
Santhana Kannan1, Subash Sivasubramaniam1, Sudhakar Marri1
1Department of Anaesthesia, City Hospital, Birmingham, (United Kingdom)
Correspondence:Dr Santhana Kannan, Department of Anaesthesia, City Hospital, Dudley Road, Birmingham B18 7QE.(United Kingdom); Phone: 0121 5074343; Fax: 0121 5074349; E-mail: s.kannan@nhs.net
ABSTRACT
Ultrasound guided nerve block is now becoming the standard practice in regional anaesthesia and has been shown to require less volume of local anaesthetic and reduce the incidence of complications. Median, ulnar and radial nerves are the main peripheral branches of the brachial plexus. Selective blocking of these nerves allows targeted approach and retention of motor power in postoperative period. The nerves can be blocked at multiple levels in upper limb. This articles describes the indications, relevant sonoanatomy and techniques to perform the blocks and recent advances.
Keywords: Ultrasound; Peripheral nerves; Brachial Plexus; Median nerve;Ulnar nerve; Radial nerve; Spinal Nerves; Anesthesia, Conduction; Nerve block
Citation: Kannan S, Sivasubramaniam S, Marri S. USG for upper limb peripheral nerve blocks. Anaesth Pain & intensive Care 2015;19(3):341-347
INTRODUCTION
Peripheral regional anesthesia and analgesia offers several advantages over traditional methods of analgesia [1, 2]. Ultrasound guided(USG) regional nerve blocks is safe and requires smaller volumes of local anesthetic allowing the practitioner to target specific nerves when required [3,4]. When compared to nerve stimulation technique, USG blocks are more effective, cause less pain during the procedure (in awake patients) and have reduced rate of vascular puncture [5]. This article focuses on USG upper limb peripheral nerve blocks (ULPNB), relevant sonoanatomy, technique, tips and recent advances. It will not cover the pharmacological aspects in terms of drug choice and adjuvants. USG blocks of brachial plexus is addressed elsewhere in this issue.
ULPNB better preserve motor function without negatively affecting quality of anesthesia, leading to increased patient satisfaction, when compared to brachial plexus block.[6]Indications of ULPNB include anesthesia or analgesia below elbow, and rescue after an inadequately effective brachial plexus block. Many procedures of upper limb may need tourniquet. It is important to remember that ULPNB alone will not cover the tourniquet pain and brachial plexus block will need to be considered. A combination technique of brachial plexus motor block using a short acting higher concentration local anesthetic and ULPNB using dilute concentration of long acting agents allows reducing the duration of motor block and prolonging analgesia postoperatively.[7]
ANATOMY
The three main peripheral branches of the brachial plexus are the median nerve, radial nerve and the ulnar nerve. In 1999, it was shown that ultrasonography using a 7.5 MHz probe allowed reliable imaging of the major arm nerves.[8] The upper limb main peripheral nerves were about 3 mm thick and the size did not correlate with subjects’ height, weight or ageassuring consistency of the nerve thickness.Arterial variants immediately adjacent to the median nerve may occur in approximately 1 in 5 limbs, which can potentially influence the block technique and outcome.[9]Although pregnancy increases median nerve susceptibility to lidocaine, the volume of local anesthetic required may not be significantly lowered.[10]
Moldovan et al found that lignocaine induced median nerve block caused a transient conduction failure that recovered completely by 3 h, whereas excitability recovered fully by 24 h.[11] The seven fold increase in threshold after complete recovery of conduction was associated with excitability changes that could only partially be explained by block of the voltage-gated Na+ channel. The data suggest that lignocaine, even at clinical ‘sub-blocking’ concentrations, could cause a reversible structural impairment of the axolemma. As the incidence of symptomatic long term neurological damage is low, the significance of these findings is not clear.A median nerve block can also cause reduced force production by those muscles not supplied by itindicating that the block can ‘spill’ over to the areas of other peripheral nerves leading to blocking of those segments as well.[12]
ULTRASOUND PRINCIPLES
Based on echogenicity, a structure can be characterized as hyperechoic (white on the screen), hypoechoic (gray on the screen) and anechoic (black on the screen).[3] Upper limb peripheral nerves appear as bright hyperechoic structures with a honeycomb texture on transverse or cross section scan. The blood vessels are hypoechoic similar to any injected local anesthetic solution. However, the latter shadow expands during injection. The peripheral nerves of upper limb are in close proximity to major blood vessels at some points. Use of Doppler feature in the USG machines will help to identify a blood vessel when in doubt. If there is resistance to injection, it warrants withdrawal of the needle to avoid intra-neural injection and potential damage. Until one gains experience of the sonographic appearance and location of the nerve structures, it would not be unreasonable to use a nerve stimulator in combination with USG guidance. It must be noted that nerve stimulation in an awake patient is painful and should be avoided if possible. Nerve stimulation technique to block median nerve was not observed to prevent intraneural injection. However, it did not necessarily translate to an increased incidence of observed nerve injuries.[14]
Ligaments and tendons appear hyperechoic similar to distal nerves but do not havethe “honeycomb” pattern. For confirmation, one can trace the “target structure” proximally or distally in order to distinguish the nerve from a tendon based on anatomy (the tendon will be traceable to the muscle body).For e.g., multiple round fibrinous structures are identified superficial to the carpal bones representing the tendons and median nerve in the carpal tunnel. Fanning or rocking the probe will change the appearance of these structures from hypo-echoic to hyper-echoic. This effect is term ‘anisotropy’ and is more apparent in tendons than in nerves. The median nerve is identified by its less dramatic anisotropy and lack of movement with flexion and extension of the digits.
The block technique is usually described as ‘in plane’ or ‘out of plane’ approach. ‘In plane’ is where the USG beam is parallel to the needle. This allows visualization of the length of the needle. Out of plane approach is similar to transverse section where only a cross section of the needle is visible. Note that one can place the probe in such a way that the nerve in question is visualized in a cross sectional view but the needle is inserted parallel to the beam. The in plane terminology only applies to the relation of the needle to the USG beam and not the nerve being visualized. For all ULPNB blocks, a linear (e.g. 38 mm) high frequency probe [8 -12 MHz] and a 50 mm long needle is recommended. Although the nerves are located close to the skin for most part, a longer needle is required for an in-plane approach. The principles of patient selection are similar to other regional nerve blocks in terms of consent, expertise of the operator and duration of procedure etc. Similarly, the principles of probe choice, sterility and ergonomics should be followed. USG regional anesthesia, when employed by clinicians experienced in its use, may decrease the incidence of vascular puncture, and may therefore make procedures safer in the presence of altered coagulation [15]. The benefits vs. risks of administering must be assessed on an individual patient basis. Volar aspect compartment syndrome has been reported after median nerve block in a patient who was systemically anticoagulated but the block was not conducted under ultrasound guidance [16].
Marhofer et al evaluated the correlation of spread of local anesthetic and effectiveness in a volunteer study involving USG median nerve block [17]. Complete circumferential spread of local anesthetic was achieved in two thirds of subjects where it was intended and in a third where it was not. Block success rate was similar at 90% and independent of whether circumferential or non-circumferential spread of the local anesthetic was achieved. Hence, a circumferential injection of local anesthetic is not essential for ULPNB. However, the onset of sensory block was faster with circumferential spread of local anesthetic. Hydrodissection is a technique where a small volume of liquid is used to separate the nerve if it lying too close to a vital structure. Median nerve block effectiveness was not reduced when circumferential perineuralhydrodissection with 5% dextrose preceeded local anesthetic injection during USG procedure.[18]
MEDIAN NERVE
The median nerve is a mixed sensory and motor nerve that is formed from the medial and lateral cords of the brachial plexus. It travels in a neurovascular bundle in the upper arm and lies medial to the brachial artery as it passes through the cubital fossa in the elbow and where it can be blocked.Distal to the elbow, the median nerve gives off the anterior interosseous nerve, which supplies the deep volar muscles of the forearm. Blocking the median nerve at the elbow leads to greater paralysis without greater distribution of anesthesia.In the forearm, the nerve is found between the muscle bodies of the flexor digitorumsuperficialis and flexor digitorumprofundus before passing through the carpal tunnel in the wrist. Its motor branches supply the deep volar muscles in the forearm and thenar eminence of the hand. Its sensory distribution is limited to the lateral two thirds of the palm on ventral surface.Median nerve blockade is useful for procedures involving the anterolateral surface of the hand, including the thumb through middle finger.
Sono-anatomy and technique
The block can be done at the antecubital fossa or the anterior aspect of the mid forearm. The brachial artery is the landmark for median nerve blockade at the antecubital fossa (Figure 1). The nerve is visualised medial to the artery. The block can be performed with an out of plane approach. With the arm extended and externally rotated, the probe is placed transversely over the brachial artery pulse. Once the brachial artery is identified, depth is adjusted to visualize the area just deeper to the artery. The brachial vein location in relation to the artery may vary and a tourniquet will aid in identifying it. 3 – 4 ml of local anesthetic is usually sufficient.
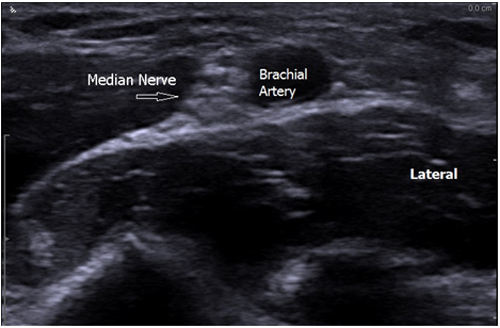
Figure 1: Median nerve at the level of elbow medial to the brachial artery.
Lower down in the forearm, the median nerve appears as an oval or circular structure between the flexor digitalis superficial and flexor digitalis profundus muscles (Figure 2). Its classic honeycomb appearance should stand out against the surrounding hypoechoic muscle. If the nerve is difficult to identify, it may be traced from the carpal tunnel. The median nerve will persist when followed, unlike the tendons on the carpal tunnel, which will transition into muscle bodies.
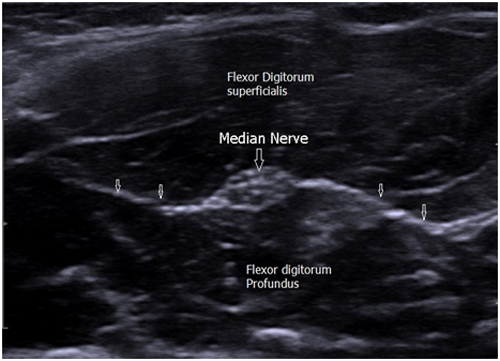
Figure 2: Median nerve at the level of forearm between the two muscle bellies. The small arrows indicate the fascial plane separating the two muscles
At the level of wrist, the carpal tunnel is seen beneath flexor retinaculum, but the tendons being highly anisotropic are not clearly visible [19]. The ulnar nerve and artery lie outside and medial to the carpel tunnel. As with the landmark based technique, the median nerve can be blocked in the carpal tunnel. This site has the same sensory distribution, but spares paralyzing the forearm muscles. Given the very superficial lie of the median nerve in the carpal tunnel, an out of plane approach is generally preferred. Use of a small volume of local anesthetic is important to negate the theoretical risk of compartment syndrome.
ULNAR NERVE BLOCK
The ulnar nerve originates from the C8-T1 nerve roots, which form part of the medial cord of the brachial plexus. It is a mixed sensory and motor nerve providing sensory innervation to the medial aspect of the hand. It descends on the posteromedial aspect of the humerus and enters the flexor compartment of the forearm by passing between the olecranon and medial epicondyle of the humerus (“cubital tunnel”) and through the two heads of the flexor carpi ulnaris. The nerve then travels near the ulnar bone and medial to the ulnar artery in the distal forearm. About 5 to 10 cm proximal to the wrist, dorsal and palmar cutaneous branches split and provide innervation to the medial aspect of the hand. Artery and nerve are found deep to the tendon of the flexor carpi ulnaris and enter the palm superficial to the flexor retinaculum, via the ulnar canal.
Sonoanatomy and technique
The ulnar nerve can be blocked proximal to or at the level of elbow, the mid forearm or the wrist. The nerve is easily located in the groove between the olecranon and the medial epicondyle. The probe orientation should be transverse and needle orientation in-plane. However, as the ulnar nerve can be compressed in the poorly compliant cubital tunnel by large volumes of local anesthetic, injections at this site should be limited to 3–5 ml to minimize the risk of a compartment syndrome. There have been no reports of ulnar nerve injury attributable to USG block at this site. With an overall very low incidence of 0.037%, ulnar nerve is still the most common peripheral nerve injured perioperatively due to external pressure[20]. If a nerve block is performed at this site in a patient undergoing a procedure under general anesthesia, it may be difficult to argue that the nerve block did not contribute to injury.To avoid this risk completely, the ulnar nerve can be blocked several centimetresabove the elbow. The nerve is identified in the cubital tunnel and traced proximally into the distal or mid-upper arm. At this site the nerve is superficial and surrounded by soft tissue.
Another convenient area for blockade of the ulnar nerve is the mid-forearm (Figure 3). This location combines the ease of visualization, ability to block all terminal branches and minimal potential for vascular injury. One can trace the ulnar artery proximally until the nerve becomes visible in the mid-forearm located medial to the vessel. Blockade at this level may also improve chances of providing anesthesia of the dorsal and volar sensory branches of the ulnar nerve, which branch out about 5 cm above the wrist.
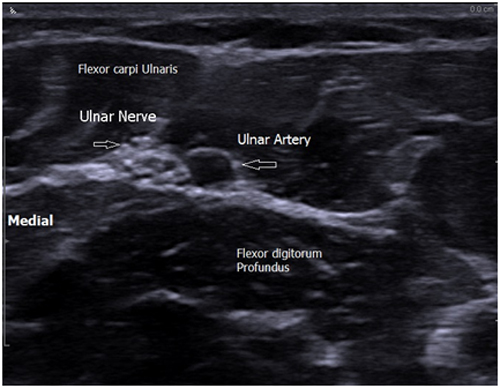
Figure 3: Ulnar nerve at the forearm level medial to the ulnar artery.
In the wrist, the hyperechoic appearing ulnar nerve continues to bemedial to the artery between the vessel and the flexor carpi ulnaris at the level of the proximal volar skin crease. This approach can spare the dorsal and volar sensory branches of the ulnar nerve. A superficial ulnar artery may join the ulnar nerve as distal as the wrist and complicate anatomical orientation.The nerve is blocked with an out of plane approach usually with 3- 4 ml of the local anesthetic.
RADIAL NERVE BLOCK
The radial nerve is a mixed sensory and motor nerve that arises from the posterior cord of the brachial plexus. It travels in the spiral groove of the humerus in the upper arm and descends anterior to the lateral epicondyle in the elbow. At the elbow it divides into the superficial branch, which provides cutaneous innervation to part of the hand, and the deep branch, which innervates the dorsal compartment of the forearm. The superficial branch travels with the radial artery in the mid-forearm, but divides away from the artery in the distal forearm as it separates into smaller cutaneous branches.
Sono-anatomy and technique
Radial nerve location was assessed in 50 adult volunteers using ultrasound guidance [21]. Three points were defined: A, midway between the anterior process of the acromion and lateral epicondyle of the humerus; B, one third of the distance between A and the lateral epicondyle; C, two thirds of the distance between A and the lateral epicondyle At point B, the radial nerve lay in the spiral groove of the humerus, closely associated with the profundabrachii artery and vein. At point C, the nerve had passed through the lateral intermuscular septum and lay between brachioradialis and brachialis muscles. In 99% of arms, the radial nerve was not visible at point A, but became visible between points A and B in 93% of arms. The depth at point B was significantly less (about 1.2 cm) than at point C (about 1.7 cm) (Figure 4). Not surprisingly, the depth of the nerve positively correlated with body mass index and with arm circumference. The radial nerve was oval-shaped at both sites. It was concluded that Points B and C may represent convenient sites for ultrasound-guided radial-nerve block where the nerve is clearly visualized and has not yet divided into superficial and deep branches. Point C may be the optimal site for radial-nerve block because of the smaller risk of vessel puncture. Blocking the nerve more proximal (level of upper or mid-humerus) assures a larger area of anesthesia.
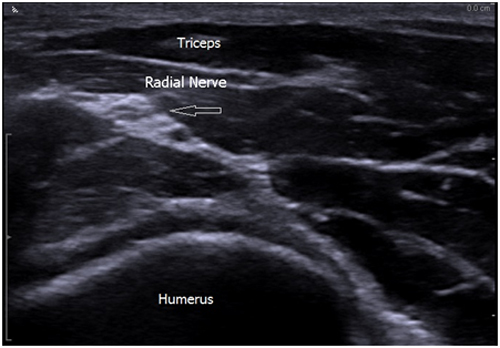
Figure 4: Radial nerve above the elbow. Note the proximity to the humerus. Triceps is on the top as it is the structure closest to the probe when it is positioned from behind the arm.
At the elbow, the radial nerve lies between the brachialis and brachioradialis muscles, above the lateral epicondyle, 1 to 2 cm lateral to the biceps tendon, which is a landmark. The radial nerve block at this level provides sensory anesthesia to the dorsolateral aspect of the hand (thumb, index, middle, and lateral half of the ring finger) up to the distal interphalangeal joint. The brachial artery is medial to the nerve at the cubital fossa. The radial nerve can also be found sonographically at the level of mid forearm by tracing the radial artery from distal to proximal where the cutaneous branches of the radial nerve unite lateral to the artery.
OTHER USES OF PNB IN UPPER LIMB
Apart from anesthesia and postoperative analgesia, ultrasound-guided ulnar nerve catheter placement has been reported in the forearm for post-operative pain relief following arthrolysis and tenolysis of the fifth finger. The ulnar nerve catheter allowed for excellent pain relief and completely painless physiotherapy without impairing motor function of the operated finger [22]. USGmedian nerve perineural catheter placement and local anesthetic infusion for 11 days has been reported to successfully facilitate intensive hand rehabilitation in a patient with chronic postoperative hand pain unresponsive to systemic opioids.[23] Median nerve catheter in combination with infraclavicular block has also been used for hand rehabilitation [24].Ultrasound was used in that patient to locate the median nerve at the mid-forearm level. This site was chosen to ensure thatthe catheter would be placed adequately distal to the branching point of the anterior interosseous nerve to minimize potential motorblockade due to retrograde flow of local anesthetic. USG median nerve block increases the velocity of blood flow in radial artery but not the diameter.[25] In that study, the authors found that the radial artery cannulation was painless and the guidewire insertion met with some more resistance than usual, presumably relating to high blood flow velocity.Dermatologists also use peripheral nerve blocks to excise simple lesions.[26]
Median and ulnar nerve block anesthesia at the wrist for prevention of procedural pain associated with injections into the palmar hand for trigger finger, palmar flexor tenosynovitis, and Dupuytren contracture was associated with 56% reduction in pain and increased patient satisfaction.[27] It has been shown that attending physicians, fellows, and residents in an Emergency department can perform forearm ultrasonography-guided nerve blocks of the radial, ulnar, and median nerves quickly, without additional anesthesia and with high patient satisfaction, after minimal training.[28] They were done to provide anesthesia for hand procedures in Emergency department. Peripheral nerve block has been used in botulinum toxin treatment for palmar plantar hyperhidrosis.[29]
PEDIATRICS
In a prospective non blinded descriptive study of ultrasound-guided ulnar, median, and radial nerve blocks in a convenience sample of pediatric patients with hand injuries requiring procedural intervention, it was found that the time to completion of nerve blocks was less than two minutes in the majority [30]. No immediate complications, including vascular puncture, carpal tunnel injury, or direct nerve injection, were noted. At 1-year follow-up, no adverse effects were reported.
FUTURE POSSIBILITIES
Three-dimensional, multiplanar ultrasound is already in use in obstetrics. In the near future, real-time 3 D ultrasound has the potential to improve nerve identification and accuracy of needle placement in regional anesthesia [31].
SUMMARY
In summary, USGULPNB blocks is becoming the standard of practice in both adults and children. It has been shown to be more effective, have less incidence of complications and is quicker to perform. There are different approaches to ULPNB block available depending upon the need with each having its advantages and disadvantages. The user needs to be aware of pitfalls of using USG guidance as certain structures look very similar.
Role of authors
SK: did the literature search, labelled the images and revised the manuscript.
SS: provided the draft version of manuscript and images.
SM: provided the draft version of manuscript and images
REFERENCES
- McCartney JL, Lin L, Shastri U. Evidence basis for the use of ultrasound for upper-extremity blocks. RegAnesth Pain Med 2010 Mar;35(2):S10–5 [PubMed] doi: 10.1097/AAP.0b013e3181d25675.
- Nielsen KC, Steele SM. Outcome after regional anaesthesia in the ambulatory setting—is it really worth it? Best Pract Res ClinAnaesthesiol 2002 Jun;16(2):145–57 [PubMed]
- Orebaugh SL, Kentor ML, Williams BA. Adverse outcomes associated with nerve stimulator-guided and ultrasound-guided peripheral nerve blocks by supervised trainees:update of a single-site database. RegAnesth Pain Med. 2012 Nov;37(6):577–82. [PubMed] [Free full text] doi: 10.1097/AAP.0b013e318263d396.
- Kessler J, Marhofer P, Hopkins PM, Hollmann MW. Peripheral regional anaesthesia and outcome:lessons learned from the last 10 years. Br J Anaesth 2015 May;114(5):728–45. [PubMed] doi: 10.1093/bja/aeu559.
- Munirama S, McLeod G. A systematic review and meta-analysis of ultrasound versus electrical stimulation for peripheral nerve location and blockade. Anaesthesia 2015 Sep;70(9):1084–91. [PubMed] [Free full text] doi: 10.1111/anae.13098.
- Lam NCK, Charles M, Mercer D, Soneru C, Dillow D, Jaime F, et al. A triple-masked, randomized controlled trial comparing ultrasound-guided brachial plexus and distal peripheral nerve block – Anesthesia for outpatient hand surgery. Anesthesiol Res Pract. 2014;2014:324083. [PubMed] [Free full text] doi: 10.1155/2014/324083.
- Smith BE, Challands JF, Suchak M, Siggins D. Regional anaesthesia for surgery of the forearm and hand. A technique of combined supraclavicular and discrete blocks. Anaesthesia 1989 Sep;44(9):747-9. [PubMed] [Free full text] doi/10.1111/j.1365-2044.1989.tb09261.x.
- Heinemeyer O, Reimers CD. Ultrasound of radial, ulnar, median and sciatic nerves in healthy subjects and patients with hereditary motor and sensory neuropathies. Ultrasound Med Biol 1999 Mar;25(3):481-5. [PubMed]
- Stimpson, JA, Gupta A. Persistent median artery (palmar type) and median nerve block in the forearm: observational study of prevalence.Regional Anesth Pain Med. 2012 Sep;37(5):558-60. [PubMed]doi: 10.1097/AAP.0b013e318260e458.
- Butterworth, JF IV. Walker FO, Lysak S. Pregnancy increases median nerve susceptibility to lidocaine.Anesthesiology. 1990 Jun;72(6):962-5. [PubMed] [Free full text]
- Moldovan, M, Lange KHW, Aachmann-Andersen NJ, Kjaer TW, Olsen NV, Krarup C. Transient impairment of the axolemma following regional anaesthesia by lidocaine in humans.Journal of Physiology. 2014 July;592(13):2735-50. [PubMed] [Free full text] doi: 10.1113/jphysiol.2014.270827.
- Li ZM, Harkness DA, Goitz RJ. Thumb force deficit after lower median nerve block. J NeuroengineeringRehabil. 2004 Oct;1(1):3. [PubMed] [Free full text] doi: 1186/1743-0003-1-3
- Hadzic A. Ultrasound-guided IS brachial plexus block. In:Hadzic A, Carrera A, Clark T, et al. Hadzic’s peripheral nerve blocks and anatomy for ultrasound-guided regional anesthesia, 2nd ed. New York:The McGraw-Hill Companies, Inc. 2012:353.
- Dufour E, Cymerman A, Nourry G, Balland N, Couturier C, Liu N, et al. An ultrasonographic assessment of nerve stimulation-guided median nerve block at the elbow:a local anesthetic spread, nerve size, and clinical efficacy study. AnesthAnalg. 2010 Aug;111(2):561-7. [PubMed] doi: 10.1213/ANE.0b013e3181e3a06f.
- Association of Anaesthetists of Great Britain and Ireland, Obstetric Anaesthetists’ Association and Regional Anaesthesia UK. Regional anaesthesia and patients with abnormalities of coagulation. Anaesthesia 2013 Sep;68(9):966-72. [PubMed] [Free full text] doi: 10.1111/anae.12359.
- Parziale JR, Marino AR, Herndon JH. Diagnostic peripheral nerve block resulting in compartment syndrome:case report. Am J Phys Med Rehabil. 1988 Apr;67(2):82-4. [PubMed]
- Marhofer D, Karmakar MK, Marhofer P, Kettner SC, Weber M, Zeitlinger M. Does circumferential spread of local anaesthetic improve the success of peripheral nerve block? Br J Anaesth. 2014 Jul;113(1):177-85. [PubMed] [Free full text]doi: 10.1093/bja/aeu002.
- Dufour E, DonatN ,Jaziri S, Kurdi O, Couturier C, Dreyfus JF, et al. Ultrasound-guided perineural circumferential median nerve block with and without prior dextrose 5% hydrodissection:a prospective randomized double-blinded noninferiority trial. AnesthAnalg. 2012 Sep;115(3):728-33. [PubMed] doi: 10.1213/ANE.0b013e31825fa37d
- McCahon RA, Bedforth NM. Peripheral nerve block at the elbow and wrist. ContinEducAnaesthCrit Care Pain 2007;7(2):42– 4. [Free full text] doi: 10.1093/bjaceaccp/mkm005.
- Lalkhen AG, Bhatia K. Perioperative peripheral nerve injuries. ContinEducAnaesthCrit Care Pain. 2012;12(1):38 – 42. [Free full text] doi: 10.1093/bjaceaccp/mkr048.
- Foxall, GL, Skinner D, Hardman JG. Bedforth NM. Ultrasound anatomy of the radial nerve in the distal upper arm. RegAnesth Pain Med. 2007 May;32(3):217-20. [PubMed]
- Lurf M, Leixnering M. Ultrasound-guided ulnar nerve catheter placement in the forearm for postoperative pain relief and physiotherapy.ActaAnaesth Scand. 2009 Feb;53(2):261-3. [PubMed] [Free full text] doi: 10.1111/j.1399-6576.2008.01762.x.
- Maxwell BG, Hansen JA, Talley J, Curtin CM, Mariano ER. Ultrasound-guided continuous median nerve block to facilitate intensive hand rehabilitation. Clin J Pain. 2013 Jan;29(1):86-8. [PubMed] doi: 10.1097/AJP.0b013e318246d1ca.
- Holman AE, Sharma B, Modest VE. Targeted ultrasound-guided double catheters (infraclavicular-brachial plexus, median nerve) facilitate hand rehabilitation with superb analgesia and motor function retention. Open J Anesthesiology, 2015 Jul;5(7):142-148. [Article online] doi: 4236/ojanes.2015.57026
- Badal JJ, Kiesau A, Boyle P. Effects of median nerve block on radial artery diameter and peak velocity. Local RegAnesth. 2010;3:5–10. [PubMed] [Free full text]
- Davies T, Karanovic S, Shergill B. Essential regional nerve blocks for the dermatologist: Part 2. ClinExpDermatol. 2014 Dec;39(8):861–7. [PubMed] [Free full text] doi: 10.1111/ced.12426.
- Sibbitt WL. Jr, Michael AA, Poole JL, Chavez-Chiang NR, DeLea SL, Bankhurst AD. Nerve blocks at the wrist for painful injections of the palm.J ClinRheumatol. 2011 Jun;17(4):173-8. [PubMed]doi: 10.1097/RHU.0b013e31821bfed0.
- Liebmann O, Price D, Mills C, Gardner R, Wang R, Wilson S, et al. Feasibility of forearm ultrasonography-guided nerve blocks of the radial, ulnar, and median nerves for hand procedures in the emergency department. Ann Emerg Med. 2006 Nov;48(5):558–62. [PubMed]
- Fujita M, Mann T, Mann O, Berg D. Surgical Pearl:Use of nerve blocks for botulinum toxin treatment of palmar-plantar hyperhidrosis.J Am AcadDermatol. 2001 Oct;45(4):587-9. [PubMed]
- Frenkel O, Liebmann O, Fischer JW. Ultrasound-guided forearm nerve blocks in kids:a novel method for pain control in the treatment of hand-injured pediatric patients in the emergency department.PedEmerg Care. 2015 Apr;31(4):255-59. [PubMed] doi: 10.1097/PEC.0000000000000398.
- Foxall GL, Hardman JG, Bedforth NM.Three-dimensional, multiplanar, ultrasound-guided, radial nerve block.RegAnesth Pain Med. 2007 Nov;32(6):516-21. [PubMed]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube