
Mustafa Arslan1, Fatih Poyraz2, Hasan Ali Kiraz3, Metin Alkan1, Gülay Kip4, Özlem Erdem5, Abdullah Özer6, Volkan Sivgin1, Faruk Metin Comu7
1Department of Anaesthesiology and Reanimation; 4Department of Paediatric Dentistry; 5Department of Pathology; 6Department of Cardiovascular Surgery
Medical Faculty, Gazi University, Ankara, (Turkey)
2Department of Cardiology; 7Department of Physiology
Medical Faculty, Kirikkale University, Afyonkarahisar, (Turkey)
3Department of Anaesthesiology and Reanimation, Medical Faculty, Onsekiz Mart University, Canakkale, (Turkey)
Correspondence:
Mustafa Arslan, MD, Department of Anesthesiology & Reanimation, Medical Faculty, Gazi University, Ankara 06510 (Turkey); Tel: 90 312 202 67 39; GSM: 90 533 422 85 77; E-mail: marslan36@yahoo.com; mustarslan@gmail.com
ABSTRACT
Objective:
Ischemia/reperfusion (I/R) injury is an important cause of myocardial damage by means of oxidative, inflammatory, and apoptotic mechanisms. The aim of the present study was to examine the potential cardio-protective effects of dexmedetomidine in a diabetic rat model of myocardial I/R injury.
Methodology:
A total of 18 streptozotocin (55 mg/kg) induced diabetic Wistar Albino rats were randomly divided into three equal groups as follows: the diabetic I/R group (DIR) in which myocardial I/R was induced by ligating the left anterior descending (LAD) coronary artery for 30 min, followed by 2 hours of reperfusion following left thoracotomy, the diabetic I/R dexmedetomidine group (DIRD) which were given 100 μg/kg dexmedetomidine intraperitoneally 30 min before I/R induction by the same method and the diabetic control group (DC) which underwent sham operations without tightening of the coronary sutures. As a control group (C), 6 healthy age-matched Wistar Albino rats underwent sham operations similar to DC group. After the operation the rats were sacrificied and the myocardial tissues were histopathologically examined.
Results:
Microscopic myonecrosis findings were significantly different among groups (p=0.008). Myonecrosis findings were significantly higher in DIR compared to C, DC and DIRD groups (p = 0.001, p = 0.007 and p = 0.037 respectively). Similarly microscopic inflammatory cell infiltration degrees showed significant differences among groups (p<0.0001). Compared to C, DC and DIRD groups, the microscopic inflammatory cell infiltration was significantly higher among DIR group (p < 0.0001, p < 0.0001 and p = 0.009 respectively). Also myocardial tissue edema was significantly different among groups (p = 0.002). The microscopic myocardial tissue edema levels were significantly higher in DIR group than C and DIRD groups (p < 0.0001 and p = 0.022 respectively). Tissue edema was also more prominent in DC compared to C group (p = 0.022)
Conclusion:
Taken together our data indicate that dexmedetomidine may be helpful in reducing myocardial necrosis, myocardial inflammation and myocardial tissue edema resulting from ischemia/reperfusion injury.
Key words:
Ischemia reperfusion; Dexmedetomidine; Myonecrosis; İnflammatory cell infiltration; Diabetic rat
Citation:
Arslan M, Poyraz F, Kiraz HA, Alkan M, Kip G, Erdem O, Ozer A, Sivgin V, Comu FM. The effect of dexmedetomidine on myocardial ischemia reperfusion injury in streptozotocin induced diabetic rats. Anaesth Pain & Intensive Care 2015;19(4):—-
INTRODUCTION
Despite the current optimal therapy, the mortality and morbidity of patients with ischemic heart disease (IHD) remain high [1], particularly in patients with diabetes mellitus (DM) [2]. Myocardial infarct size is a major determinant of prognosis in patients with IHD, and development of novel strategies to limit infarct size is of great clinical importance. Clinical studies have shown that DM increased the susceptibility of myocardium to ischemia-reperfusion (I/R) injury.[3,4] The mortality rate in various clinical settings of I/R injury, including acute myocardial infarction,[5,6] and coronary artery bypass grafting [7,8], is higher in patients with DM. Diabetes not only renders the heart more vulnerable to ischemic insult but also abolishes or compromises the effectiveness of cardioprotective interventions such as ischemic pre-conditioning.[9] These available clinical evidences strongly support the notion that DM increases the sensitivity of the heart to I/R injury and elimination of reperfusion injury may further improve the outcome of diabetic patients with IHD.
Dexmedetomidine (DEX) is a highly selective and potent α2- adrenergic agonist with sedative, analgesic, anxiolytic, and sympatholytic effects with lack of respiratory depression. DEX was reported to be protective in I/R injury due to transient global or focal cerebral ischemia in both animal and human studies [10,11] and cardiac I/R injury in animals [12,13] possibly due to its sympatholytic [13], anti-inflammatory [14] and antioxidant effects.[15]
Altough the cardioprotective effect of DEX against I/R injury was shown in animal models without diabetes,[12,13] its potential role in cardioprotection against I/R injury in diabetics has not been studied so far. So we conducted this study to investigate the potential cardioprotective effect of DEX against I/R injury in diabetic rats.
METHODOLOGY
Animals and Experimental Protocol
This study was conducted in the GUDAM Laboratory of Gazi University with the consent of the Experimental Animals Ethics Committee of Gazi University. All animals received human care in compliance with the “Principles of Laboratory Animal Care” formulated by the National Society for Medical Research and the “Guide for the Care and the Use of Laboratory Animals” prepared by the National Academy of Science and published by the National Institute of Health (NIH publication Nr. 85–23, revised in 1985).
In the study, 24 male Wistar Albino rats weighing between 200 and 250 g, raised under the same environmental conditions, were used. The rats were kept at 20-21oC in cycles of 12 hours of daylight and 12 hours of darkness and had free access to food until two hours before the anesthetic procedure. The animals were randomly separated into four groups, each containing six rats.
Diabetes was induced by a single IP injection of streptozotocin (Sigma Chemical, St. Louis, MO, USA), at a dose of 55 mg/kg body weight. The blood glucose levels were measured 72 hours and 4 weeks following this injection. Rats were classified as diabetic if their fasting blood glucose (FBG) levels exceeded 250 mg/dl, and only animals with FBGs of > 250 mg/dl were included in the diabetic groups (diabetes only, diabetes plus ischemia-reperfusion and diabetes plus dexmedetomidine-ischemia-reperfusion). The rats were kept alive for four weeks after streptozotocin injection to allow the development of chronic diabetes before they were exposed to I/R as described previously. [16]
Rats were anesthetized with an IP injection of 100 mg/kg of ketamine. The trachea was cannulated for artificial respiration. The chest was shaved and each animal was fixed in a supine position on the operating table. The chest was opened by a left thoracotomy followed by sectioning the fourth and fifth ribs about 2 mm to the left of the sternum. Positive-pressure artificial respiration was started immediately with room air, using a volume of 1.5 ml/100 g body weight at a rate of 60 strokes/min. Sodium heparin (500 IU/kg) was administered through the peripheral vein in the tail.
After the pericardium was incised, the heart was exteriorized with gentle pressure on the right side of the rib cage. An 8/0 silk suture attached to a 10-mm micropoint reverse-cutting needle was quickly placed under the left main coronary artery. The heart was then carefully replaced in the chest and the animal was allowed to recover for 20 min.
There were four experimental groups. Group C (control; n=6), Group DC (diabetes-control; n=6), Group DIR (diabetes-ischemia-reperfusion; n=6) and Group DIRD (diabetes-ischemia-reperfusion-dexmedetomidine; n=6), which underwent left thoracotomy and received IP dexmedetomidine (Precedex 100 μg/2 ml, Abbott®, Abbott Laboratory, North Chicago, IL, USA) administrated via 100 μg/kg IP route 30 min before ligating the LAD (17-19). A small plastic snare was threaded through the ligature and placed in contact with the heart. The artery could then be occluded by applying tension to the ligature (30 min), and reperfusion was achieved by releasing the tension (120 min).[20] However, after the above procedure, the coronary artery was not occluded or reperfused in the control and diabetic control rats.
All the rats were given ketamine 100 mg/kg IP and intracardiac blood samples were obtained. At the end of the reperfusion period, all rats were sacrified under anesthesia and myocardial tissue was harvested for histopathological analyses.
Histological determinations
All of the specimens were fixed in 10% buffered neutral formalin and embedded in paraffin. To visualize myocardial lesions at different levels, the entire heart was cut into four segments from apex to bottom. The segments were embedded in paraffin and 4-μm thickness cross-sections were cut from each segment.
The slides were stained with Hematoxylin-Eosin (Bio-optica, Milano, Italy) for the evaluation of the tissues’ histological features. The slides were evaluated under light microscope for myonecrosis, inflammatory cell infiltration and edema. A minimum of 10 fields for each slide were examined and graded for severity of changes using scores on a scale of severe (+++), moderate (++), mild (+) and nil (-). [21]
Statistical Analysis
The Statistical Package for the Social Sciences (SPSS, Chicago, IL, USA) 20.0 software was used for the statistical analysis. Variations in blood glucose levels, and histopathological examination between study groups were assessed using the Kruskal-Wallis test. The Bonferroni-adjusted Mann-Whitney U test was used after significant Kruskal-Walliso determine which groups differed from the others. Results were expressed as mean ± standard deviation (Mean ± SD). Statistical significance was set at a p value of <0.05 for all analysis.
RESULTS
Blood glucose measurements were 88.5 ± 8.6, 338.7 ± 40.3, 348.2 ± 52.6 and 343.8 ± 50.5 mg/dL for Group C, DC, DIR and DIRD, respectively. Blood glucose levels after 4 weeks were 106.33 ± 5.68, 321.00 ± 40.09, 359.00 ± 33.02 and 475.50 ± 63.49 mg/dL for Group C, DC, DIR and DIRD. Serum glucose was detected to be significantly lower in Group C when compared to Groups DC, DIR and DIRD (p<0.0001).
Light microscopic myonecrosis findings were significantly different among groups (p=0.008). Myonecrosis were significantly higher in Group DIR compared to Groups C, DC, and DIRD (p=0.001, p=0.007 ve p=0.037 respectively), (Table 1, Figure 1-4).
Table 1: Histopathological findings of the heart tissue (Mean ± SD)
| Group C
(n=6) |
Group DC
(n=6) |
Group DIR
(n=6) |
Group DIRD
(n=6) |
P** | |
| Myonecrosis | 0.0±0.0* | 0.17 ± 0.41* | 0.83 ± 0.41 | 0.33 ± 0.52* | 0.008 |
| Inflammatory cell infiltration | 0.0 ± 0.0* | 0.17 ± 0.41* | 1.17 ± 0.41 | 0.50 ± 0.55* | <0.0001 |
| Edema | 0.17 ± 0.41* | 1.17 ± 0.41+ | 2.00 ± 0.63 | 1.00 ± 1.10* | 0.002 |
* p<0.05: When compared with Group DIR; +p<0.05: When compared with Group C
p**: Statistical significance was set at a p value < 0.05 for Kruskal-Wallis test
Similarly light microscopic inflammatory cell infiltration degrees showed significant difference among groups (p<0.0001). Compared to Groups C, DC and DIRD, the microscopic inflammatory cell infiltration were significantly higher among Group DIR (p<0.0001, p<0.0001 and p=0.009 respectively), (Table 1, Figure 1-4). Also myocardial tissue edema was significantly different among groups (p=0.002). The light microscopic myocardial tissue edema levels were significantly higher in Group DIR than Groups C and DIRD (p<0.0001, p=0.022 respectively) tissue edema was also more prominent in Group DC compared to Group C (p=0.022), (Table 1, Figure 1-4).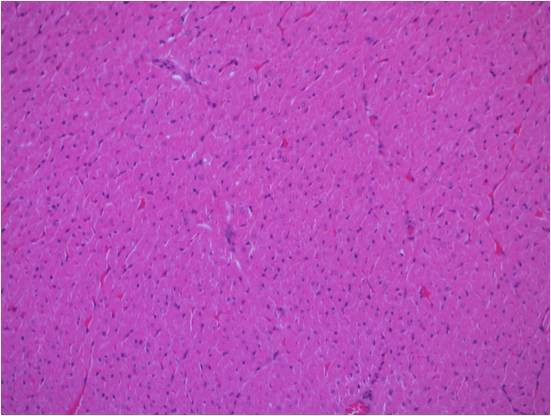 Figure 1: Normal structured myocardial tissue fibers in the control group, H&E x200
Figure 1: Normal structured myocardial tissue fibers in the control group, H&E x200
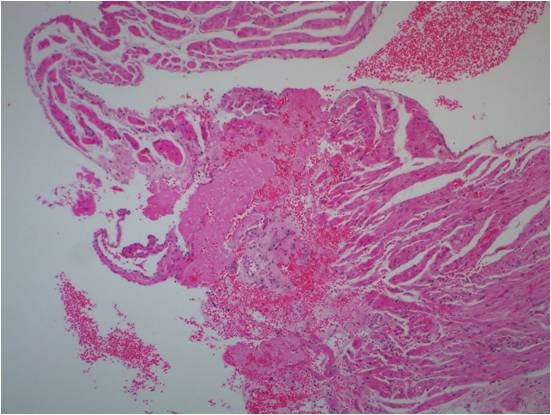 Figure 2: Mild inflammatory cell infiltration and myonecrosis of myocardial tissue in the diabet control group, H&E x200
Figure 2: Mild inflammatory cell infiltration and myonecrosis of myocardial tissue in the diabet control group, H&E x200
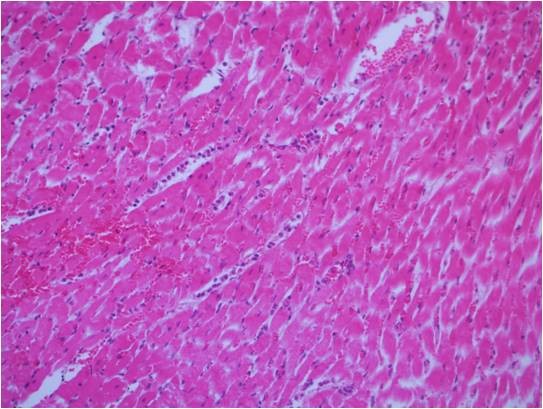 Figure 3: Extensive inflammatory cell infiltration and edeme of myocardial tissue in the diabetic ischemia reperfusion group, H&E x200
Figure 3: Extensive inflammatory cell infiltration and edeme of myocardial tissue in the diabetic ischemia reperfusion group, H&E x200
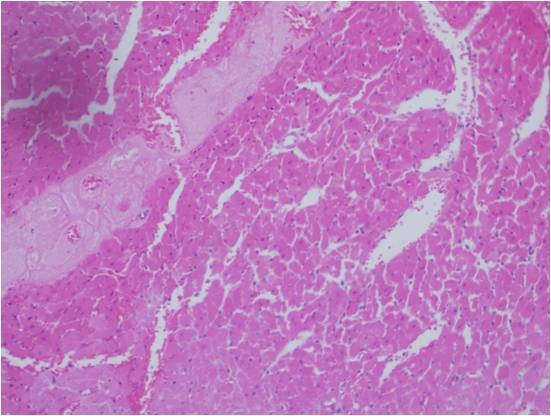 Figure 4: Mild inflammatory cell infiltration and myonecrosis of myocardial tissue in the diabetic ischemia reperfusion dexmedetomidine group, H&E x200
Figure 4: Mild inflammatory cell infiltration and myonecrosis of myocardial tissue in the diabetic ischemia reperfusion dexmedetomidine group, H&E x200
DISCUSSION
The novel finding of this study is that the administration of DEX before induction of ischemia significantly mitigates the myocardial injury induced by I/R in diabetic rat heart. Altough the cardioprotective effect of DEX against I/R injury were shown in the previous experimental non-diabetic heart models,[12,13] these findings can not be generalised to diabetic heart where I/R injury is much more prominent. Our aim in this study was not to explore the potential mechanisms by which DEX exerts cardioprotection against I/R injury, rather we aimed to find out if DEX had any cardioprotective effect in diabetic population. We have shown for the first time that DEX also exerts cardioprotective effects in an experimental model of diabetic rat heart against I/R injury. Our results clearly demonstrated that DEX given before the induction of I/R, significantly decreases the amount of myonecrosis, inflammatory cell infiltration and tissue edema in the myocardial tissue of diabetic rat heart detected histopathologically.
Altough it is well known that diabetic heart is especially susceptible to I/R injury the underlying mechanisms responsible for the increased injury in diabetic myocardium are not fully understood. However, it appears that excessive oxidative stress induced by hyperglycemia plays a major role. In fact, a feature common to all cell types that are damaged by hyperglycemia is an increased production of reactive oxygen species (ROS), particularly increased production of mitochondrial ROS by hyperglycemia is recognized as a major cause of I/R injury in the diabetic myocardium.[22] Moreover, new interesting data came from studies of peroxynitrite and nitrotyrosine in the hyperglycemic oxidative stress in the heart. Acute exposure to high glucose especially under pathological conditions like ischemia, increases inducible nitric oxide synthetase (iNOS) gene expression, paralleled by a simultaneous increase of both nitric oxide (NO) and superoxide (O2¯ ) production. The interaction of O2¯ with NO is very rapid and leads to inactivation of NO and production of the potent oxidant peroxynitrite (NOO−), which causes damage to cellular structures, such as lipids, DNA, mitochondria, ion channels, transporters, enzymes and receptors.[23] Increased plasma nitrotyrosine levels were observed in diabetic subjects[23,24] and furthermore, increased nitrotyrosine formation has been detected during acute myocardial infarction in working rat hearts during hyperglycemia [23] Frustaci et al.[24] showed a co-localization of nitrotyrosine and ischemic damage within the heart of diabetic patients indicating that the two events are correlated. The observation that the increased apoptosis of myocytes in heart biopsies from patients with diabetes, [24] as well as in hearts from STZ-induced diabetic rats [25] is selectively associated with the levels of nitrotyrosine found in those cells, suggests that the oxidative damage and apoptosis of myocardial cells are part of the mechanism by which hyperglycemia exerts its damaging action in diabetes. [23]
Hyperglycemia-dependent myocardial oxidative damage could be amplified by consequent inflammatory process which is also aggrevated by hyperglycemia. Animal studies showed increased levels of proinflammatory cytokines (tumor necrosis factor-α (TNF-α), IL-6, IL-18) and peroxynitrite (an index of oxidative stress) in the myocardium of hyperglycemic mice. The level of the inflammatory cytokines were found to be strictly correlated with the blood glucose levels and cause eventually to myocardial apoptosis and greater infarct size. [26]
During the pathophysiologic process of reperfusion, damage to and dysfunction of endothelial cells within the coronary artery are early and important events [27] that lead to the subsequent apoptosis of cardiomyocytes during the I/R period.[28] Hyperglycemic conditions not only aggravate endothelial cell dysfunction by inhibiting their proliferation and dispersal, but also decrease the expression of the anti-apoptotic protein survivin, resulting in apoptosis in vivo. [29] The results of the above mentioned findings suggest that hyperglycemia, both by amplifying oxidative stress, inflammatory insult and apoptotic responses to myocardial ischemia, increases the amount of myocardial damage and prognosis of patients undergoing I/R stress. Clinical data also confirms the increased susceptibility of diabetic heart to I/R injury. In multiple studies, diabetes was found to be associated with an increased cardiac morbidity and mortality following surgical or nonsurgical (angioplasty and vascular stenting) revascularization techniques.[5,7,8] I/R injury following myocardial revascularization is considered as one of the major factors contributing towrds development of adverse outcomes in diabetic population. Indeed, the mortality rate of diabetic patients after acute myocardial infarction suffering from I/R injury is approximately four to six fold that of nondiabetic patients.[30] So inhibition of inflammation and reducing oxidative stress would be a potential target for reducing I/R injury dependent worse outcomes in diabetic population.
Although the exact mechanism of DEX in preventing I/R injury has not been clarified, there are some opinions on how this drug exhibits its preventive properties for I/R injury. In recent years, a line of studies demonstrated that DEX possesses anti-inflammatory effects, apart from its anesthetic property.[14,28-31] Qiao et al [31] and Taniguchi et al [32] found that DEX may lessen systemic inflammation and increase survival rate in sepsis and endotoxin-induced shock in rats. Can et al [14] also reported the anti-inflammatory effect of DEX in spinal cord injury in rats. Venn et al. [33] and Memis et al. [34] demonstrated that DEX sedation significantly decrease cytokine (IL-1β, TNF-α, and IL-6) production in critically ill patients. Peng et al.[35] demonstrated that high dose DEX pretreatment significantly decresed the microglial production of LPS stimulated pro-inflammatory mediators like NO, prostaglandin E2, IL-1βb, and TNF-α and the expression of iNOS messenger RNA. Similar effects were reported in activated macrophage [15] and cecal ligation and puncture model rats [31]. As exessive iNOS expression and associated inflammatory cytokine release are critically involved in the I/R injury pathogenesis, this anti-inflammatory effects leading to decreased oxidative stress may be the main protective factor of DEX against I/R injury. Our results are concordant in a manner with the previous findings indicating anti-inflammatory effect of DEX after I/R injury as we also observed that the amount of inflammatory infiltrate and tissue edema, most probably accured due to tissue inflammation, was significantly reduced by DEX. However our study was not primarily focused on the mechanism by which DEX exert cardioprotection thus we can not exclude the possibility that decreased myonecrosis itself, occured due to other mechanisms, might be the cause of decreased inflammatory infiltrate seen in DIRD group.
Another possible explanation for the cardioprotective effect of DEX might be the sympatholysis which is one of dexmedetomidine’s properties as a result of its effect via α2- adrenoceptors. Experimental and clinical studies suggest that catecholamines promote the progression of myocardial damage after I/R injury [36]. Previous studies reported that myocardial ischemia rapidly and massively increased the norepinephrine (NE) concentration in the myocardial tissue.[37] Alfa2-adrenergic agonists like DEX have been reported to have protective effects on the ischemic myocardium and attenuate plasma NE levels.[38] Alfa2-adrenoreceptors also exist at sympathetic nerve endings, and cardiac presynaptic α2-adrenoreceptor stimulation decreased NE release from sympathetic nerve endings [39]. Thus, α2- adrenoreceptor stimulation would attenuate the elevation of NE concentration. The attenuation of NE release by DEX may prevent potential destructive effects of excess metabolism caused by NE by means of prohibiting increased free oxygen radical production and reduce oxygen consumption.[40] Another location of α2- receptors are on blood vessels, and DEX causes vasoconstriction due to its α2- agonist property. Maier et al[41] suggested that this effect may improve perfusion of ischemic tissue by increasing vascular resistance in non-ischemic tissue causing ‘‘reverse steal effect’’. Another explanation for the cardioprotective effect of DEX is that, DEX alters the myocardial oxygen balance. In previous studies DEX has been reported to improve myocardial oxygen balance by increasing the ischemic-non-ischemic blood flow ratio and maintaining the oxygen balance in the regional ischemic hearts in dogs.[38] Thus, it can be considered that DEX might exert myocardial protection resulting from the attenuation of the catecholamine response to ischemic stres, redistributing myocardial blood flow and maintain the myocardial oxygen balance.
LIMITATIONS
This study has certain limitations that need commenting. First of all only one dose of DEX was tested. However the dose of DEX were based on previous studies demonstrating cardioprotective effect.[20] Also our study was not conducted to find out the mechanism by which DEX exert for cardioprotection however our results clearly demonstrated that DEX when given before induction of ischemia significantly decreases myocardial tissue necrosis, inflammatory infiltrate and tissue edema in diabetic rat heart. Different dosages, alternative time protocols and researches primarily focusing on the potential protective mechanisms for myocardial injury induced by I/R in diabetic heart should be investigated in future studies.
CONCLUSION
Taken together our data indicate that dexmedetomidine may be helpful in reducing myocardial necrosis, myocardial inflammation and myocardial tissue edema resulting from I/R injury in a diabetic rat model. Our findings may stimulate further studies aiming to conclude the protective effect of DEX especially in diabetic patients who require a coronary artery by-pass operation and so a clinical implication might be obtained.
Conflict of interest: None declared by the authors.
Authors’ contribution: FP: Main author of the article
HAK, AO & FMC: Helped in experimental study
MA, GK & VS: Collection of data
OE: Helped in histopathological interpretation
REFERENCES
- McGovern PG, Pankow JS, Shahar E, Doliszny KM, Folsom AR, Blackburn H, et al. Recent trends in acute coronary heart disease–mortality, morbidity, medical care, and risk factors. The Minnesota Heart Survey Investigators. N Engl J Med 1996;334(14):884. [PubMed] [Free full text]
- Haffner SM, Lehto S, Ronnemaa T, Pyorala K, Laakso M. Mortality from coronary heart disease in subjects with type 2 diabetes and in nondiabetic subjects with and without prior myocardial infarction. N Engl J Med 1998;339(4):229. [PubMed]
- Alegria JR, Miller TD, Gibbons RJ, Yi QL, Yusuf S; Collaborative Organization of RheothRx Evaluation (CORE)Trial Investigators.Infarct size, ejection fraction, and mortality in diabetic patients with acute myocardial infarction treated with thrombolytic therapy. Am Heart J 2007;154(4):743. [PubMed]
- Marso SP, Miller T, Rutherford BD, Gibbons RJ, Qureshi M, Kalynych A, et al. Comparison of myocardial reperfusion in patients undergoing percutaneous coronary intervention in ST-segment elevation acute myocardial infarction with versuswithout diabetes mellitus (from the EMERALD Trial). Am J Cardiol 2007;100(2):206. [PubMed]
- Brener SJ, Mehran R, Dressler O, Cristea E, Stone GW. Diabetes mellitus, myocardial reperfusion, and outcome inpatients with acute ST-elevation myocardial infarction treated with primary angioplasty (fromHORIZONS AMI). Am J Cardiol. 2012 Apr 15;109(8):1111-6. doi: 10.1016/j.amjcard.2011.11.046 [PubMed]
- Donahoe SM, Stewart GC, McCabe CH, Mohanavelu S, Murphy SA, Cannon CP, et al. Diabetes and mortality following acute coronary syndromes. JAMA 2007;298:765. [PubMed] [Free full text]
- Carson JL, Scholz PM, Chen AY,Peterson ED, Gold J, Schneider SH. Diabetes mellitus increases short-term mortality andmorbidity in patients undergoing coronary artery bypass graft surgery. J AmColl Cardiol 2002;40(3):418. [PubMed]
- Cohen Y, Raz I, Merin G, Mozes B. Comparison of factors associated with 30-day mortality aftercoronary artery bypass grafting in patients with versus without diabetes mellitus. Israeli CoronaryArtery Bypass (ISCAB) Study Consortium. Am J Cardiol 1998;81(1):7. [PubMed]
- Engbersen R, Riksen NP, Mol MJ, Bravenboer B, Boerman OC, Meijer P, et al. Improved resistance to ischemia and reperfusion, but impaired protection by ischemic preconditioning in patients with type 1 diabetes mellitus: a pilot study. Cardiovas Diabetol 2012;11:124. doi: 10.1186/1475-2840-11-124 [PubMed] [Free full text]
- Engelhard K,Werner C, Eberspächer E, Bachl M, Blobner M, Hildt E, et al. The effect of the alpha 2-agonist dexmedetomidine and the N-methyl-D-aspartate antagonist S(+)-ketamine on the expression of apoptosis-regulatingproteins after incomplete cerebral ischemia and reperfusion in rats. Anesth Analg 2003;96:524. [PubMed]
- Dahmani S, Rouelle D, Gressens P, Mants J. Effects of dexmedetomidine on hippocampal focal adhesion kinase tyrosine phosphorylation in physiologic and ischemic conditions. Anesthesiology 2005;103:969. [PubMed] [Free full text]
- Okada H, Kurita T, Mochizuki T, Morita K, Sato S. The cardioprotective effect of dexmedetomidine on global ischemia in isolated rat hearts. Resuscitation 2007;74:538. [PubMed]
- Yoshitomi O, Cho S, Hara T, Shibata I, Maekawa T, Ureshino H, et al. Direct protective effects of dexmedetomidine against myocardial ischemia-reperfusion injury in anesthetized pigs. Shock 2012;38(1):92. doi: 10.1097/SHK.0b013e318254d3fb. [PubMed]
- Can M, Gul S, Bektas S, Hanci V, Acikgoz S.Effects of dexmedetomidine or methylprednisolone on inflammatory responses in spinal cord injury. Acta Anaesthesiol Scand 2009;53:1068. doi: 10.1111/j.1399-6576.2009.02019.x. [PubMed]
- Lai YC, Tsai PS, Huang CJ. Effects of dexmedetomidine on regulating endotoxin-induced up-regulation of inflammatory molecules in murine macrophages. J Surg Res 2009;154:212. [PubMed]
- Türeci E, İş M, Üzüm G, Akyüz F, Ulu MO, Döşoğlu M, et al. Alterations in blood-brain barrier after traumatic brain injury in streptozotocin-induced diabetic rats. J Nervous Sys Surgery 2009;2(2):79.[Free full text]
- Cakir M, Polat A, Tekin S, Vardi N, Taslidere E, Rumeysa Duran Z, et al.The effect of dexmedetomidine against oxidative and tubular damage induced by renal ischemia reperfusion inrats. Ren Fail 2015;17:1-5 doi: 10.3109/0886022X.2015.1011550 [PubMed] [Free full text]
- Wang H, Chen H, Wang L, Liu L, Wang M, Liu X. Acute hyperglycemia prevents dexmedetomidine-induced preconditioning against renal ischemia-reperfusioninjury. Acta Cir Bras 2014;29(12):812-8. doi: 10.1590/S0102-86502014001900008.[PubMed] [Free full text]
- Jeon YT, Hwang JW, Lim YJ, Park SK, Park HP. Postischemic sevoflurane offers no additional neuroprotective benefit to preischemic dexmedetomidine. J Neurosurg Anesthesiol 2013;25(2):184-90. doi: 10.1097/ANA.0b013e3182764d2a. [PubMed]
- Kocoglu H, Karaaslan K, Gonca E, Bozdogan O, Gulcu N. Preconditioning effects of dexmedetomidine on myocardial ischemia/reperfusion injury in rats. Curr Ther Res Clin Exp 2008;69:150. [PubMed] [Free full text]
- Loh HK, Sahoo KC, Kishore K, Ray R, Nag TC, Kumari S, et al. Effects of thalidomide on isoprenaline-induced acute myocardial injury: a haemodynamic, histopathological and ultrastructural study. Basic Clin Pharmacol Toxicol 2007;100(4):233. [PubMed]
- Brownlee M. The pathobiology of diabetic complications: A unifying mechanism. Diabetes 2005;54:1615. [PubMed] [Free full text]
- Ceriello A. Acute hyperglycaemia: A “new” risk factor during myocardial infarction. Eur Heart J 2005;26:328. [PubMed] [Free full text]
- Frustaci A, Kajstura J, Chimenti C, Jakoniuk I,Leri A, Maseri A, et al. Myocardial cell death in human diabetes. Circ Res 2000;87:1123. [PubMed] [Free full text]
- Fiordaliso F, Li B, Latini R, Sonnenblick EH, Sonnenblick EH,Anversa P, et al. Myocyte death in streptozotocin-induced diabetes in rats in angiotensin II-dependent. Lab Invest 2000;80:513. [PubMed]
- Marfella R, D’Amico M, Di Filippo C, Piegari E,Nappo F, Esposito K, et al. Myocardial infarction in diabetic rats: role of hyperglycaemia on infarct size and early expression of hypoxia-inducible factor 1. Diabetologia 2002;45:1172. [PubMed]
- Tsao PS, Aoki N, Lefer DJ, Johnson III G, Lefer AM. Time course of endothelial dysfunction and myocardial injury during myocardial ischemia and reperfusion in the cat. Circulation 1990;82:1402. [PubMed]
- Gottlieb RA, Burleson KO, Kloner RA, Babior BM, Engler RL. Reperfusion injury induces apoptosis in rabbit cardiomyocytes. J Clin Invest 1994;94:1621. [PubMed] [Free full text]
- Song Q, An X, Li D, Sodha NR, Boodhwani M, Tian Y, et al. Hyperglycemia attenuates angiogenic capability of survivin in endothelial cells. Microvasc Res 2009;78:257. [PubMed] [Free full text]
- Alegria JR,Miller TD, Gibbons RJ, Yi QL, Yusuf S. Infarct size, ejection fraction, and mortality in diabetic patients with acute myocardial infarction treated with thrombolytic therapy. Am Heart J 2007;154:743. [PubMed]
- Qiao H, Sanders RD, Ma D, Wu X, Maze M. Sedation improves early outcome in severely septic Sprague Dawley rats. Crit Care 2009;13:R136. [PubMed] [Free full text]
- Taniguchi T, Kidani Y, Kanakura H, Takemoto Y, Yamamoto K. Effects of dexmedetomidine on mortality rate and inflammatory responses to endotoxin-induced shock in rats. Crit Care Med 2004;32:1322. [PubMed]
- Venn RM, Bryant A, Hall GM, Grounds RM. Effects of dexmedetomidine on adrenocortical function, and the cardiovascular, endocrine and inflammatory responses in post-operative patients needing sedation in the intensive care unit. Br J Anaesth 2001;86:650. [PubMed] [Free full text]
- Memis D, Hekimoglu S, Vatan I, Yandim T, Yüksel M, Süt N. Effects of midazolam and dexmedetomidine on inflammatory responses and gastric intramucosal pH to sepsis, in critically ill patients. Br J Anaesth 2007;98:550. [PubMed] [Free full text]
- Peng M, Wang YL, Wang CY, Chen C. Dexmedetomidine attenuates lipopolysaccharide-induced proinflammatory response in primary microglia. J Surg Res 2013;179(1):e219. [PubMed]
- Schömig A, Richardt G. The role of catecholamines in ischemia. J Cardiovasc Pharmacol 1990;16:105. [PubMed] [Free full text]
- Lameris TW, de Zeeuw S, Alberts G, Boomsma F, Duncker DJ, Verdouw PD, et al. Time course and mechanism of myocardial catecholamine release during transient ischemia in vivo. Circulation 2000;101:2645. [PubMed] [Free full text]
- Roekaerts PM, Prinzen FW, Lange SD. Beneficial effects of dexmedetomidine on ischemic myocardium of anaesthetized dogs. Br J Anaesth 1996;77:427. [PubMed] [Free full text]
- Matko´ I, Fehe´r E, Vizi ES. Receptor mediated presynaptic modulation of the release of noradrenaline in human papillary muscle. Cardiovasc Res 1994;28:700. [PubMed] [Free full text]
- Hoffman WE, Kochs E, Werner C, Thomas C, Albrecht RF. Dexmedetomidine improves neurologic outcome from incomplete ischemia in the rat. Reversal by the alpha 2-adrenergic antagonist atipamezole. Anesthesiology 1991;75(2):328. [PubMed] [Free full text]
- Maier C, Steinberg GK, Sun GH, Zhi GT, Maze M. Neuroprotection by the alpha 2-adrenoreceptor agonist dexmedetomidine in a focal model of cerebral ischemia. Anesthesiology 1993;79:306. [PubMed] [Free full text]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube