
Ewa Werpachowska, MBChB*,Santhana Kannan, MD, DNB, FRCA**, Vincent Bulso, FRCA**
*Core Trainee; **Consultant
Department of Anaesthesia, City Hospital, Dudley Road, Birmingham (United Kingdom)
Correspondence: Dr S. Kannan, Department of Anaesthesia, City Hospital, Dudley Road, Birmingham B18 7QE. (United Kingdom); Phone: 0044 121 5074343; Fax: 0044 121 5074349; E-mail: kannan.gas@gmail.com
Key words: Cannulation; Intravenous
Citation: Werpachowska E, Kannan S, Bulso V. Uncommon case of an obstructed intravenous cannula. Anaesth Pain & Intensive Care 2014(18(4):471-472
New ‘safety’ cannulae have been introduced in practice which provide passive automatic protection against needle stick injury. They have a built-in mechanism which is activated upon removal of the needle from the cannula and covers the sharp needle tip. There have been no reports of structural defects in such cannulae causing problems. We report an instance where in spite of a successful intravenous placement with a safety cannula, it was unusable and had to be replaced.
An ASA I woman presented for an elective day case procedure. The patient had prominent and so easy peripheral veins. A 20G venous cannula (Vasofix® Safety, B. Braun Melsungen AG, Germany) was inserted on first attempt. There was a flashback of blood into the hub. The cannulation was done as normal and the needle removed. It was then noticed that the cannula could not be flushed. There was no swelling at the site and the patient did not report any pain. The cannula could not be aspirated either. However, drops of blood did flow back on opening the end-cap. Repeat attempts at flushing the cannula failed. Another 20G cannula (same batch) was inserted into a different arm successfully on first attempt and the anesthesia proceeded uneventfully.
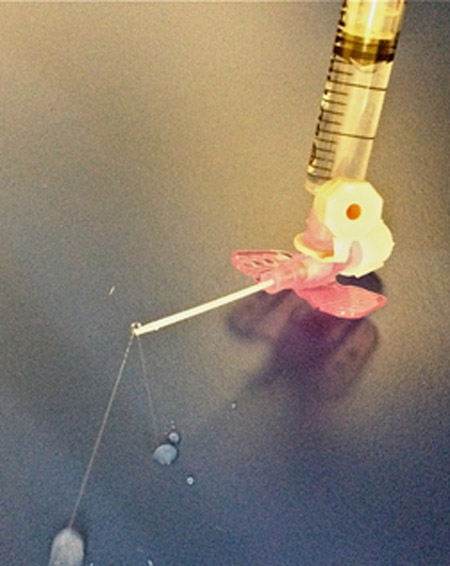
The first cannula was removed and inspected. There was no obvious physical damage, kink or change in its structure. When the cannula was flushed, the cause for the ‘partial obstruction’ became apparent. The tip of the cannula was blocked except for two narrow jets of the fluid being let out from the sides at different angles during the flush (Figure 1) with significant amount of pressure during injection. Since the cannula was not completely obstructed, it allowed the flashback of blood into the hub. One would expect that the presence of needle within the cannula would ensure cannula patency. This report shows that it need not be the case.
Figure 1: Tip of the cannula showing two thin jets of fluid
Structural defects in intravenous cannulae are very rare.[1,2]. The type of defect reported here can become significant in an emergency or in a patient with poor veins. Also, visible flashback of blood can lead to repeatedly failed attempts to flush the cannula as partial obstruction is less likely to be suspected. The old adage ‘if in doubt, take it out’ should be exercised.
REFERENCES
- Sinden MP, Jayamaha JE. Defective intravenous cannulae. Anaesthesia1995;50:829-830.
- Bannister M, Stacey, MRW. Faulty intravenous cannulae. Anaesthesia 2000;55:937.



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube