
Sonal S. Khatavkar, MBBS, DNB , DA1, Sarika S. Lonkar, MBBS, DNB2, Pournima B. Panchal, MBBS, DNB3, W. S. Thatte, MBBS, MD, DA4, Sai Nagendra, MBBS3, Divya Tewari, MBBS3
1Associate Professor; 2Assistant Professor; 3Senior Resident; 4Professor & HOD
Department of Anesthesiology, Dr. D Y Patil Medical College, Pimpri, Pune, Maharashtra – 411018, (India)
Correspondence: Dr Sonal S. Khatavkar, Flat S2/B1, Tejovalaya, Raviraj Co-op. Housing Society Ltd, Warje, Pune – 411058 (India); Phone: 9820434472; E-mail: drsonalkhatavkar@yahoo.co.in
ABSTRACT
Objective: Caudal block has gained much popularity in the past few decades to provide analgesia in pediatric population. Although local anesthetic agents remain the mainstay for caudal blocks, addition of additives to the solution improves quality and duration of analgesia and reduces the toxicity by allowing lower concentrations of the local anesthetic agents. In this regard opioids have been studied extensively, but there is not much comparative research about caudal clonidine. The aim of our current study was to compare the caudal block characteristics of ropivacaine 0.25% with clonidine 1 µg/kg versus ropivacaine 0.25% with fentanyl 1µg/kg in pediatric patients.
Methodology: A total of 60 ASA 1 children of either gender, age from 2 to 10 years, weighing 10 to 30 kg, scheduled for lower abdominal or limb surgery, were enrolled for this study. Children were randomly allocated into 2 equal groups. Group RF received 1 ml/kg of ropivacaine 0.25% plus fentanyl 1μg/kg via caudal route. Group RC received 1 ml/kg of ropivacaine 0.25% plus clonidine 1 µg/kg via same route. All children were administered general anesthesia followed by caudal block for postoperative analgesia. Duration of analgesia, sedation score and any side effects were noted. Calculation of sample size was done by using power analysis. The non-parametric data comparison was done by Student’s t-test.
Results: Duration of analgesia was significantly prolonged in RC group. Dose requirement for rescue analgesia was significantly lesser in group RC. There was no significant difference between both groups for hemodynamic response after caudal block. The incidence of side effects were not significant.
Conclusion: In conclusion clonidine and fentanyl, both improve the quality of analgesia when used with ropivacaine in caudal block in pediatric patients, but the quality of analgesia and duration with clonidine plus ropivacaine is superior to fentanyl plus ropivacaine.
Key words: Ropivacaine; Clonidine; Fentanyl; Caudal block; Analgesia
Citation: Khatavkar SS, Lonkar SS, Panchal PB, Thatte WS, Nagendra S, Tewari D. The efficacy of ropivacaine-fentanyl versus ropivacaine-clonidine for pre-emptive caudal anesthesia in children. Anaesth Pain & Intensive Care 2016;20(1):54-58.
INTRODUCTION
Pain is a protective mechanism designed to alert the body to potentially injurious stimuli. Pain has been defined as an unpleasant sensory and emotional experience, associated with actual or potential tissue damage.1 “It is our responsibility to treat pain in neonates and infants as effectively as we do in other patients” – Rogers M.2
Postoperative pain relief in children is very important since emotional component of pain is very strong in children. As pain is very difficult to be assessed in pediatric population, postoperative pain is very commonly under treated in this age group.
Caudal epidural is now one of the most commonly performed regional blocks in pediatric anesthesia, after its first description by Campbell in 1933.3 It is well-accepted and proven technique for providing analgesia. Use of single local anesthetic agent via caudal route may provide a shorter duration of block4 and thus often requires supplemental agents. Bupivacaine and ropivacaine are the most commonly used local anesthetic drugs for caudal block.
Ropivacaine has been used for regional anesthesia in adults5 and can be used even in younger patients for caudal epidural analgesia.6,7 It offers some advantage over bupivacaine as it has less cardiac and neurological toxicity, less motor blockade and prolonged sensory analgesia.8
Addition of adjuvants (opioids, ketamine etc.) prolongs the duration of block and is used increasingly in current practice. Opioids have a risk of postoperative respiratory depression, and ketamine has the potential of neurotoxicity if inadvertently injected intrathecally.9 Clonidine, is an alpha adrenergic agonist, which prolongs analgesia and sedation. The analgesic action is due to stimulation of descending noradrenergic medullospinal pathways inhibiting the release of nociceptive neurotransmitters in the dorsal horn of spinal cord.10 The analgesic effect of clonidine is prolonged after neuraxial injection.11,12 As an adjuvant, it allows a lower concentration of the local anesthetic and prevents motor block, while it prolongs the duration of analgesia, increasing the margin of safety.13,14,15 Fentanyl is a µ receptor agonist and acts at pre and postsynaptic sites in the CNS, mainly brainstem and spinal cord, as well as outside CNS in peripheral tissues.16 Lipophilic opioids (fentanyl) have a very fast onset of action compared with lipophobic opioids (morphine) when administered along with a local anesthetic and many of their clinical actions occur well beyond the intraoperative period.17,18,19,20
We conducted this study to compare the analgesic efficacy of clonidine with fentanyl when used as an adjuvant with ropivacaine for caudal block in pediatric patients.
METHODOLOGY
This prospective randomized double blind study was conducted at our institution from June 2015 to December 2015. Sixty children, of both genders, 2 to 10 years of age, weighing 10 to 30 kg, ASA 1 and 2, scheduled for various elective infra-umbilical, perineal and lower limb surgical procedures, e.g. circumcision, herniotomy, orchidopexy, or urethroplasty etc. were included in the study. Hospital ethical committee clearance was obtained and a written informed consent was obtained from the parents of the children before commencing the study. Patients aged more than 10 years, with any contraindications to epidural anesthesia e.g. sacral spine abnormalities, local infection, coagulation disorders, hematological or neurologic disease and whose parents refused permission, were excluded from the study.
Children were randomly divided in two equal groups; Group RC and Group RF. Randomization was done by lottery method. Calculation of sample size was done by using power analysis. The non-parametric data comparison was done by Student’s t-test. Patients and their parents were blinded to the caudal medications administered. All medications were prepared by anesthesiologists who did not participate in the study. Observations were done by another group of anesthesiologists, who did not know the drugs in use.
Group RF received caudal block with inj ropivacaine (0.25%) 1 ml/kg + inj fentanyl 1 µg/kg, while Group RC received inj ropivacaine (0.25%) 1 ml/kg + inj clonidine 1 µg/kg
All patients were premedicated with oral midazolam 0.5 mg/kg 40 minutes prior to surgery. Patient was shifted into operating room, multi-parameter monitor was attached and baseline readings of heart rate (HR), oxygen saturation (SpO2), systolic blood pressure (SBP), and diastolic blood pressure (DBP) were noted. Intravenous access was achieved. Premedication with inj. glycopyrrolate 4 µg/kg, ondansetron. 0.1 mg/kg, pentazocine 0.3 mg/kg IV was done. The child was preoxygenated with 100% oxygen for 3 minutes, the induced with propofol 2 mg/kg, atracurium 0.6 mg/kg, and intubated with appropriate sized endotracheal tube. Maintainance was done with sevoflurane in oxygen 50% and nitrous oxide 50%. Caudal block was given in lateral position under all aseptic precaution with a 22 gauge hypodermic needle. After confirming the position of the needle with Whoosh test, the allocated drug was given. Administering anesthesiologist was blinded to the composition of the drug. Intra-operatively HR, SBP, DBP were noted at 5, 10, 15, 30, and 60 min
The postoperative pain relief was evaluated using FLACC scale (face, legs, activity, cry, consolability) with its 0-10 score range hourly for first 6 hours and then 4 hourly up to 24 hours. Sedation was evaluated by Ramsay score at same time intervals. If FLACC pain score > 4, inj paracetamol 15 mg/kg was given as rescue analgesia. (repeated after 6 hours if required). Duration of analgesia (time from caudal block to FLACC > 4) was noted and number of doses of paracetamol required in 24 hours were noted.
Postoperatively patients were observed in pediatric post-anesthesia care unit for 12 hrs. Side-effects, e.g. respiratory depression, motor blockade, deep sedation, shivering, hypotension, nausea and/or vomiting, were observed.
Statistical analysis: Statistical data were collected and fed in a Microsoft excel worksheet. Mean value and standard deviation were computed by using IBM SPSS Statistics for Windows, Version 20.0. Armonk, NY: IBM Corp. for age, weight, duration of surgery, duration of analgesia, HR, SBP, and DBP. Unpaired student’s t-test was used to compare mean values of two groups. A p < 0.05 was considered as statistically significant. Mann-Whitney test was used to analyze non-parametric parameters like FLACC score. Conclusion was drawn after studying the statistical analysis.
RESULTS
60 children were included (30 children in each group) in our study profile. The demographic profile of the patients in group RC and group RF was comparable with regards to age, weight and gender and on statistical analysis no significant difference was found as is clearly evident from the Table 1.
Table 1: Comparison of demographic data
| Demographic characteristics | Group RC | Group RF | P value |
| Age (years) | 5.67 ± 2.94 | 5.93 ± 2.78 |
>0.05 |
| Weight ( kg) | 14.70 ± 6.16 | 16.06 ± 5.92 | |
| Gender (M/F) | 27/3 | 28 / 2 |
Hemodynamic parameters e.g. HR, SBP, DBP, MAP and SPO2 were recorded. Comparing between both the groups, differences were not significant.
Figure 1 conveys the comparison of HR and the results were statistically not significant (P > 0.05).
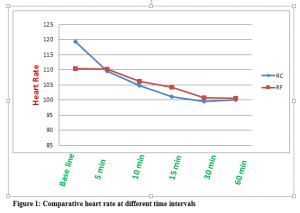
There were no significant differences between groups for heart rate (P>0.05)
Figure 2: conveys the comparison of SBP and the results were statistically not significant (P>0.05).
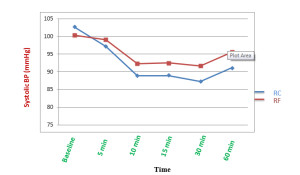
Figure 2: Comparison of systolic BP
Figure 3 conveys the comparison of DBP and the results were statistically not significant (P > 0.05).
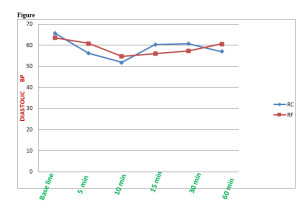
3: Comparative diastolic BP (mmHg)
No episode of hypotension and bradycardia was observed in any patient.
Oxygen saturation throughout the procedure was in acceptable range. (> 97%) {P > 0.05}.
At the end of 6 hours FLACC sore was below 4 in RF group , while it was below 4 at the end
of 16 hours in RC group. Thus difference was statistically significant (P > 0.05).
As is evident from the Figure 4, Comparable mean FLACC score in both the groups were
Significant (p<0.05). Values were lower in Group RC and the difference was found to be statistically significant (p <0.05)
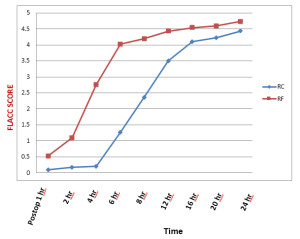
Figure 4: Comparison of FLACC scores
Values of Ramsay sedation score were lower in Group RF and the difference was found to be statistically significant (P< 0.05).
The mean duration of analgesia was 889.8 ± 42 vs. 318 ± 42 min in Group RC vs. Group RF respectively and the difference was statistically significant (p<0.0001)
There were minimal side effects observed in both groups; Vomiting was noted in 1 patient in Group RC, compared to 2 patients in Group RF, and the difference was statistically significant (P < 0.05) Urinary retention, respiratory depression or any other complication was not observed in any of the patients in both groups.
DISCUSSION
Caudal analgesia is one of the simple and most commonly performed regional blocks for providing analgesia in pediatric patients. It is a safe and reliable technique used for intra and postoperative analgesia in children undergoing abdominal and lower limb surgeries.6,7 Various doses of clonidine ranging from 1-5 µg/kg have been used for epidural analgesia. We preferred a dose of 1 µg/kg of clonidine in our study as many studies showed that increasing the dose of 1to 2µg/kg did not enhance the analgesic efficacy of this drug,21 but it increased the incidence of adverse effects e.g., bradycardia and hypotension with increasing dose.22 Many researchers concluded that co-administration of clonidine with local anesthetics improves the quality of peripheral nerve blocks.23,24 An addition of clonidine prolonged analgesia significantly.
Clonidine induced prolongation of caudal analgesia with bupivacaine is mainly due to anti nociceptive action which is due to direct suppression of the spinal cord nociceptive neurons by epidural clonidine. Clonidine also suppresses neurotransmission in peripheral, sensory Aδ and C nerve fibers. The final mechanism suggested is pharmacokinetically mediated: clonidine induces vasoconstriction to α-2b adrenoceptors located at peripheral vascular smooth muscles.
Caudal clonidine causes sedation, which is mainly dose dependent. Activation of alpha-2 adrenergic receptors in locus cerulus results in sedation. Increase in concentration of GABA secretions causes CNS depression.
Ivani G et al25 reported that 2 mg/kg of 0.2% ropivacaine is sufficient to obtain sensory block for lower abdominal or for genital surgery in children. Ropivacaine 0.25% 1 ml/kg by caudal route produces a maximal plasma concentration of 0.72 ± 0.24 mg/lit, which is much lower than the maximal-tolerated plasma concentration of ropivacaine in adult volunteers (2.2 ± 0.8 mg/lit). Therefore, we have chosen 0.25% 1 ml/kg ropivacaine for our case study. This concentration was sufficient to provide analgesia.
In our study, we have seen that caudal ropivacaine alone provided excellent analgesia in the early postoperative period. The effect wore off approximately 6 hours after an operation in cases where fentanyl was added as an adjuvant, and supplemental analgesics were required. An addition of clonidine prolonged analgesia significantly (15 hrs). Rescue analgesia was not required.
Arpita et al in their study concluded that addition of clonidine to ropivacaine in caudal block prolonged analgesia up to 975 ± 40.5 min.26
Regarding hemodynamics, we did not observe any significant difference in mean HR, SBP, DBP between the two groups, which corroborated to the study result obtained by Bajwa SJS et al.27 No difference was found regarding postoperative sedation between two groups, which matched with our study. No adverse effects were noted in any patient of either group. Ivani et al also showed that 0.1% ropivacaine with clonidine 2 µgm/kg is associated with an improved quality of postoperative analgesia compared to plain 0.2% ropivacaine.
Fentanyl causes least respiratory depression when given extradurally because of high lipid solubility. A bupivacaine─fentanyl mixture as a single caudal epidural injection does not change onset, quality and duration of analgesia, and sedation score. A higher dose of 2 µg/kg when added to 0.25% bupivacaine for single injection in children causes vomiting and desaturation. To prolong the duration of analgesia with minimal side effects because the mean duration of analgesia provided with even longer acting local anesthesia is limited, fentanyl, a lipophilic opioid, is very commonly used as an additive to local anesthetics in children. Although there is no debate about its beneficial effects, side effects like respiratory depression, nausea and vomiting are common.
Koul A et al28 found significant prolongation of postoperative analgesia with an addition of clonidine with bupivacaine caudally. The addition of clonidine and fentanyl to ropivacaine in single shot caudal epidural definitely prolongs duration of analgesia, but quality and duration of analgesia is found to be more superior in RC group than RF group.
CONCLUSION
We conclude that a single shot caudal injection of clonidine (1 μg/kg) added to ropivacaine 0.25% offers an advantage of prolonged postoperative pain relief over 0.25% ropivacaine with fentanyl in children undergoing lower abdominal surgery, without increasing the incidence of adverse effects.
Conflict of interest: None declared by the authors
REFERENCES
- Merkel SI, Voeoel- Lewus T, Shayevitz JR, Malviya S. The FLACC: A behavioral scale for scoring postoperative pain in young children. Paediat Nurs. 1997;23:293. [PubMed]
- Rogers M. Do the right thing –pain relief in infants and children. N Engl J Med. 1992;326:55-56. [PubMed] [Free full text]
- Choonara I. Pain relief. Arch Disease Child 1989;64;1101-1102 [PubMed] [Free full text]
- Verghese ST, Hannallah RS. Postoperative pain management in children. Anesthesiol Clin North America 2005;23:163-84 [PubMed]
- Habre W, Bergesio R, Johnson C, Hackett P, Joyce D, Sims C. Pharmacokinetics of ropivacaine following caudal analgesia in children. Paediatr Anaesth 2000;10:143-7. [PubMed] DOI: 10.1046/j.1460-9592.2000.00454.x
- Yildiz TS, Korkmaz F, Solak M, Toker K. Clonidine addition prolongs the duration of caudal analgesia. Acta Anaesthesiol Scand 2006;50:501-4. [PubMed] [Free full text] DOI: 10.1111/j.1399-6576.2005.00941.x
- Tripi PA, Palmer JS, Thomas S, Elder JS. Clonidine increases duration of bupivacaine caudal analgesia for ureteroneocystostomy: A double-blind prospective trial. J Urol 2005;174:1081-3. [PubMed]
- Mazoit JX, Dalens BJ. Pharmacokinetics of local anaesthetics in infants and children. Clin Pharmacokinet. 2004;43(1):17-32. [PubMed]
- Malinovsky JM, Lepage JY, Cosian A, Mussini JM, Pinaudt M, Souron R. Is ketamine or its preservative responsible for neurotoxicity in rabbit? Anesthesiology 1993;78:101-5. [PubMed] [Free full text]
- Cook B, Dayle E. The use of additives to local anaesthetic solutions for caudal epidural blockade. Paediatr Anaesth 1996;6:353-9. [PubMed] DOI: 10.1046/j.1460-9592.1996.d01-3.x
- Bonnet F, Boico O, Rostaing S, Loriferne JF, Saada M. Clonidine induced analgesia in post operative patients; epidural versus intramuscular administration. Anesthesiology 1990;72:423-7. [PubMed] [Free full text]
- Eisenach J, Detweiter D, Hood D. Haemodynamic and analgesic action of epidurally administered clonidine. 1993 Feb;78(2):277-87. [PubMed] [Free full text]
- Tsui BC, Berde CB. Caudal analgesia and anaesthesia techniques in children. Curr Opin Anaesthesiol 2005;18:283-8. [PubMed]
- Hansen TG, Henneberg SW, Walther-Larsen S, Lund J,Hansen M. Caudal bupivacaine supplemented with caudal or intravenous clonidine in children undergoing hypospadias repair: A double-blind study. Br J Anaesth 2004;92:223-7. [PubMed] [Free full text] doi: 1093/bja/aeh028
- Ivani G, De Negri P, Conio A, Amati M,Roero S, Giannone S, et al. Ropivacaine-clonidine combination for caudal blockade in children. Acta Anaesthesiol Scand 2000;44:446-9. [PubMed] DOI: 10.1034/j.1399-6576.2000.440415.x
- Pert CB, Synder S. Opiate receptors; demonstration in nervous tissue. Science 1973;179(4077):1011-4. [PubMed] DOI: 10.1126/science.179.4077.1011
- Bohannon TW, Estes MD. Evaluation of subarachnoid Fentanyl for postoperative analgesia. Anesthesiology 1987;67:A237.
- Normura MK, Mokriski BK, Malinow AM. Effect of epinephrine on intrathecal fentanyl analgesia. Reg Anesth 1989;14:20-25.
- Hunt CO, Naulty JS, Bader AM, Hauch MA, Vartikar JV, Datta S, et al. Perioperative analgesia with subarachnoid fentanyl-bupivacaine for ceaserian delivery. Anesthesiology 1989;71:535-540. [PubMed] [Free full text]
- Leighton BL, DeSimone ChA, Norris M, Ben-David B. Intrathecal narcotics for labor revisited: the combination of fentanyl and morphine intrathecally provides rapid onset of profound, prolonged analgesia. Anesth Analg 1989;69:122-125. [PubMed]
- Klimscha W, Chiari A, Michalek-Sauberer A, Wilding E, Lerche A, Lorber C, et al. The efiicacy and safety of a clonidine / bupivacaine for pediatric hernia repair. Anesth Analg 1998;86(1):54-61. [PubMed]
- Breschan C, Krumphoiz R, Likar R, Kraschi R, Schalk HV. Can a dose of 2 µg/kg caudal clonidine cause respiratory depression in neonates? Paediatr Anaesth 1999;9:81-3. [PubMed]
- El Saied AH, Steyn MP, Ansermino JM. Clonidine prolongs the effect of ropivacaine for axillary brachial plexus blockade.Can J Anaesth. 2000;47:962–7. [PubMed] [Free full text]
- Ivani G, Conio A, de Negri P, Eksborg S, LoÈnnqvist PA. Spinal versus peripheral effects of adjunct clonidine: Comparison of the analgesic effect of a ropivacaine-clonidine mixture when administered as a caudal or ilioinguinal-iliohypogastric nerve blockade for inguinal surgery in children.Paediatr Anaesth.2002;12:680–4. [PubMed] DOI: 10.1046/j.1460-9592.2002.00935.x
- Ivani G, Mereto N, Lampugnani E, Negri PD, Torre M, Mattioli G, et al. Ropivacaine in paediatric surgery: Preliminary results.Paediatr Anaesth. 1998;8:127–9. [PubMed] DOI: 10.1046/j.1460-9592.1998.00246.x
- Arpita Laha,Samila Ghosh, and Haripada Das. Comparison of caudal analgesia between ropivacaine and ropivacaine with clonidine in children. Saudi J Anaesth. 2012 Jul-Sep;6(3):197–200. [PubMed] [Free full text] doi: 10.4103/1658-354X.101199.
- Bajwa SJ, Karun J, Bajwa SK, Bakshi G, Singh K, Panda A. Caudal ropivacaine-clonidine: A better post-operative analgesic approach.Indian J Anaesth. 2010;54:226–30. [PubMed] [Free full text] doi: 10.4103/0019-5049.65368.
- Koul A, Pant D, Sod J. Caudal Clonidine in Day-Care Paediatric Surgery.Indian J Anaesth.2009;53:450–4. [PubMed] [Free full text]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube