutaneous central venous catheterization performed by medical house officers: a prospective study. Cathet Cardiovasc Diagn 1982;8(1):23-9.[PubMed]
- Eisenhauer ED, Derveloy RJ, Hastings PR. Prospective evaluation of central venous pressure (CVP) catheters in a large city-county hospital. Ann Surg 1982;196(5):560-4.[PubMed][Free full text]
- Denys BG, Uretsky BF, Reddy PS. Ultrasound-assisted cannulation of the internal jugular vein. A prospective comparison to the external landmark-guided technique. Circulation 1993;87(5):1557-62.[PubMed][Free full text]
- Troianos CA, Hartman GS, Glas KE, Skubas NJ, Eberhardt RT, Walker JD, et al. Guidelines for performing ultrasound guided vascular cannulation: recommendations of the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr 2011 Dec;24(12):1291-318.[PubMed]doi: 10.1016/j.echo.2011.09.021.
- Randolph AG, Cook DJ, Gonzales CA, Pribble CG. Ultrasound guidance for placement of central venous catheters: a meta-analysis of the literature. Crit Care Med 1996;24(12):2053-8.[PubMed]
- Hind D, Calvert N, McWilliams R, Davidson A, Paisley S, Beverley C, et al. Ultrasonic locating devices for central venous cannulation: meta-analysis. BMJ 2003;327(7411):361.[PubMed][Free full text]
- Froehlich CD, Rigby MR, Rosenberg ES, Li R, Roerig PL, Easley KA, et al. Ultrasound-guided central venous catheter placement decreases complications and decreases placement attempts compared with the landmark technique in patients in a pediatric intensive care unit. Crit Care Med 2009;37(3):1090-6.[PubMed]
- Wigmore TJ, Smythe JF, Hacking MB, Raobaikady R, MacCallum NS. Effect of the implementation of NICE guidelines for ultrasound guidance on the complication rates associated with central venous catheter placement in patients presenting for routine surgery in a tertiary referral centre. Br J Anaesth 2007;99(5):662-5.[PubMed][Free full text]
- Evans LV, Dodge KL, Shah TD, Kaplan LJ, Siegel MD, Moore CL, et al. Simulation training in central venous catheter insertion: improved performance in clinical practice. Acad Med;85(9):1462-9.[PubMed]
- Wadman MC, Lomneth CS, Hoffman LH, Zeger WG, Lander L, Walker RA. Assessment of a new model for femoral ultrasound-guided central venous access procedural training: a pilot study. Acad Emerg Med;17(1):88-92.[PubMed][Free full text]
- Schnadower D, Lin S, Perera P, Smerling A, Dayan P. A pilot study of ultrasound analysis before pediatric peripheral vein cannulation attempt. Acad Emerg Med 2007;14(5):483-5.[PubMed][Free full text]
- Moore CL, Copel JA. Point-of-care ultrasonography. N Engl J Med 2011;364(8):749-57.[PubMed][Free full text]doi: 10.1056/NEJMra0909487.
- Stone MB, Moon C, Sutijono D, Blaivas M. Needle tip visualization during ultrasound-guided vascular access: short-axis vs long-axis approach. Am J Emerg Med 2010;28(3):343-7.[PubMed]doi: 10.1016/j.ajem.2008.11.022. Epub 2010 Jan 28.
- Rossi UG, Rigamonti P, Ticha V, Zoffoli E, Giordano A, Gallieni M, et al. Percutaneous ultrasound-guided central venous catheters: the lateral in-plane technique for internal jugular vein access. J Vasc Access 2014;15(1):56-60.[PubMed][Free full text]doi: 10.5301/jva.5000177.
- Mey U, Glasmacher A, Hahn C, Gorschluter M, Ziske C, Mergelsberg M, et al. Evaluation of an ultrasound-guided technique for central venous access via the internal jugular vein in 493 patients. Support Care Cancer 2003;11(3):148-55.[PubMed]
- Milling T, Holden C, Melniker L, Briggs WM, Birkhahn R, Gaeta T. Randomized controlled trial of single-operator vs. two-operator ultrasound guidance for internal jugular central venous cannulation. Acad Emerg Med 2006;13(3):245-7.[PubMed][Free full text]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube