
Santhana Kannan1, Sudhakar Marri1, Subash Sivasubramaniam1
1Department of Anesthesia, City Hospital, Birmingham(United Kingdom)
Correspondence:Dr Santhana Kannan, Department of Anesthesia, City Hospital, Dudley Road, Birmingham B18 7QE.(United Kingdom); Phone: 0121 5074343; Fax: 0121 5074349; E-mail: s.kannan@nhs.net
ABSTRACT
Ultrasound guided nerve block is now becoming the standard practice in regional anesthesia and has been shown to require less volume of local anesthetic and reduce the incidence of complications.Brachial plexus block can be approached via interscalene, supraclavicular, infraclavicular or axillary routes. Each of these approaches have their individual advantages and risk. This articles describes the indications, relevant sonoanatomy and techniques to perform the blocks and recent advances.
Keywords: Ultrasonography;Nerve block;Anesthesia, Conduction; Brachial plexus; Brachial plexus block; Brachial plexus; Brachial plexus anesthesia
Citation: Kannan S, Marri S, Sivasubramaniam S. USG for brachial plexus block. Anaesth Pain & intensive Care 2015;19(3):333-340
INTRODUCTION
Peripheral regional anesthesia and analgesia offer several advantages over traditional opioid based analgesia.[1, 2] There is increasing evidence that ultrasound(USG) guided regional nerve blocks are safe [3] and require smaller volumes of local anesthetics.[4] It also allows the practitioner to target specific nerves when required. When compared to peripheral nerve stimulation technique, USG guidance was more effective, caused less pain during the procedure (in awake patients) and had reduced rate of vascular puncture.[5]This article focuses on USG guided blocks of the brachial plexus (BP), relevant sonoanatomy, technique, tips and recent advances. It will not cover the pharmacological aspects in terms of drug choice and adjuvants. USG guided blocks of other nerves of upper limb is addressed elsewhere in this special issue.
BP block was introduced into clinical practice by Kulenkampff in 1911.[6]In 1978, La Grange described the use of the Doppler probe to identify arteries and the BP.[7]Fifteen years later, Kapral et al expanded that idea with the first described USGguided BP block.[8]Interestingly, CT guided BP block was being used in selected patients until much later [9].Vincent Chan then described the use of both USG and nerve stimulation to perform BP block [10].
ANATOMY
BP innervates almost whole of the upper limb. Hence, blocking the BP soon after its formation will lead to anesthesia of most of the upper limb. BP is identified by nerve roots and trunks in the interscalene (IS) region, divisions in the supraclavicular (SC) region, cords in the infra-clavicular (IC) region and individualnervebranches in the axillary region (Figure 1).It is formed by the ventral (or anterior) primary rami of C5-T1 spinal nerves. The BP lies in the posterior triangle of the neck along the posterior border of the sternocleidomastoid muscle emerging from the IS groove between the anterior and medialscalenemuscles. This is the location to perform the IS block as described later. The five roots of the plexus emerge and unite to form three trunks. These structures are named as upper, middle and lower trunks by their anatomical position. The upper two roots (C5, 6) form the upper trunk, the middle root (C7) the middle trunk, and the lower two roots (C8, T1) form the lower trunk. Behind the middle of the clavicle, each trunk divides into two divisions– anterior and posterior.
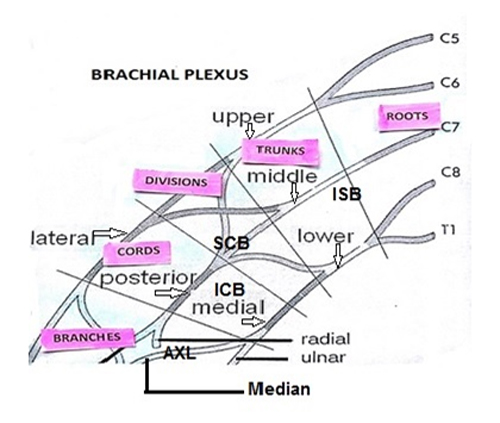
Figure 1: Formation of the brachial plexus. The approximate site of the block is indicated.
[ISB Interscalene block, SCB Supraclavicular block, ICB Infraclavicular block, AXL Axillary block]
The three posterior divisions join to form the posterior cord, the anterior division of the upper and middle trunk form the lateral cord and the anterior division of the lower trunk continues as the medial cord. The names of the cords is based on their relation to the axillary artery. The nerves originating from the cords are enclosed with the artery in a neurovascular sheath, the axillary sheath. It is a multi-compartmental structure formed by thin layers of fibrous tissue with discrete fascial septae. Nerves are enmeshed in this tissue creating individual fascial compartments for each of them.[11]These compartments could potentially limit the circumferential spread of injected solutions, thereby requiring separate injections into each compartment for maximal nerve blockade.The literature evidence is conflicting whether a single injection into the sheath will suffice or multiple injections are necessary [12]. Proximity to the vessel also increases the risk of vascular puncture.
The subclavian artery is a useful landmark in case of doubt in SC region. The BP lies superoposterolateral to the artery just above the clavicle. The complex branching and unification of the roots and divisions also means that a given peripheral nerve has multiple spinal root origins. For e.g. while blocking of the upper trunk alone will not completely cover the musculocutaneous nerve which has origins in C 5,6 and 7, it should cover the axillary nerve which has fibres from C 5, 6 only. Ulnar nerve has origins from C 8 – T1, which means a block of lower trunk should suffice. A lower root origin of ulnar nerve also means that IS block fails to block it in 50% of patients [13]. Nerves such as median (C6 – T1) and radial (C5 – T1) have wider origins and need all the trunks to be blocked. There is anatomical variation in about 12% of the patients where a given nerve may have a branch from a different root etc.[14] This may lead to partially effective blocks if only selected branches are targeted. The type of block depends upon the nature of surgery (Table 1).
Table 1: Choosing the block
|
Approach |
Level |
Surgical site |
| Interscalene | Roots / Trunks | Shoulder, upper arm, elbow |
| Supraclavicular | Trunks, Proximal divisions | Arm and forearm |
| Infraclavicular | Cords | Forearm, wrist, hand |
| Axillary | Individual nerves | Forearm, wrist, hand |
A few nerves that are not part of the brachial plexus are important because they may not be covered by BP blockade [11]. The SC nerves (C3- C4) provide sensory innervation to the “cape area” encompassing the shoulder. The intercostobrachial nerve originates from the second thoracic ventral rami (T2) and with the medial cutaneous nerve, innervates the upper inner arm.
USG PRINCIPLES
Based on echogenicity, a structure can be characterized as hyperechoic (white on the screen), hypoechoic (gray on the screen) and anechoic (black on the screen) [15]. Proximal nerves are hypoechoic (dark with a white rim) round structures, which are similar to blood vessels but neither collapsible nor pulsatile. This is important since it is not too difficult to assume an adjacent blood vessel to be the nerve trunk, for e.g. BP and vertebral artery. Use of Doppler feature in the USG machines will help to identify a blood vessel when in doubt. Any injected local anesthetic solution will appear as hypoechoic shadow which expands during injection. If there is resistance to injection, it warrants withdrawal of the needle to avoid intra-neural injection and resultant damage.This is in contrast to appearance of smaller and peripheral nerves which are predominantly bright hyperechoic structures with a honeycomb texture on transverse or cross section scan.Until one gains experience of the sonographic appearance and location of the nerve structures, it would not be unreasonable to use a nerve stimulator in combination with USG guidance. It must be noted that nerve stimulation in an awake patient is painful and should be avoided if possible. Ligaments and tendons have a similar appearance to distal nerves (hyperechoic, but do not have “honeycomb” appearance). For confirmation, one can trace the “target structure” proximally or distally in order to distinguish the nerve from a tendon based on anatomy (the tendon will be traceable to the muscle body).
The block technique is usually described as ‘In plane’ or ‘out of plane’ approach. ‘In plane’ is where the USG beam is parallel to the needle. This allows visualization of the length of the needle. Out of plane approach is similar to transverse section where only a cross section of the needle is visible. Note that one can place the probe in such a way that the nerve in question is visualized in a cross sectional view but the needle is inserted parallel to the beam. The in plane terminology only applies to the relation of the needle to the USG beam and not the nerve being visualized.For all BP blocks, a linear (e.g. 38 mm) high frequency probe (8-12MHz) and a 50 mm long needle is recommended. The principles of patient selection are similar to other regional nerve blocks in terms of consent, expertise of the operator and duration of procedure etc. Similarly, the principles of probe choice, sterility and ergonomics should be followed. USG guided regional anesthesia, when employed by clinicians experienced in its use, may decrease the incidence of vascular puncture, and may therefore make procedures such as SC blocks safer in the presence of altered coagulation [16]. USG guided BP block is not contraindicated in presence of coagulopathy. The benefits vs. risks of administering must be assessed on an individual patient basis.
INTERSCALENE BP BLOCK
The roots of the BP are found in the IS groove between the anterior and middles scalene muscles at the level at the cricoid cartilage. The IS groove is located lateral to the anterior scalene muscle and deep to the sternocleidomastoid muscle. The phrenic nerve crosses the scalaneus anterior muscle and lies between that muscle and sternomastoid. Hence there is a risk of unilateral diaphragmatic palsy as a complication of this block if the local anesthetic is injected incorrectly. Theincidence of phrenic nerve palsy with SC block was 67% three decades ago [17]. However, recent studies put the incidence closer to 17% [18]. The use of USG guidance canalmost eliminate it [19] which could be very useful should a bilateralSC block be needed [20]. Deep to the plexus at the level of the cricoid is the transverse process of the C6 along with the vertebral artery. Hence, injection of local anesthetic into the vertebral artery is a known complication leading to local anesthetic toxicity. The proximity to the epidural space leads to risk of intracranial spread of local anesthetic, if it is injected near to the nerve root as it is emerging from neural foramen or adjacent to transverse process.
Sonoanatomy:
Although the BP is typically only 12 – 20 mm (1 to 2 cm) deep from the skin, a 50 mm needle is required for the in-plane approach. The nerve roots are visible as hypo echoic round structures between scalene muscles at the level of the cricoid cartilage. Concurrent use of nerve stimulator results in deltoid or biceps contraction. Contraction of the diaphragm indicatesphrenic nerve stimulation and antero-medial placementof the needle tip. Trapezius musclestimulation indicates needle placement is tooposterior.
Technique:
Position the patient supine with head turned slightly to the opposite side. Visualize the carotid and internal jugular vein at the level of the cricoid. Identify the sternomastoid muscle superficial to the vessels and move the probe gradually towards the lateral side. At this point, deep to the sternomastoid lies the anterior scalene muscle and the medial scalene muscle lateral to it. The groove lies between these muscles usually in line with the lateral edge of the sternomastoid and BP nerve roots or trunks are visualised in this groove. Nerves in the groove appear hypo echoic and round. One description is that of ‘traffic lights’ where the three trunks are seen vertically on top of each other when the probe is placed at right angles to their direction of descent (Figure 2, 3). Depending upon the position of the probe, one may see the branching of the trunks. Deeper to the nerves, one may be able to visualise the hypoechoic transverse process of C6 and the vertebral artery. Cervical transverse process appear as ‘U’ shaped bright structure. The vertebral artery is only visualised below the C6 transverse process, a useful landmark in identifying specific nerve roots. For in plane approach, insert needle from the lateral end of the USGprobe (Figure 3).A dose of 10–15 ml is normally sufficient to induce complete brachial plexusblock although the risk of involvement of phrenic nerve is minimized if smaller volumes of 5 ml is used. It has been reported that 5 mL of 0.75% ropivacaine, or approximately 1.7 mL for each of the three trunks of the brachial plexus (superior, middle, and inferior) is sufficient to accomplish surgical anesthesia for shoulder surgery [21].The entire brachial plexus can be blocked from this position by slightly repositioning the needle to include the T1 root, which forms part of the ulnar nerve and is not blocked by nerve stimulation guidance. A catheter can also be inserted into the IS space if continuous brachial plexus anesthesia is desired.
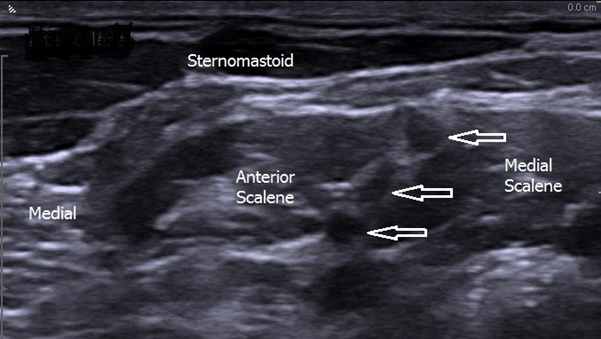
Figure 2: Sonoanatomy at interscalene level. Note the ‘traffic light’ position of the trunks (White arrows). Anterior scalene is medial to medial scalene muscle
One can also use the Trace back approach where the subclavian artery is first identified above the middle of the clavicle in SC fossa. Deeper to the artery, the hyperechoic pleura and 1st rib are identified. The trunks and divisions of the BP are visible as a bunch of grapes superior and lateral to the subclavian artery. The probe is gradually moved upwards towards the IS region whilst having a continuous view of the nerves.

Figure 3: Probe position for interscalene block. It is generally at the level of the cricoid cartilage. Needle is introduced from lateral side for in plane approach
SUPRACLAVICULAR BP BLOCK
SC block provides a rapid onset, dense and predictable anesthesia of the upper limb as the nerves are closely packed. It provides anesthesia and analgesia for arm and forearm surgery. The block is also useful for arterio-venous shunt surgery in patients requiring dialysis.
Sonoanatomy:
The BP and the subclavian artery lie on top of the first rib. The BP is located lateral and posterior to the subclavian artery. The subclavian vein and anterior scalene muscle are medial to the subclavian artery. The pleura is usually found 1-2cm deep from the BP. This explains the instances of pneumothorax before the era of USG. Pneumothorax can still occur with use of USG if structures are not properly identified. Note that both the pleura and first rib have a hyperechoic rim. However, the pleural moves with breathing efforts. Rib has the anechoic shadow beneath it as it blocks the USG waves.
Technique:
TheSC block is performed by an in-plane approach dueto risk of pleural puncture. Position the patient supine with the head slightly turned to the contralateral side. Titling the patient to the opposite side with pillows under the shoulder gives more room to access to plexus from a lateral to medial direction. The probe is placed firmly over the SC fossa in the coronal oblique plane with the probe pointing caudally (Figure 4).

Figure 4: Probe position for supraclavicular block. Note the change in orientation of probe when compared to interscalene approach
The probe is gently turned and angled to obtain the best possible transverse view of the subclavian artery. The BP in the SC region appear hypoechoic and is posterior to the pulsatile subclavian artery and superior to the first rib. If necessary, the nerve trunks from IS groove can be followed caudad, to the SC region to identify the divisions of the BP as a ‘bunch of grapes’ appearance above and lateral to the subclavian artery (Figure 5). Concurrent use of the nerve stimulator results in biceps and triceps twitches or hand muscle twitches.

Figure 5: Sonoanatomy at the supraclavicular level. Note the plexus looks like a ‘bunch of grapes’ located posterolateral to the subclavian artery
Observe local anesthetic spread around the plexus in real time during injection. Aim to deposit the local anesthetic initially immediately above the first rib and next to the subclavian artery to anesthetise the lower trunk. This usually lifts the BP away from the artery and allows circumferential spread of local anesthetic around the plexus. Colour Doppler use is encouraged to identify small vessels (SC or the transverse cervical artery) around the plexus which could be along the path of the needle and resemble hypoechoic nerve trunks/divisions.
INFRACLAVICULAR APPROACH
This approach targets the cords of the BP. At the IC level, the cords are arranged around the axillary artery and named accordingly. The axillary vein lies medial and caudad in relation to the artery. The pectoralis major and minor muscles lie anterior to the BPand one can see the contraction of these muscles if a nerve stimulator is used. The pleura lies 0.5 –1 cm deep to the axillary artery. Hence, it is important to determine the skin-pleura distance before needle insertion and not insert the needle deeper than this distance.
In 1146 cases of sonographically guided IC brachial plexus block, arterial puncture occurred in 8 (0.7%) patients. Therewere no reported cases of nerve injury, pneumothorax, or local anesthetic toxicity[22].IC approach is unsuitable in the presence of factors such as pacemaker. A recent Cochrane review [23] concluded that IC approach is as safe and effective as any other BP blocks, regardless of whether USG or nerve stimulator guidance is used. The advantages of ICB include a lower likelihood of tourniquet pain during surgery, more reliable blockade of the musculocutaneous nerve when compared to a single-injection axillary block, and a significantly shorter block performance time compared to multi-injection axillary and mid-humeral blocks.
Technique:
Position the patient supine with the arm to be blocked resting by the patient’s side. Using a small curved probe will provides a wider field of vision in comparison to a linear probe.Identify the coracoid process and move the probe medially in the parasagittal plane to obtain transverse view of the axillary artery and vein (Figure 6).
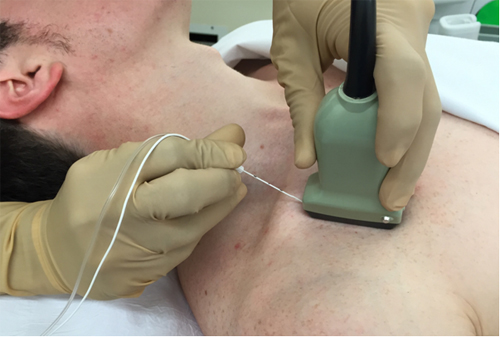
Figure 6: Probe position for infraclavicular block. The probe is nearly in the sagittal plane of the body. Note the approach of needle from the ‘top’
After identifying the coracoid process at infraclavicular area, identify the axillary vessels deep to the pectoralis muscles. Nerves in this region appear hyperechoic, with the lateral cord lying lateral and superficial to the axillary artery (9-12 o’clock position), the posterior cord lies posterior to the artery (6-9 o’clock position) and the medial cord lies medial and caudad (3-6 o’clock position) (Figure 7). The posterior cord can be confused with acoustic enhancement from the artery. Arm abduction will bring the three cords more superficial and will enhance the nerve visualization.
An in-plane approach is recommended to visualize the needle shaft and tip all the times during the procedure. Advance the needle from the cephalad end of the probe below the clavicle towards the caudad end in plane with the probe and USG beam. The goal is to deposit local anesthetic posterior to the artery resulting in a U shaped spread around the artery and all three cords.A higher volume of 20 – 25 ml is required for this block.
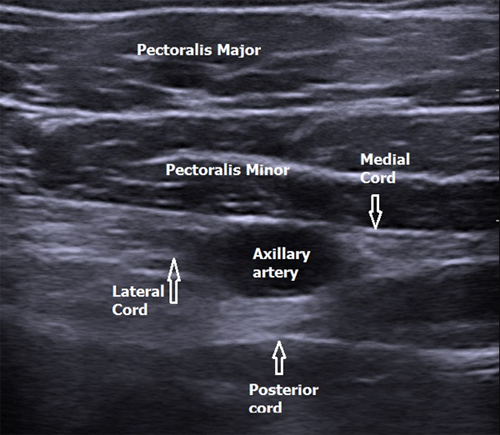
Figure 7: Sonoanatomy at the infraclavicular level. The cords are located at 2, 6 and 11 o’clock position
AXILLARY APPROACH
The axillary approach aims to block the terminal branches of the BP which include the median, ulnar, radial and musculocutaneous nerves. The median, ulnar and radial nerves lie next to the axillary artery surrounding it.The musculocutaneous nerve divides from the lateral cord in the proximal axilla and is commonly spared by the classical axillary approach. This will lead to ‘tourniquet pain’ if it is not blocked separately.
Sonoanatomy and technique:
An in plane approach is usually used. The needle is inserted at a shallow angle as the branches of the BP in the axilla are superficial. Position the patient supine and abduct the arm to 90 degrees and stand by the side of the patient. The probe is firmly placed along the axillary crease to obtain the best possible transverse view of the axillary artery (Figure 8).

Figure 8: Probe position for axillary block. The probe is parallel to the axillary crease. A lateral entry of needle aids access to musculocutaneous nerve
Nerves in the axilla have mixed echogenicity and a honey comb appearance. The nerves are round or oval, and are located around to the axillary artery often within 1 cm from the skin surface.Concurrent use of nerve stimulator may be required to precisely locate the different branches. The triceps, biceps and coracobrachialis muscles surround the artery and the hyperechoic and bright image of the humerus is visible deep to the muscles. The hyperechoic musculocutaneous nerve lies in the plane between the biceps and coracobrachialis muscles. The location of the nerves around the axillary artery is quite variable. Also, the vascular relationships are affected by changes in arm position and applied external pressure during regional block performance.The median nerve often has a honey combed appearance and lies between the 9 -12 o’clock position. The ulnar nerve usually lies between the axillary artery and axillary vein, often underneath the vein at the 1-3 o’clock position [Figure 9). The radial nerve lies deep to the ulnar nerve, often in the 5-6 o’clock position and is often more difficult to locate. Alternatively the nerves could be traced upwards from the lower arm or elbow region to ensure the correct nerves are identified around the axially artery.15 to 25 ml of local anesthetic is required for the axillary block.
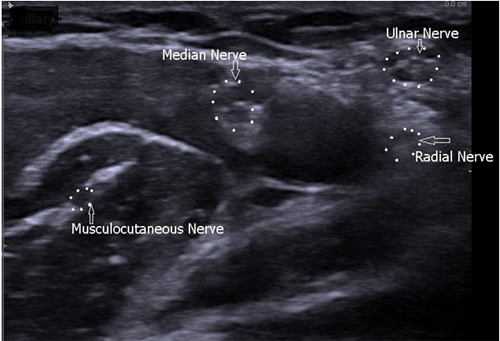
Figure 9: Sonoanatomy at axillary level. The relation to axillary artery is maintained. Note musculocutaneous has moved much laterally. The honey-comb appearance of nerves is seen. Nerves outlined with white dots
USES OF BP BLOCKS
Apart from anesthesia and postoperative analgesia, USG guided BP block has been used in the management of upper limb ischaemia in a neonate [24].The somatic nerves also carry the sympathetic fibres to the vessels in the distal upper limb, which leads to vasodilatation. Blaivas and Lyon used USG guided BP block to aid reduction of dislocated shoulders in Emergency department [25].
PEDIATRICS
In children, the nerves and blood vessels are usually more closely related leading to increased risk of complications. The use of USG guided blocks in children was first described in 2004 [26]. USG guidance has been demonstrated to improve block characteristics in children including shorter block performance time, higher success rates, shorter onset time, longer block duration, less volume of local anesthetic agents and visibility of neuraxial structures [27]. USG guided BP block has been successfully used in children as young as 6 months. Lower volumes of local anesthetic is highly desirable due to weight restrictions.USG guided SC blocks have been shown to slightly quicker to perform and have a higher success rate when compared to the IC route [28]. The complication rate with either route was low. Brachial plexus catheters have been shown to be safe in children [29]. The incidence of complications was similar to adults with catheter dislodgement or occlusion accounting for 60%. There were no reports of persistent neurologic problems, serious infection or local anesthetic toxicity. Infection is unlikely if the catheter stays in for 3 days or less.
SUMMARY
In summary, USG guided BP blocks is becoming the standard of practice in both adults and children. It has been shown to be more effective, have less incidence of complications and is quicker to perform. There are different approaches to BP block available depending upon the need with each having its advantages and disadvantages. The user needs to be aware of pitfalls of using USG guidance as certain structures look very similar.
Authors’ contribution:
SK: Did the literature search, labelled the images and revised the manuscript
SM: Provided the draft version of manuscript and images
SS: Provided the draft version of manuscript and images
REFERENCES
- McCartney JL, Lin L, Shastri U. Evidence basis for the use of ultrasound for upper-extremity blocks. RegAnesth Pain Med 2010;35(2 Suppl):S10–15[PubMed]doi: 10.1097/AAP.0b013e3181d25675.
- Nielsen KC, Steele SM. Outcome after regional anaesthesia in the ambulatory setting—is it really worth it? Best Pract Res ClinAnaesthesiol 2002;16(2):145 –57[PubMed]
- Orebaugh SL, Kentor ML,Williams BA. Adverse outcomes associated with nerve stimulator-guided and ultrasound-guided peripheral nerve blocks by supervised trainees: update of a single-site database. RegAnesth Pain Med. 2012;37(6):577–82.[PubMed] [Free full text]doi: 10.1097/AAP.0b013e318263d396.
- Kessler J, Marhofer P, Hopkins PM, Hollmann MW. Peripheral regional anaesthesia and outcome: lessons learned from the last 10 years. Br J Anaes 2015;114(5):728–45 [PubMed] doi: 10.1093/bja/aeu559.
- Munirama S, McLeod G. A systematic review and meta-analysis of ultrasound versus electrical stimulation for peripheral nerve location and blockade. Anaesthesia2015;70(9):1084–91[PubMed] [Free full text]doi: 10.1111/anae.13098.
- Kulenkampff D, Persky MA. Brachial plexus anaesthesia: its indications, technique, and dangers. Ann Surg1928 Jun;87(6):883-91.[PubMed] [Free full text]
- La Grange P, Foster P, Pretorius L. Application of the Doppler ultrasound blood flow detector in supraclavicular brachial plexus block. Br J Anaesth. 1978 Sep;50(9):965-7.[PubMed]
- Kapral S, Krafft P, Eibenberger K, Fitzgerald R, Gosch M, Weinstabl C: Ultrasound-guided supraclavicular approach for regional anesthesia of the brachial plexus. AnesthAnalg 1994 Mar;78(3):507-13. [PubMed]
- Mukherji SK, Wagle A,Armao DM, Dogra S. Brachial plexus nerve block with CT guidance for regional pain management: Initial Results. Radiology 2000 Sep;216(3):886–90. [PubMed] [Free full text]
- Chan VWS, Perlas A, Rawson R, Odukoya O. Ultrasound-guided supraclavicular brachial plexus block. AnesthAnalg 2003 Nov;97(5):1514 –17.[PubMed]
- Neal JM, Hebl JR,Gerancher JC,Hogan QH. Brachial plexus anesthesia: essentials of our current understanding. RegAnes Pain Med 2002 Jul;27(4):402–28. [PubMed]
- Benhamou D. Axillary plexus block using multiple nerve stimulation: A European view (editorial). RegAnesth Pain Med 2001 Nov;26(6):495-98. [PubMed]
- Lanz E, Theiss D, Jankovic D. The extent of blockade following various techniques of brachial plexus block. AnesthAnalg 1983 Jan;62(1):55-8. [PubMed]
- Satyanarayana N, Vishwakarma N, Kumar GP, Guha R, Datta AK, Sunitha P. Variation in relation of cords of brachial plexus and their branches with axillary and brachial arteries—a case report. Nepal Med Coll J 2009 Mar;11(1):69–72.[PubMed]
- Hadzic A. Ultrasound-guided IS brachial plexus block. In: Hadzic A, Carrera A, Clark T, et al. Hadzic’s peripheral nerve blocks and anatomy for ultrasound-guided regional anesthesia, 2nd ed. New York: The McGraw-Hill Companies, Inc. 2012:353.
- Association of Anaesthetists of Great Britain and Ireland, Obstetric Anaesthetists’ Association and Regional Anaesthesia UK. Regional anaesthesia and patients with abnormalities of coagulation. Anaesthesia 2013 Sep;68(9):966-72.[PubMed] [Free full text]doi: 10.1111/anae.12359.
- Knoblanche GE. The incidence and aetiology of phrenic nerve blockade associated with supraclavicular brachial plexus block. Anaesth Intensive Care. 1979 Nov;7(4):346–9.[PubMed]
- Mak PH, Irwin MG, Ooi CG, Chow BF. Incidence of diaphragmatic paralysis following supraclavicular brachial plexus block and its effect on pulmonary function. Anaesthesia. 2001 Apr;56(4):352–6.[PubMed] [Free full text]
- Renes SH, Spoormans HH, Gielen MJ, Rettig HC, van Geffen GJ. Hemidiaphragmatic paresis can be avoided in USG-guided supraclavicular brachial plexus block. RegAnesth Pain Med. 2009 Nov;34(6):595–9.[PubMed]
- Holborow J, Hocking G. Regional anaesthesia for bilateral upper limb surgery: a review of challenges and solutions. Anaesth Intensive Care. 2010 Mar;38(2):250–8.[PubMed] [Free full text]
- Gautier P, Vandepitte C, Ramquet C. The minimum effective anesthetic volume of 0.75% ropivacaine in USG-guided interscalene brachial plexus block. AnesthAnalg 2011 Oct;113(4):951–5. [PubMed] doi: 10.1213/ANE.0b013e31822b876f.
- Sandhu NS, Manne JS, Medabalmi PK, Capan LM. Sonographically guided infraclavicular brachial plexus block in adults: a retrospective analysis of 1146 cases. J USG Med 2006 Dec;25(12):1555–61. [PubMed] [Free full text]
- Chin KJ, Alakkad H, Adhikary SD, Singh M. Infraclavicular brachial plexus block for regional anaesthesia of the lower arm. Cochrane Database Syst Rev.2013 Aug;28:8[PubMed] [Free full text]doi: 10.1002/14651858.CD005487.pub3.
- Ponde VC,Shah DM, Mane S. Role of ultrasound-guided continuous brachial plexus block in the management of neonatal ischemia in upper limb. Saudi J Anaesth. 2012 Oct;6(4):423–5. [PubMed] [Free full text]doi: 10.4103/1658-354X.105898.
- Blaivas M, Lyon M. Ultrasound-guided interscalene block for shoulder dislocation reduction in the ED. Am J Emerg Med 2006 May;24(3):293-6.[PubMed]
- Marhofer P, Sitzwohl C, Greher M, Kapral S.Ultrasound guidance for infraclavicular brachial plexus anaesthesia in children. Anaesthesia 2004 Jul;59(7):642–6. [PubMed] [Free full text]
- Rubin K, Sullivan D, Sadhasivam S. Are peripheral and neuraxial blocks with ultrasound guidance more effective and safe in children? PaediatrAnaesth 2009 Feb;19(2):92–6. [PubMed] doi: 10.1111/j.1460-9592.2008.02918.x.
- De José María B, Banús E, Navarro Egea M, Serrano S, Perelló M, Mabrok M. Ultrasound-guided supraclavicular vs infraclavicular brachial plexus blocks in children.PaediatrAnaesth. 2008 Sep;18(9):838-44. [PubMed] doi: 10.1111/j.1460-9592.2008.02644.x.
- Walker BJ, Long JB, De Oliveira GS, Szmuk P, Setiawan C, Polaner DM, et al. Peripheral nerve catheters in children: an analysis of safety and practice patterns from the pediatric regional anesthesia network (PRAN). Br. J. Anaesth. 2015 Sep;115(3):457-62. [PubMed] doi: 10.1093/bja/aev220.



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube