
Tanvir Samra, MBBS, MD1, Kamlesh Kumari, MBBS, MD2, Vikas Saini, MBBS, MD1
1Assistant Professor; 2Senior Resident
Department of Anesthesiology& Intensive Care, Post Graduate Institute of Medical Education & Research (PGIMER), Sector 12, Chandigarh (India)
Correspondence: Tanvir Samra, Assistant Professor, Department of Anesthesiology& Intensive Care, Post Graduate Institute of Medical Education & Research (PGIMER), Sector 12, Chandigarh (India); Phone: (M): 9910703609; E-mail: drtanvirsamra@yahoo.co.in
Abstract
Pneumatoceles have been described as a complication of staphylococcal pneumonia in children. But the management of large (>1 cm) bilateral bronchopleural fistula (BPF) in a child on positive pressure ventilation is a challenge for the intensivist. Bronchoscopy is an efficient method to close small BPFs (1-3 mm); independent lung ventilation cannot be used in patients with bilateral lung involvements; high frequency ventilation is of limited value in patients with distal and parenchymal disease; surgical management is deferred in patients with severe hypoxia and active chest infection. Extracorporeal membrane oxygenation is the only treatment modality left but its availability is limited to a few centers only.
Key words: Pneumatocele; Bronchopleural fistula; Ventilation; Intensive care
Citation: Samra T, Kumari K, Saini V. Ventilatory management in a child with bilateral bronchopleural fistula: A challenge for the intensivist. Anaesth Pain & Intensive Care 2016;20(2):217-220
Received: 6 January 2016; Reviewed: 2 February, 6 May 2016; Corrected: 6 May 2016; Accepted: 15 May 2016
INTRODUCTION
A bronchopleural fistula (BPF) is a communication between the pleural space and the bronchial tree. Approximately two thirds of BPFs are secondary to pulmonary resections (pneumonectomy, lobectomy) and present in the postoperative period. The remaining are due to tuberculosis, pneumonia, empyema, lung abscess and radiotherapy for lung cancers.[1]We report the challenges faced in mechanically ventilating a child with fulminant staphylococcus aureus pneumonia complicated by bilateral BPF.
CASE REPORT
A 12 year old boy presented to the medical emergency with a five day history of fever, headache and vomiting. The child was tachypneic (R.R – 40 breaths per minute), febrile (38.4°C) and had a high pulse rate (120 per min). Neck rigidity and an occasional wheeze present in lung bases (left > right) were the only findings on systemic examination. Leucopenia (WBC count of 2200/mm3) and thrombocytopenia( platelet count 8000/mm3) was reported in hematological studies. He was hypoxic with an arterial partial pressure of oxygen (PaO2) of 50 mmHg and partial pressure of carbon dioxide (PaCO2) of 45 mmHg on high flow inspired oxygen (ventimask with FiO2 of 0.5). The child was thus intubated and shifted to the intensive care unit (ICU).
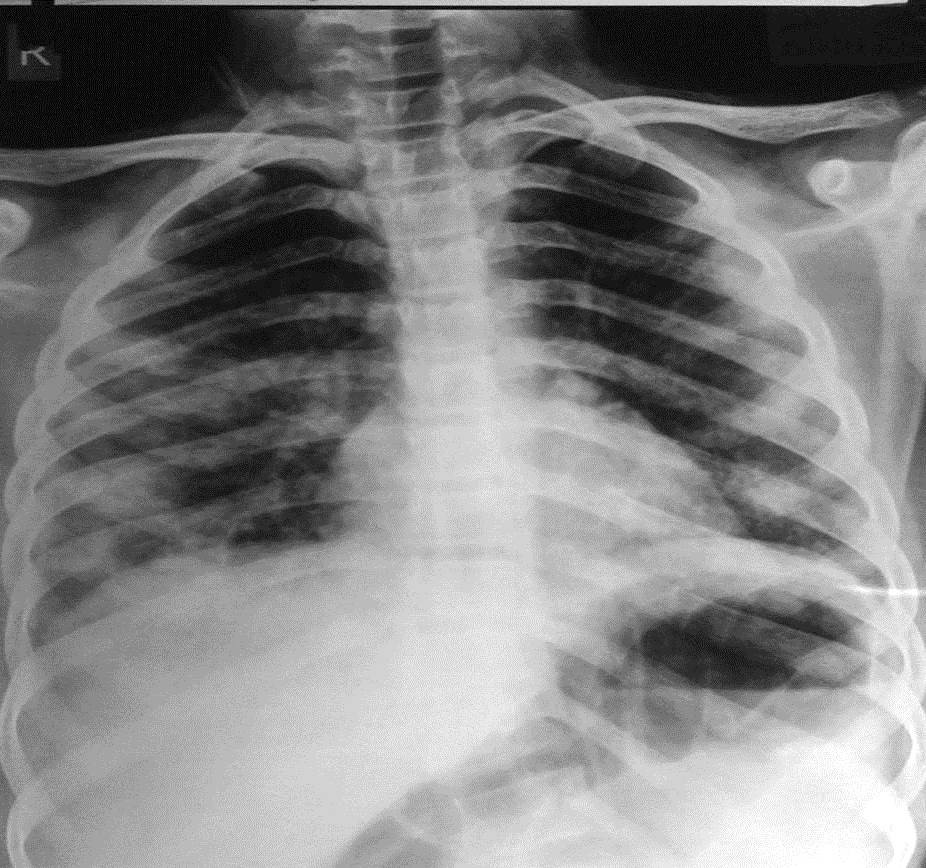
Figure 1: CXR on admission; bilateral multilobar patchy infiltrates
Bilateral multilobar patchy infiltrates were seen in chest x-ray (Figure 1). Probable diagnosis of tubercular meningitis and pneumonia was made and he was managed with antituberculosis drugs, antibiotics and ventilated with synchronous intermittent mechanical ventilatory (SIMV) mode. Staphylococcus aureus was isolated from blood culture and was sensitive to methicillin, oxacillin, netilmicin, clindamycin, vancomycin, and teicoplanin; so antibiotics were changed based on reports of culture/sensitivity. But there was no clinical improvement and HRCT Chest was done which reported multiple cavitary nodules in bilateral lungs; with a few in sub pleural location (Figure 2). Pleural fluid analysis was done and revealed a glucose level of 5mg/dl, protein fluid to serum ratio of < 0.5 with predominant polymorphs, sterile culture and ADA negative report.
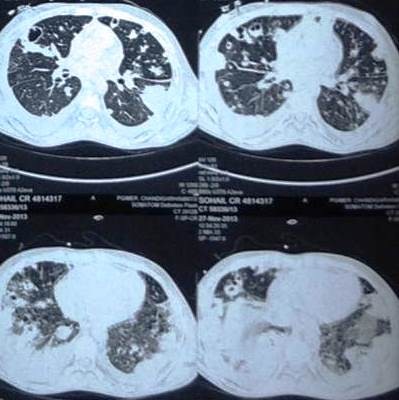
Figure2: HRCT Chest: multiple nodules with cavitation in bilateral lungs
On fourth day the child developed right followed by left pneumothorax for which bilateral intercostal drainage (ICD) was done. This was further complicated by the development of bilateral bronchopleural fistula, right followed by left. Ventilator settings were changed from SIMV to PSV (pressure support ventilation); minimum pressure support of 10 cmH2O and zero PEEP (summarized in Table 1). Left up position was done for dependent drainage as right BPF > left BPF. But loss of tidal volume through bilateral BPF resulted in increasing hypoxia and hypercarbia.
Bilateral BPF removed any possibility of one lung ventilation. Fibreoptic bronchoscopy guided direct application of sealant (cyanoacrylate, fibrin agents, Gelfoam) was planned but the presence of multiple large (> 1 cm) bilateral BPF and active chest infection on bronchoscopy was a contraindication for the procedure. Surgical management was deferred because of active chest infection and severe hypoxia. Extracorporeal membrane oxygenator (ECMO) was the only option left but it is not available in our set up. The child subsequently developed severe hypoxia (PaO2 of 40 – 50 mmHg) and hypercapnia (PaCO2 120 mmHg) and expired after 25 days of stay in the ICU.
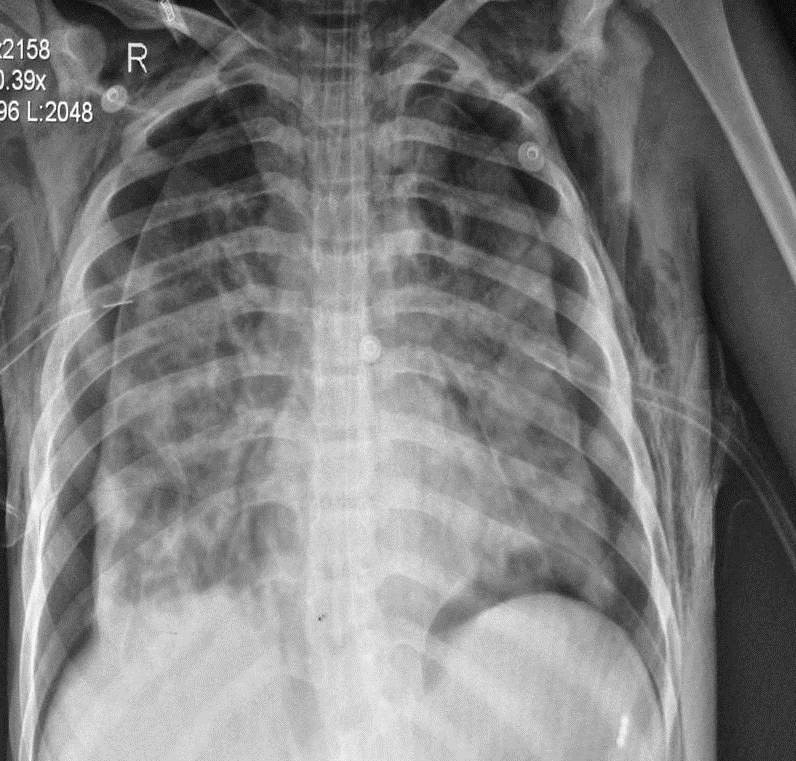
Figure 3: Bilateral pneumothorax complicating subsequently to BPF
Table 1: Ventilatory settings in patient with B/L multiple BPF: progressive development of hypoxia and hypercarbia
| Time period | Ventilator settings | PH | PaO2 | PaCO2 | HCO3 | B.E | SPO2 |
| On admission to ICU | SIMV (F/PEEP/PS) 15, 5/10 | 7.36 | 136.6 | 43.9 | 24.4 | – 1.2 | 98.9 |
| Day 2 | SIMV (F/PEEP/PS) 16, 4/10 | 7.35 | 109.3 | 59.4 | 32.5 | 5.1 | 98.0 |
| Day 4 (Development of B/L BPF) | CPAP (PEEP/PS) 2/12 | 7.31 | 151.7 | 76.2 | 37.6 | 8.1 | 99.1 |
| Day 5 | CPAP (PEEP/PS) 1/6 | 7.29 | 135.4 | 83.9 | 40 | 9.6 | 98.8 |
| Day 5 | CPAP (PEEP/PS) 0/10 | 7.41 | 140 | 62.9 | 39.3 | 11.8 | 99.0 |
| Day 10 | CPAP (PEEP/PS) 0/10 | 7.33 | 108.5 | 78.7 | 40.7 | 11.0 | 97.9 |
| Day 16 | CPAP (PEEP/PS) 0/12 | 7.31 | 60.3 | 75.5 | 41.6 | 14.4 | 91.27 |
| Day 22 | CPAP (PEEP/PS) 0/10 | 7.27 | 73.3 | 100.6 | 45.1 | 13.1 | 92.7 |
| At time of arrest
(Day 25) |
SIMV (F/PEEP/PS)12/ 2/15 | 7.11 | 41.4 | 137.7 | 42.9 | 7.7 | 58.8 |
DISCUSSION
Pulmonary pneumatoceles are thin-walled, air-filled cysts within the lung parenchyma and develop as a sequela to acute pneumonia caused by Staphylococcus aureus.[2] Seventy percent of pneumatoceles occur in children younger than 3 years and incidence of post-infectious pneumatocele in staphylococcal pneumonias can be as high as 85%.[3] Most pneumatoceles resolve spontaneously but in some rare cases may lead to complications. Cardiorespiratory compromise has been reported in a 15-month-old girl due to progressive enlargement of multiple pneumatoceles causing a tension effect which was successfully treated with percutaneous decompression using computed tomography (CT)-guided pigtail catheter placement.[4] In our case the child developed bilateral BPF as a complication of pneumatoceles.
Management of BPF in patients on mechanical ventilator is challenging as the airway pressures need to be maintained at or below the critical opening pressure of the fistula to promote healing of fistula, yet provide adequate alveolar ventilation for sufficient gas exchange.[5]Use of least possible PEEP, tidal volume, inspiratory time and number of mechanical breaths per minute minimize the airway pressures. Prognosis depends on the amount of air leak; patients with smallest air leak have the best prognosis.[6]
BPF in patients with suppurative pleuro-plumonary diseases are initially managed conservatively with dependent drainage, reduction of the pleural space, antibiotics, nutritional supplementation and adequate ventilatory management.[7] Use of chest tubes have inherent benefits and complications. It is the initial method of choice for control of tension pneumothorax and aspiration but they lead to loss of tidal volume and are a source of infection.
There are no established guidelines on the management of patients with BPF and no consensus on how to approach the problem. Thus, each case has to be individually assessed and treatment options explored. Certain treatment strategies could not be used in our patient due to the specific disease etiology. Independent lung ventilation is of no use in patients with bilateral BPF. High frequency ventilation (HFV) is useful in patients with normal lung parenchyma and proximal BPF, but it is of limited value in patients with distal and parenchymal disease.[8]Flexible bronchoscopy is a therapeutic modality in patients with smaller (< 5mm) fistula. Intrabronchial valves (Spiration IBV) serve as a noninvasive therapeutic option for the closure of BPFs in patients with persistent air leak.[9] Our patient had bilateral large BPF; fistulas bigger than 8 mm are not suitable for bronchoscopic therapy.[10] Surgical management was deferred in our patient because of active chest infection and severe hypoxia.
BPF secondary to bacterial pneumonias are associated with significant morbidity and mortality and are still a cause of BPF in children in developing countries. Treatment of life threatening complications and pleural space infection should be instituted as early as possible. The management of an immediate post-operative fistula and large BPF is surgical. ECMO is the only supportive treatment modality left in a few cases and thus should be available at all tertiary care referral hospitals.
REFERENCES
- Sonobe M, Nawkagawa M, Ichinose M, Ikegami N, Nagasawa M, Shindo T. Analysis of risk factors in bronchopleural fistula after pulmonary resection for primary lung cancer. Eur J Cardiothorac Surg 2000;18:519-23. [PubMed] [Free full text]
- Tong SY, Davis JS, Eichenberger E, Holland TL, Fowler VG Jr. Staphylococcus aureus infections: epidemiology, pathophysiology, clinical manifestations, and management. Clin Microbiol Rev. 2015;28:603-61. doi: 10.1128/CMR.00134-14. [PubMed] [Free full text]
- Kunyoshi V, Cataneo DC, Cataneo AJ. Complicated pneumonias with empyema and/or pneumatocele in children. Pediatr Surg Int. 2006 ;22:186-90. [PubMed]
- Ku SW, Yu TC, Chan KW. Decompression of multiple tension pneumatoceles in a child using computed tomography-guided percutaneous catheter placement. Can Respir J. 2011; 18: e82–e85. [PubMed] [Free full text]
- Miren A, Schinco VAF, Santora AT. Ventilatory management of a bronchopleural fistula following thoracic surgery. Respir Care 1998;43:1064-9.
- Pierson DJ, Horton CA, Bates PW. Persistent bronchopleural air leak during mechanical ventilation: a review of 39 cases. 1986;90:321-3. [PubMed]
- Slade M. Management of pneumothorax and prolonged air leak. Semin Respir Crit Care Med 2014; 35:706. doi: 10.1055/s-0034-1395502. [PubMed]
- Louis M, Noppen M. Bronchopleural fistulas: An overview of the problems with special focus on endoscopic management. Chest 2005;128:3955-65. [PubMed]
- Mahajan AK, Verhoef P, Patel SB, Carr G, Kyle Hogarth D. Intrabronchial valves: a case series describing a minimally invasive approach to bronchopleural fistulas in medical intensive care unit patients. J Bronchology Interv Pulmonol. 2012 ;19:137-41. doi: 10.1097/LBR.0b013e318251c897. [PubMed] [Free full text]
- Steiger Z, Wilson RF. Management of bronchopleural fistulas. Surg Gynecol Obst. 1984; 158:267-71.



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube