
Atul Samaiya, MS, DNB, MNAMS, EBSQ, FICS*, Nupur Chakravorty, MD**, Vivek Madhav Kanhare, MS, MCh***, Devashish Chakravarty, MD, PDCC****,Renu Singh, MS*****
*Consultant Oncosurgeon, Department of Surgical Oncology, Navodaya Cancer Hospital, Bhopal, MP (India)
**Associate Professor, Department of Anesthesiology & Critical Care, L.N. Medical College, Bhopal, MP-462042 (India)
***Consultant cardiac surgeon, Department of Cardiothoracic Vascular Surgery, Chirayu Medical College & Hospital, Bhopal, MP-462042 (India)
****Consultant cardiac anesthesiologist, Chirayu Medical College & Hospital, Bhopal, MP-462042 (India)
*****Consultant Oncosurgeon, Jawaharlal Nehru Cancer Hospital & Research Centre, Bhopal, MP-462042 (India)
Correspondence: Dr. Nupur Chakravorty, MD, Associate Professor, Department of Anesthesiology & Critical Care, L.N. Medical College, Bhopal, MP-462042 (India); E-mail: drnupurc@yahoo.com
ABSTRACT
Anesthetic management of patients with intratracheal mass lesions is fraught with pitfalls if the inherent problems are not anticipated and prepared for. We present here a case of a lower tracheal tumor near the carina undergoing general anesthesia for surgical resection with tracheal anastomosis. A brief review of pertinent literature is also included.
Keywords: Tracheal tumors; Anesthetic management.
Citation: Samaiya AS, Chakravorty N, Kanhare VM, Chakravarty D, Singh R. Surgical resection of intratracheal tumor: challenges in perioperative management. Anaesth Pain & Intensive Care 2015;19(1):57-59
INTRODUCTION
Primary cystic adenoid carcinomas of trachea account for less than one third of adult primary tracheal tumors. Most of these tumors are described in upper trachea and juxtacarinal location for this type of tumors is very rare. Surgical resection of these juxtacarinal tumors is an anesthetic as well as surgical challenging task requiring maintenance of a patent airway, a visible and approachable operative field, control of bleeding and prevention of tumor tissue moving distally into tracheobronchial tree. A successful outcome in these cases requires a meticulous planning and good interaction between surgical and anesthetic teams.
CASE REPORT
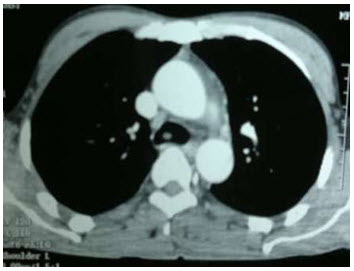
A 34 year non-smoker male patient with a history of chronic tobacco chewing presented with a history of cough for 2 years, progressive dyspnea and wheeze for the last 6 months. Fibreoptic bronchoscopy revealed a polypoidal mass in the lower trachea just near the carina, projecting into the lumen with narrowing of trachea at that level. The biopsy confirmed a diagnosis of primary low grade adenoid cystic carcinoma. Computed tomography scan revealed a 3.4×2.8 cm polypoidal mass in the lower trachea, involving right lateral tracheal wall, reaching up to 1.2 cm above the carina, adherent to the azygous vein and abutting the superior vena cava (Figures 1-A & B).
Figure 1-A: CT scan showing tumor

Figure 1-B: Another frame of CT scan showing tumor
Excision of mass and resection anastamosis of trachea under general anesthesia with standby heart lung machine was planned. On preoperative evaluation, patient could lie in the supine position without any observable distress. He had mild inspiratory stridor, and bilateral wheeze with occasional crepitations. On room air patient’s arterial saturation (SpO2) was 91% while the arterial blood gas analysis showed a PaO2 of 85 mmHg, PaCO2 40 mmHg and pH 7.42. All other blood and biochemical investigations were within normal range.
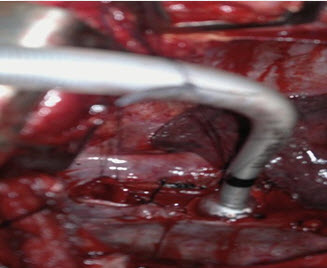
In the operating room the patient was counselled and premedicated with inj. glycopyrrolate 0.2 mg. Intravenous fluids were started and standard monitoring devices attached. Central venous pressure monitoring and an intra arterial line for blood pressure and blood gas monitoring were set up. After airway preparation with 4% lignocaine spray and 10% lignocaine viscous, patient was sedated with titrated doses of inj. fentanyl, midazolam and propofol. We then did a fibreoptic bronchoscopy maintaining spontaneous respiration and passed a size 7.0 mm ID endotracheal tube (ETT) keeping the tip of the tube above the growth. Ventilation was confirmed clinically and by capnography, after which patient was given inj. atracurium 0.3 mg/kg and he was mechanically ventilated. Right muscle sparing posterolateral thoracotomy was done via 4th intercostal space. A 3×3 cm tracheal mass was seen in lower trachea upto the tracheal bifurcation. Adherent azygous vein was ligated and trachea separated from the superior vena cava, with preservation of the left recurrent laryngeal nerve. Lower end of trachea was transected above the carina, and a sterile size 6.0 mm cuffed ETT inserted by the surgeon via incision into left bronchus (Figure 2). Isolated left lung ventilation was done. At the upper end, the surgeon transected the trachea 5 mm above the tumor and removed the mass. Trachea was then approximated and end to end anastomosis performed at the carinal level after inferior pulmonary ligament release. When surgical anastomosis was almost complete, the thoracic ETT was withdrawn, orotracheal tube was manipulated past the incision and patient was ventilated through it till surgical anastomosis was completed. Total surgical procedure took around 150 min during which adequacy of gas exchange was monitored by oxygen saturation, end tidal carbon dioxide and with arterial blood gases.
Figure 2: ETT inserted via tracheal incision.
Postoperatively patient was electively ventilated for 24 hrs and remained stable. Mild air leak was present for 48 hours but no significant changes were seen in clinical monitors as well as arterial blood gases. Patient was extubated and discharged on 15th postoperative day. Histopathology confirmed adenoid cystic carcinoma with perineural invasion with free margins. Patient was put on radiotherapy sessions after 7 weeks which concluded in September 2013. Patient is recurrence free till this time.
DISCUSSION
Primary tracheal tumors comprise 0.3% of all bodily tumors1 with cystic adenoid carcinomas of trachea accounting for < 1% of respiratory tract tumors. Since these tumors usually occupy more than 75% of the tracheal lumen when patients become symptomatic2 it is a challenge for the anesthesiologist to maintain a viable airway before and during induction, provide visible operative field, and prevent tumor tissue being pushed through. distally into tracheobronchial tree during resection. Anesthesia strategies described for management of airway during surgical resection of these tumors include the use of fibreoptic intubation, laryngeal mask airway, high frequency jet ventilation, tracheostomy under local anesthesia, and cardiopulmonary bypass.3,4 Tracheal mass present at a lower level can have more complicated management of airway, anesthesia and the surgery for successful and safe removal of the mass.5
Although we had a heart lung machine ready on standby, since upper trachea was patent, we decided to intubate the patient. If ventilation through orotracheal tube had been unsatisfactory, as shown by high airway pressures or hypercarbia, we would have established femorofemoral bypass. Femorofemoral bypass has been used in cases of obstructed airway where it is not possible to initiate any manoeuvre to maintain airway by endotracheal intubation.4 We did not do a preoperative tracheostomy since the lower position of the mass would not have provided any extra benefit on ventilation through a tracheostomy. Awake fibreoptic intubation was done to ensure airway patency. Propofol infusion was necessary for adequate sedation to prevent any stimulation of the airway which could cause complete obstruction. We preferred intravenous induction with propofol over inhalational induction as the latter can sometimes lead to airway irritation.6 Muscle relaxation was also a demand of the surgical procedure which we were compelled to take with all due precautions to detect and prevent loss of gas exchange.
Surgical procedures like use of Nd- Yag laser have been used to remove these tumors.5 In our case we did not have this facility and financial constraints did not allow the patient to proceed to a centre with this facility. Open resection was the only option to protect the patient from imminent asphyxia and restore airway patency. Primary operation of resectable masses along with adjuvant radiotherapy, as was done in our case, has been found to have better disease specific and overall survival rates, as compared to radiotherapy with or without chemotherapy,7 which reinforced our decision. No involvement of adjacent lymph nodes was also a decisive factor to operate.
CONCLUSION
Primary juxtacarinal tumor of the trachea is a challenge both to the surgeon and more so to the anesthesiologist, who has to ensure a patent airway and effective gas exchange throughout the procedure. A good perioperative plan with a back up in place and continuous interaction between surgical and anesthesiology team workers is essential in these cases for a safe and effective outcome.
REFERENCES
- Caiadoa A, Moura e Sá J. Tracheal tumors review – a clinical case of adenoid cystic carcinoma. Rev Port Pneumol 2008 Jul-Aug;14(4):527-34. [PubMed]
- Madan K, Agarwal R, Bal A, Gupta D. Bronchoscopic management of a rare benign endobronchial tumor. Rev Port Pneumol 2012;18:251-4.[PubMed] [Free full text] doi: 10.1016/j.rppneu.2012.02.003.
- Divatia JV, Sareen R, Upadhye SM, et al. Anaesthetic management of tracheal surgery using the laryngeal mask airway. Anaesth Intensive Care 1994;22:69–73. [PubMed]
- Goyal A, Tyagi I, Tiwari P, Agarwal SK, Syal R. Management of difficult airway in intratracheal tumor surgery. BMC Ear Nose Throat Disord. 2005 June 7;5:4. [PubMed] [Free full text]
- Azorin J, Lamberto JF, Personne C, Larmignat P, Khellaf M, Kmeny JL, et al. Adenoid cystic carcinoma of the trachea: Treatment by combined laser therapy and surgery. Rev Mal Respir 1987;4:95-6. [PubMed]
- Conacher ID. Anaesthesia and tracheobronchial stenting for central airway obstruction in adults. Br J Anaesth. 2003;90:367–74. [PubMed] [Free full text]
- Webb BD, Walsh GL, Roberts DB, Sturgis EM. J Am Coll Surg. 2006 Feb;202(2):237-46. [PubMed]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube