
Shiv Kumar Singh1, Hetal B. Vadera2
1Consultant Anaesthesia, Department of Anaesthesia, Royal Liverpool University Hospitals, Liverpool,(UK)
2Consultant & Head, Department of Anaesthesia, Sterling Hospital, Rajkot, (India)
Correspondence:Dr Shiv Kumar Singh, Department of Anaesthesia, 11th Floor, Royal Liverpool University Hospitals, Prescot Street, Liverpool L7 8XP (UK);
E-mail: shiv.singh@rlbuht.nhs.uk
ABSTRACT
Inguinal hernia surgery is one of the commonest day case procedure in any surgical unit, and one of the procedures that has a very high incidence of persistent post-surgical pain. Blocks of the ilioinguinal and iliohypogastricnerves may reduce the incidence of this chronic pain. Blocking the genital branch of genitofemoral nerve completes the nerve block for inguinal hernia surgeries. All these three nerves can be easily blocked under ultrasound guidance and this improves the effectiveness of the block. Failures in achieving complete anesthesia and analgesia is not always due to technical reasons, anatomical variations may be the cause in some of the cases. This article describes the anatomy, sonoanatomy, the variations and the nerve blocks under ultrasound guidance.
Key words:Hernia, Inguinal/surgery; Nerve Variations; Nerve Block; Nerve Blockade; Anesthesia, Local; Spinal Nerves; Acute Pain; Pudendal Neuralgia; Ultrasound; Ultrasonography; Ultrasound Imaging; Ultrasonography, Interventional
Citation:Singh SK, Vadera HB. Ultrasound guided hernia blocks. Anaesth Pain &Intensive Care 2015;19(3):366-371
INTRODUCTION
Inguinal hernia repair is one of the commonest day-case surgical procedures. Significant part of the pain from hernia surgery arises from the abdominal wall incision, the somatic pain. Despite the effective perioperative pain management strategies, the frequency of moderate to severe pain from this lower abdominal surgeryis seen in approximately 30–75% of the patients.1-3
In normal circumstances, the acute pain associated with inguinal hernia surgery diminishes within several days to weeks but, in about 10% of cases, this pain persists and patient experience what is know as chronic or persistent post surgical pain (CPSP or PPSP).4-6 The most consistent risk factor for CPSP is the presence and/or intensity of pain experienced in the perioperative period and hence preventive analgesia and optimal treatment of post-operative pain is essential to prevent, mitigate, or treat CPSP in hernia surgeries.4-6
Peripheral nerve blocks along with multimodal analgesia are commonly employed for perioperative management of pain arising from hernia surgeries. These blocks are often performed using blind techniques and, more recently under ultra-sound guidance. The failure rates of blind technique as per the published literature are approximately 30- 60%.7-8 This high rate of failure comes from the lack of knowledge about the anatomy of the nerves (anomalies and anatomical variations) and partly from the failure to eliminate the “cushion effect” while performing the loss of resistance (LOR) blocks.9
Complete analgesia for any inguinal hernia surgery not only requires blockade of the ilioinguinal nerve(IIN) and iliohypogastric (IHN) nerve but also blockade of the genital branch of the genitofemoral nerve (GFN).
Blocks of the IIN and IHN can be performed with anatomical landmarks (conventional, blind technique) or with ultrasound guidance(USG) techniques. In recent years, the ultrasound-guided nerve blocks are gaining popularity and have been found to have greater success.Blockade of the genital branch of the GFN can either be done by the surgeon under direct vision or under ultrasound guidance.
In this article, we discuss the blockade of the IIN, IHN and GFN under ultrasound guidance.
APPLIEDANATOMY
IIN and IHN
Both the IIN and IHN arise from first lumbar ventral ramus(Figure 1)The IINis smaller than IHN and arises with it to emerge from lateral border of psoas major, with or just inferior to the IHN. It passes obliquely across quadratus lumborum and the upper part of iliacus and enters transversus abdominis near the anterior end of the iliac crest. It sometimes connects with the IHN at this point. It pierces internal oblique and supplies it and then traverses the inguinal canal below the spermatic cord. It emerges with the cord from the superficial inguinal ring to supply the proximal medial skin of the thigh and the skin over the root of the penis and upper part of the scrotum in males, or the skin covering the mons pubis and the adjoining labium majus in females. The IHN follows similar route to IIN but terminates earlier in the anterior abdominal wall above the pubic tubercle.The IIN and IHN are reciprocal in size.10-11
There are number of anatomical variations described in relation to their origin and the course of these two nerve. There are cadaveric studies that report total absence of the IIN.12-15 There is also variable emergence of the nerve in relation to the internal oblique muscle.12 These variations may be responsible for nerve block failures when done blindly using landmark techniques.
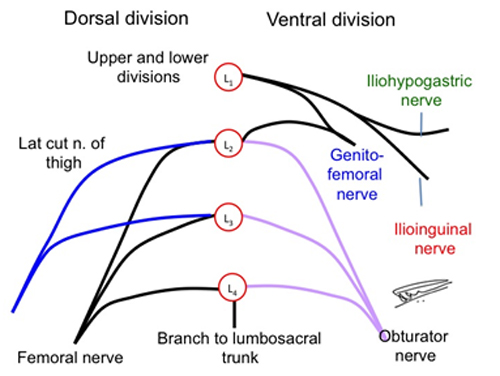
Figure 1: Origin of ilioinguinal, iliohypogastric and the genitofemoral nerves from the lumbar plexus
There are variations in the origin of the II and IHN nerves. In one of the studies it was found that the IIN originated mostly fromL1 (65%) but in 14% it originated from T12 and L1 and in small percentage from L1 and L2 (11%) or even from L2 and L3 (10%). The IHN originated from T12 in 7%, from T12 and L1 in 14%, from L1 in 10%, and from T11 and T12 in 6%.11
The entry and termination of the two nerves in the anterior abdominal wall is pretty constant.The IIN enters the abdominal wall approximately 3.0 cm medial and 4.0- 5.0 cm inferior to the anterior superior iliac spine (ASIS)and terminates approximately 3 cm lateral to the midline. The IHN enters the abdominal wall at similar distance from ASIS as II nerve but slightly inferior, at around 1.5 cm to the ASIS and terminates around 4.0 – 5.0 cm lateral to the midline.12
IIN is sometimes smaller and terminates near the iliac crest by joining the IHN, which then sends branches to replace the absent terminal part of the IIN.10, 12
The IINis normally devoid of the lateral cutaneous branch but in some it provide a lateral cutaneous or iliac branch to supply the skin in the region of the anterior superior iliac spine. It may even partially or completely replace the genital branch of the genitofemoral nerve or the lateral femoral cutaneous nerve.
The IIN and IHN sometime arise as a common trunk, and in their course, usually separate between the transversus abdominis and internal oblique muscles.
Eichenberger et al in their anatomical study for hernia block found that both IIN and IHN lie in the transversus abdominis plane at a point 5cm cephalad and 5 cm posterior to the ASIS. This is an ideal point for both USG and landmark based IIN and IHN blocks.16
Genital Branch of GFN
Like the IIN and IHN, GFN also takes origin from the lumbar plexus (L1 and L2 roots). (Figure 1)It predominantly carries sensory fibers, except for the motor fibres to cremasteric muscle. The nerve after its formation in the lumbar plexus lies on the psoas muscle, crosses the ureter on its descent before it dividing into femoral and genital components at variable distance from the inguinal ligament. The femoral branch passes under the inguinal ligament into the femoral sheath to supply the skin over the femoral vessels. The genital branch on the other hand passes through the internal inguinal canal/ring and descends behind the spermatic cord in males or the round ligament in females. In males it provides sensory supply to skin over the scrotum and motor fibres to the cremasteric muscles. In females the nerve supplies the skin over the mons pubis and labium majus.17
As described above, there are anatomical variations in the origin and distribution of the nerve. There are free communications between the three nerves and hence it is important to block all three for complete analgesia for the surgeries involving this region of the body.18
PATIENT POSTION AND LANDMARKS
The patient is positioned supine for this block. The important landmarks for the blocks are the iliac crest and the anterior superior iliac spine (ASIS). The point of interest is 5 cm cranial and 5 cm posterior to the ASIS for the IIN and IHN blocks. (Figure 2)As explained earlier, at this point the IIN has penetrated the transversus abdominis muscle with 90% probability and the IH with 95% probability. Both these nerves are found in the transversus abdominis plane (TAP) with 90% probability. The landmark for the GFN block is a point media to the pubic tubercle (PT).16
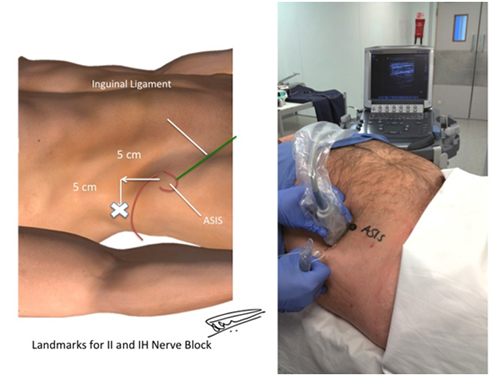
Figure 2: Landmarks and probe position for IIN and IHN block [ASIS = Anterior superior iliac spine]
PROBE POSITION
IIN and IHN Block
The US probe (transducer) is positioned transversely above the ASIS and is moved cranially and then posteriorly into an oblique position just above the iliac crest.(Figure 2) The probe in this position lies perpendicular to the anatomical course of the two nerves. The probe can be adjusted so that the cross-sectional images of the two nerves can be easily obtained (Figure 3).
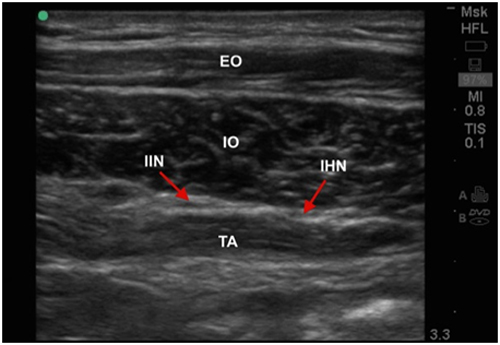
Figure 3: Sonoanatomy of the IIN and IHN. Both nerves lie in transversus abdominis plane at the landmark described [EO = External oblique muscle; IO = Internal oblique muscle; TA =Transversus abdominis muscle]
Genital Branch of GFN
For this nerve block, the probe is placed transversely just lateral to the pubic tubercle, parallel and above the inguinal ligament(Figure 4).At this point the spermatic cord can be easily identified. The probe can also be placed over the femoral vessels and then moved cranially and medially, above the inguinal ligament towards the pubic tubercle till the spermatic cord is easily identified 19(Figure 5).
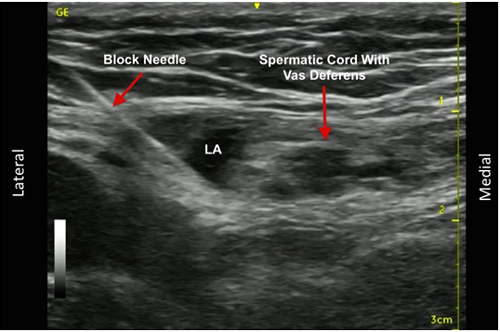
Figure 5: Sonoanatomy of the spermatic cord for the genital branch of genitofemoral nerve block
SONOANATOMY
IIN and IHN
At the probe position described above, in almost 90% of the subjects both the IIN and the IH nerves can be seen lying next to each other in the transverses abdominis plane. In the US image, we see three distinct muscles under the subcutaneous tissues, from outside-in (top to bottom) we see; external oblique (EO), Internal Oblique (IO) and the Transversus abdominis (TA) muscles. The fascia separating these muscles is hyper-echoic and the fascial plane we are interested in lies between the IO and TA muscle. The fascia here splits to enclose the IIN and IH nerves. (Figure 3) It is at this point that the local anaesthetic is deposited to block both the IIN and IH nerves.
Genital Branch of GFN
With the US probe placed medial to the PT and above and parallel to the inguinal ligament. (Figure 4) We identify the contents of the internal inguinal canal; spermatic cord and in some cases the testicular vessels. (Figure 5)On moving the probe caudally the femoral vessels can also be identified. It is important to keep the probe above the inguinal ligament and avoid injection of local anesthetic (LA) below the inguinal ligament at any time.
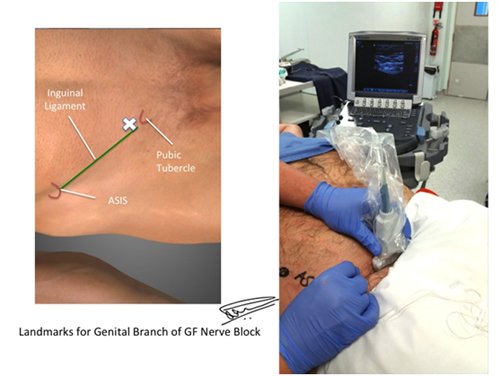
Figure 4: Landmarks and probe position for genital branch of genitofemoral nerve (GFN) block
EQUIPMENT REQUIRED
Ultrasound machine with high frequency linear probe (HFL), standard block tray (including Intralipid® 20%), 22G (50mm, 80mm and 100mm) needlesand 20 ml syringes with local anesthetic (levo-bupivacaine, bupivacaine or ropivacaine)
TECHNIQUE
IIN and IHN Blocks
With the patient positioned supine, a point is marked 5 cm cranial and 5 cm posterior to the ASIS. After following standard aseptic precautions and appropriate preparation of the US probe, the HFL probe is placed above the ASIS and then moved cranially and then posteriorly so that the probe lies at an oblique transverse position just above the iliac crest. The probe is adjusted so that cross-sectional view of the IIN and IHN is obtained. The nerves are positioned at the centre of the US screen, the depth and gain adjusted appropriately. The three layers of muscles are identified; similar to the way TAP blocks are done. The IIN and IH are identified as two hypoechoic shadows lying within the split of the IO fascia. (Figures 2 & 3)
The nerve block can be done either awake or under GA. In awake patients, the skin is infiltrated with short acting LA (1% lignocaine), just lateral to the transducer where the needle entry point is located. A 80mm or 100mm short beveled needle is advanced in-plane from lateral to medial direction, keeping tip of the needle under vision at all times. The needle passes through the skin and subcutaneous tissues and then the EO and IO muscles. The needle is then advanced to pierce the IO fascia just lateral to the nerves. The LA needs to be deposited under the IO fascia so as to surround the two nerves. In short stature and obese patients, placing a sand bag under the ipsilateral side provides a tilt and helps to approach the nerves from the lateral side. In case of difficulties, the nerves can be approached from medial to lateral side as well with equal efficacy.
After confirming position of the tip of the needle is in right plane, 10-15 ml of LA is injected in 5ml aliquots after aspiration. Attempt is made to identify both nerves but in certain cases due to the anatomical variations, they may not be visible, in such cases using slightly larger volumes (20-30 ml) may ensure block success. In all cases the volume of LA should not exceed the prescribed toxic limits i.e. no more than 2mg/ kg for (levo-) bupivacaine and 3mg/kg of ropivacaine.
Genital Branch of GFN Block
Anaesthetists rarely do this block, as it is easier for the surgeon to deposit LA under direct vision. For this block, the probe is positioned as described above. Once the spermatic cord is identified, a 50-80 mm block needle is introduced from the lateral side using in-line approach. It is important to always aspirate before we inject, as there are small vessels located in this region. Once the needle tip is next to the spermatic cord, 5ml of LA is deposited after aspiration. The LA can be seen surround the spermatic cord(Figures 4 & 5).
COMPARISON WITH LANDMARK TECHNIQUE
As compared to landmark technique, success rate of the block is higher in expert hands using US guided nerve blocks. Failure rates are higher in landmark techniques,mostly due to deposition of LA in the wrong plane, wrong landmarks and possibly due to anatomical variations as described in the article.7-8 Similarly, complication rates are considered to be lower with ultrasound guided technique.7-8
CLINICAL PEARLS
- IIN and IHN blocks do not cover visceral pain and it is important to use multi-modal analgesia for better outcomes and patient satisfaction. Using simple analgesics like IV paracetamol and diclofenac helps in better control of postoperative pain.
- Patient may feel pain during handling of the hernia sac if genital branch of GFN is not blocked and in such cases surgeons can be instructed to deposit 5-7 ml of LA around the spermatic cord or in the sac itself.
- In-plane technique is always preferable but out-of-plane technique can also be used in obese or patients with difficult anatomy.You may also need to use curvilinear probe in morbidly obese patients to identify the structures that are much deeper.
- These blocks are volume dependent and one must not shy away from using larger volumes, keeping in mind the toxic limits and the possibility of the surgeon needing to infiltrate in case of failure or sparing.
CONCLUSION
IIN and IHN blocks are very effective techniques in providing anaesthesia and postoperative analgesia for inguinal hernia surgeries. Adding genital branch of GFN block completes the hernia blocks and provides complete anaesthesia and analgesia for the region. Ultrasound guidance adds accuracy to the performance of the blocks and reduces the complications and failure rates. It is important to recognise that many variations exist in the origin and course of the nerves. The IIN, IHN and the GFN often communicate with each other and hence blockade of all the three are important in providing complete analgesia.
Conflict of interest: None declared by the author.
Financial disclosure: Nil
REFERENCES
- Callesen T,Bech K, Nielsen R. Pain after groin hernia repair. Br J Surg. 1998;85(10):1412– [PubMed]
- Toivonen J, Permi J, Rosenberg PH. Analgesia and discharge following preincisional ilioinguinal and iliohypogastric nerve block combined with general or spinal anaesthesia for inguinal herniorrhaphy. ActaAnaesthesiol Scand.2004;48:480-485. [PubMed]
- Poobalan AS, Bruce J, Smith WC, King PM, Krukowski ZH, Chambers WA. A review of chronic pain after inguinal herniorrhaphy. Clin J Pain. 2003;19:48–54 [PubMed]
- Mallikarjuna M, Santhosh S, and Abhishek V. Chronic Pain after Inguinal Hernia Repair. International Scholarly Research Notices.2014, vol. 2014, Article ID 839681, 6 pages. [Free full text]DOI:10.1155/2014/839681
- Nienhuijs SW, Staal JF, Strobbe LJA, Rosman C, Groenewoud JMM, Bleichrodt RP. Chronic pain after mesh repair of inguinal hernia: a systemic review.Am J Surg, 2007;194:394–400 [PubMed][Free full text]
- Kehlet H, Jensen TS, Woolf CJ. Persistent postsurgical pain: risk factors and prevention. Lancet.2006 May 13;367(9522):1618-25[PubMed]
- Lim SL, Ng Sb A, Tan GM. Ilioinguinal and iliohypogastric nerve block revisited: single shot versus double shot technique for hernia repair in children. PaediatrAnaesth. 2002;12:255–260. [PubMed]
- Weintraud M, Marhofer P. Bösenberg A,Kapral S, Willschke H, Felfernig M, Kettner S.Ilioinguinal/iliohypogastric blocks in children: where do we administer the local anesthetic without direct visualization? AnesthAnalg. 2008;106(1):89–93[PubMed]doi: 10.1213/01.ane.0000287679.48530.5f.
- Singh SK, Gulyam Kuruba SM: The Loss of Resistance Nerve Blocks.International Scholarly Research Network; ISRN Anesthesiology. Volume 2011, Article ID 421505[Free full text]doi:10.5402/2011/421505.
- Klaassen Z,Marshall E, Shane Tubbs R,Louis RG Jr, Wartmann CT, Loukas M. Anatomy of the ilioinguinal and iliohypogastric nerves with observations of their spinal nerve contributions. Clin Anat. 2011 May;24(4):454-61[PubMed]doi: 10.1002/ca.21098.
- Papadopoulos NJ,Katritsis ED. Some observations on the course and relations of the iliohypogastrics and IINs (based on 348 specimens). Anat. Anz.1981;149(4):357-64. [PubMed]
- Jamieson RW, Swigart LL, Anson BJ. Points of parietal perforation of the ilioinguinal and iliohypogastric nerves in relation to optimal sites for local anesthesia. Q Bull Northwest Univ Med Sch1952;26(1):22-6. [PubMed][Free full text]
- Oelrich TM andMoosman DA. The aberrant course of the cutaneous component of the ilioinguinal nerve. Anat. Rec. 1977;189:233-6.[PubMed][Free full text]
- Yıldız S ,KocabıyıkN, CoşkunK, ÖzerT, Zeybek N. Association of anatomical variations of ilioinguinal nerve with inguinal hernia repair. Gulhane Med J. 2012;54(2):155-9.
- Rab M, Ebmer J, Dellon AL. Anatomic variability of the ilioinguinal and genitofemoral nerve: Implications for the treatment of groin pain. PlastReconstr Surg. 2001;108:1618–23 [PubMed]
- Eichenberger U, Greher M, Kirchmair U, Curatolo M, Moriggl B. Ultrasound-guided blocks of the ilioinguinal and iliohypogastric nerve: accuracy of a selective new technique confirmed by anatomical dissection. Br J Anesth. 2006;97:238–43[PubMed][Free full text]
- Liu WC, Chen TH, Shyu JF, Chen CH, Shih C, Wang JJ, et al. Applied anatomy of the genital branch of the genitofemoral nerve in open inguinal herniorrhaphy. Eur J Surg. 2002;168(3):145–149 [PubMed]
- Sasaoka N, Kawaguchi M, Yoshitani K,Kato H,Suzuki A, Furuya H. Evaluation of genitofemoral nerve block, in addition to ilioinguinal and iliohypogastric nerve block, during inguinal hernia repair in children. BrJ Anaesth. 2005;94(2):243-6. [PubMed][Free full text]
- Wipfli M, Birkhauser F, Luyet C, Greif R, Thalmann G, Eichenberger U. Ultrasound-guided spermatic cord block for scrotal surgery. Br J Anaesth. 2011;106:255–259. [PubMed][Free full text]doi: 10.1093/bja/aeq301.



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube