
Mohammad Irfan Akhtar1, Ali Sarfraz Siddiqui2, Muhammad Faisal Khan2
1Associate Professor; 2Assistant Professor
Department of Anesthesiology, Aga Khan University Hospital, Stadium Road, P.O. Box 3500. Karac hi 74800 (Pakistan)
Correspondence: Dr Mohammad Irfan Akhtar,
Associate Professor, Department of Anesthesiology,
Aga Khan University Hospital, Stadium Road, P.O. Box 3500. Karac hi 74800 (Pakistan); E-mail: mohammad.irfan@aku.edu
ABSTRACT
Introduction: Oxygen supplementation in post anesthesia care unit (PACU) is a safe, simple and effective method to ensure adequate oxygenation in most patients recovering from anesthesia. Despite dearth of clinical studies demonstrating the need for routine oxygen therapy in every postoperative patient, routine administration of oxygen is common in the PACU irrespective of the type of surgery, physical status of patient or technique of anesthesia employed, thus wasting important resource. The study was conducted to observe supplemental oxygen administration practices to adult patients in PACU of a tertiary care teaching hospital.
Methodology: This was a prospective observational study with inclusion of all adult American Society of Anesthesiologists (ASA) physical status I, II, and III patients undergoing general anesthesia and central neuraxial blocks being shifted to PACU. Institutional ethical review committee approval was taken. A trained research assistant collected data with defined variables in PACU of a tertiary care hospital in a specially designed form.
Results: A total of five hundred and eighty five adult patients were enrolled in this study. Four thirty one (74%) patients received supplemental oxygen in PACU. Among 431 patients who received supplemental oxygen in recovery room, 373 (86%) patients received oxygen therapy without any specific reason. In fourteen patients (2.4%), transient hypoxemia was observed, increasing oxygen flow and addressing the underlying cause managed that.
Conclusion: Supplemental oxygen practice was not standardized in the PACU. Majority of the patients received oxygen supplementation without any specific clinical indication. Hypoxic event in PACU is not common and can easily be managed with vigilant monitoring and timely intervention.
KeyWords: Post anesthesia care unit, Supplemental Oxygen, Practices.
Citation: Akhtar MI, Siddiqui AS, Khan MF. Supplemental oxygen administration practices in post anesthesia care unit of a tertiary care hospital: an observational prospective study. Anaesth Pain & Intensive Care 2018;22(2):174-179
Received: 21 Nov 2017, Reviewed: 8 Jun 2018, Corrected: 21 Jun 2018, Accepted: 21 Jun 2018
INTRODUCTION
The importance of post anesthesia care unit (PACU) is well established in the prevention and proactive management of post-operative anesthetic and surgical complications thus facilitating safe discharge of the surgical patients to the ward or home. Oxygen supplementation in the PACU is a safe, simple and usually effective method to ensure adequate oxygenation in most patients recovering from anesthesia. Despite the lack of studies demonstrating the need for routine oxygen therapy in every postoperative patient, routine administration of oxygen is common in the post-anesthesia recovery room irrespective of the type of surgery, physical status of patient or technique of anesthesia employed. The incidence of hypoxemia in PACU ranges from 12%-30% depending upon the cut-off of 94-92% SpO2 for defining desaturation.1 American Society of Post-anesthesia Nurses adapted standards requiring the use of pulse oximetry in the recovery room setting. Consultants and members of American Society of Anesthesiologists are equivocal regarding routine administration of supplemental oxygen in the post-anaesthesia care unit but they recommend administration of supplemental oxygen in the recovery room to patients at risk of hypoxemia.2
There is evidence available that oxygen is not needed in up to 63% of patients during the immediate postoperative period. Gift et al. recommended that oxygen saturation levels should be noted at the time of admission to the PACU and those patients with oxygen saturations of 92% or less should be given oxygen therapy. Oxygen at 4 litres/minute via nasal cannula maintains adequate oxygen saturation levels.3 Supplemental oxygen should be used when needed. Pulse oximetry provides objective value to determine the need for oxygen supplementation. The use of pulse oximetry in the PACU helps identifying hypoxemic patients and selectively recommending oxygen therapy.4
In the current evidence-based medical practice, there is an increasing understanding of acknowledging oxygen as a drug with specific biochemical and physiologic actions.5 Several factors have been identified in literature that predispose patient to hypoxemia in the immediate postoperative period like patients factors, anesthetic technique and surgery. Keeping in mind these factors will help in identifying patients who are more prone to develop hypoxemia and should be more closely monitored by the PACU staff. Such patients may receive prophylactic oxygen therapy.6
Significant cost savings can be done if supplemental oxygen is used judiciously. In this time of economic pressure on medicine and routine availability of SpO2 monitors in the PACU, it is time to rethink our use of routine supplemental oxygen in PACU patients.7
The objective of the study was to evaluate supplemental oxygen administration practices to adult patients in post anesthesia care unit of a tertiary care hospital. Our study hypothesis was based on our observation that there was a large proportion of unjustified oxygen supplementation in PACU resulting in wastage of an important medical resource.
METHODOLOGY
This Prospective observational study was conducted in the main PACU of a tertiary care hospital from October to December 2016, after approval from Ethical review Committee (Protocol Ref. number: 4350-Ane-ERC-16). A total of 585 patients were enrolled for the study. All adult patients having ASA physical status I, II and III patients brought to post anesthesia care unit (PACU) of main operation theatres after elective surgery under general anesthesia and central neuraxial blocks (Spinal and Epidural) were included in this study. Pediatric surgical patients, patients with hemodynamic instability, and the patients undergoing cardiothoracic surgery, caesarean delivery and craniotomy were excluded from this study. Primary outcome of the study was to see the extent of unjustified oxygen administration in the PACU and secondary outcome was to see the incidence of hypoxic events in the PACU.
According to the hospital’s PACU policy, all patients coming to PACU after general anesthesia receive supplemental oxygen through facemask. In each patient, ASA standard monitoring was routinely done in the PACU including electrocardiogram (ECG), percentage oxygen saturation (SpO2), non invasive blood pressure (NIBP) on arrival, every 10 minutes interval or whenever needed till discharge from PACU.
Hypoxemia was defined as SpO2 of 90% and partial pressure of oxygen (PaO2) of 60 mm Hg on breathing room air for more than 30 seconds. Oxygen Supplementation is defined as oxygen administration through nasal prong or Hudson facemask at 1-5 liters/minute or 6-10 liters/minute respectively. Irrational oxygen supplementation was defined as oxygen administration at room air saturations of 94% or more.
A trained research assistant collected the data in a specially designed form. The research assistant monitored oxygenation with the pulse oximetry continuously and recorded the SpO2 values in the form during the stay of selected patient in PACU. Patient confidentiality was maintained by mentioning only medical record number (MR#) in the form. The primary investigator for safe record possession kept all the forms. Patient’s age, sex, weight, height, ASA physical status, comorbid condition, diagnosis, type of surgical procedure, duration of surgery and anesthetic technique used were all noted in the form. If hypoxic event occurred in any adult patient under observation in PACU, its cause and management were also noted in the form.
All statistical analyses were performed using Statistical Packages for Social Sciences version 19 (SPSS Inc., Chicago, IL). Mean and standard deviation were computed for age, height, weight, and BMI. Frequency and percentage were computed for gender, ASA status, anesthetic technique, oxygen supplementation and reason for oxygen supplementation.
RESULTS
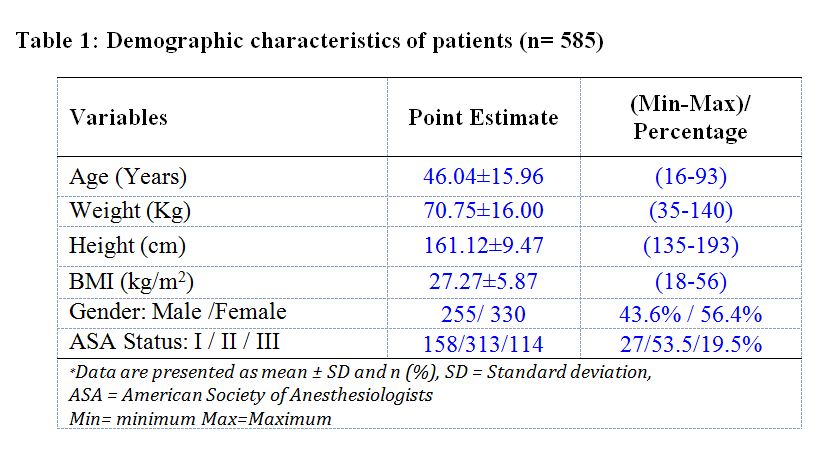
A total of five hundred and eighty five adult patients were enrolled and analyzed in this study. Two hundred and fifty five (43.6%) were male patients while three hundred and thirty (56.4%) were female (Table 1).
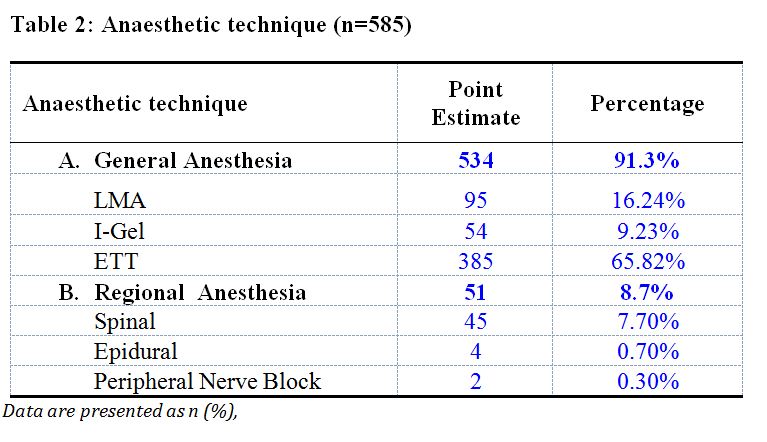
Anesthesia techniques were variable as per the need of surgical procedure and choice of anesthetist (Table 2).
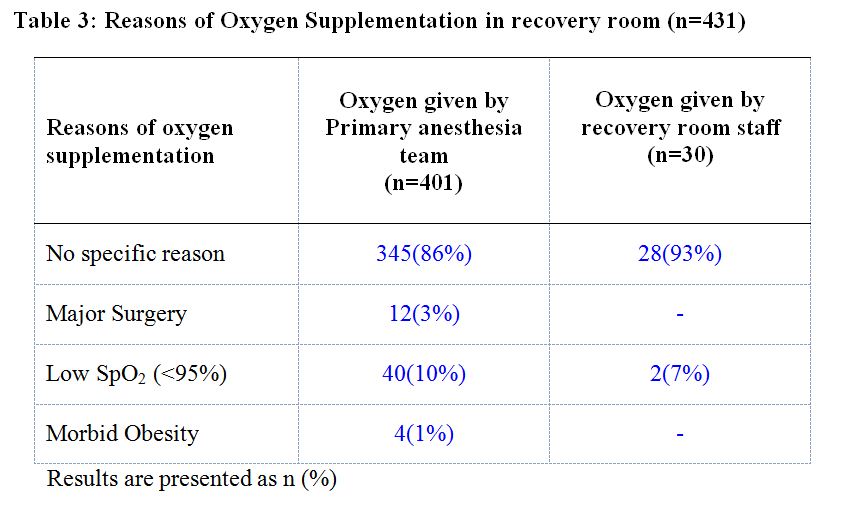
In the PACU, supplemental oxygen therapy was ordered by the primary anesthesia team in 401 (74%) patients while in 30 (6%) patients recovery staff provided supplemental oxygen (Figure 1). There were 87% patients (373/431) who received oxygen therapy without any specific reason (Table 3).
In this study, incidence of hypoxemia in PACU was only 2.4%. Hypoxia was transient and all patients responded to appropriate oxygen therapy without any hypoxic damage. Majority were general surgical and ENT surgery patients with age > 50 years or body mass index (BMI) >35 kg/m2 or combination of both.
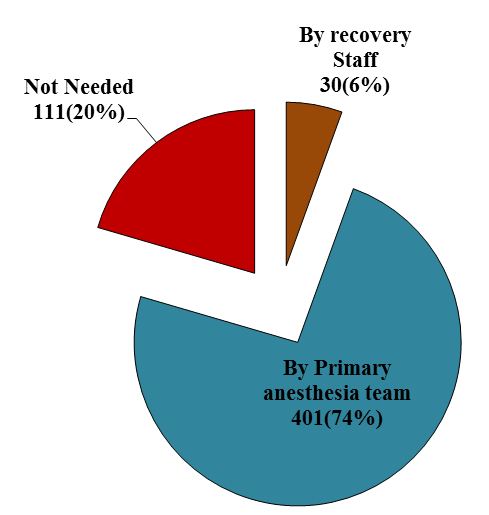
Figure 1: Oxygen supplementation given in recovery room (n=542)
Majority of patients (approximately 80%) received supplemental oxygen through Hudson mask while others via nasal prong. Mean duration of oxygen therapy in PACU in the study was 31 minutes with oxygen flow ranging from 6 to 10 liters/min.
DISCUSSION
The study has demonstrated the magnitude of the irrational supplemental oxygen administration to patients in PACU of a tertiary care hospital. It is important to understand the rationale of oxygen administration for standardized goals of preventing hypoxemia, to reduce the work of breathing and to reduce myocardial work. With the advent of evidence based clinical practice, administration of supplemental oxygen to the PACU patients must be standardized.
Literature shows that postoperative hypoxemia is caused by inadequate ventilation as a result of residual effects of anesthetic agents and use of neuromuscular blocking drugs. This adds to mismatch in ventilation/perfusion ratio caused mainly by atelectasis zones in lung-dependent regions.8 Other causes may include low cardiac output states, anemia, shivering, pain and agitation.9 The Canadian Anesthesiologists’ Society, American Society of Anesthesiologists (ASA), World Federation of Societies of Anesthesiologists, and the World Health Organization, as a standard of care monitoring in the intraoperative and immediate postoperative period, have advocated pulse oximetry.10,11 Much of decline in the hypoxic events is attributable to improvements in the safety of anesthesia administration and monitoring, including the nearly universal use of pulse oximetry that has been associated with the earlier diagnosis and correction of hypoxemia.
Pulse oximetry has contributed to the improved identification of hypoxemia and cardiac events in PACU. It is now a standard monitor that guides oxygen flow in recovery and after discharge in surgical ward, but without any influence on postoperative mortality or complication rate.4 SpO2 limit of 94% was related to hypoxemia in 15%12 and 37%7 of patients. With SpO2 limit of 94%, patients after general anesthesia without supplemental oxygen in the PACU had higher incidence of hypoxemia (44.7%) than patients after regional anesthesia (24%). Even patients after general anesthesia with supplemental oxygen showed hypoxemia (26.1%).13 In studies with 92% as SpO2 limit, the incidence of hypoxemia was 7%, 15% and 23.14% of patients.14-16 After gynecological laparoscopic surgeries, keeping SpO2 limit of 94%, only15% of patients needed supplemental oxygen in PACU.12
Evidence showed that the variables that have significant association with immediate postoperative hypoxemia include ASA physical status III, age > 55 years, history of COPD, SpO2 < 95% preoperatively, general anesthesia, inability to keep hand grip for 15 seconds and clinical signs of inadequate ventilation. Regional anesthesia, with or without perioperative sedation with diazepam or midazolam was related to lower incidence of immediate post-operative hypoxemia.16
Identification of post-operative patients at risk of hypoxemia should be identified. In accordance with our study findings, literature has demonstrated that elderly patients have special considerations in relation to post-operative hypoxemia due to decrease in respiratory reserve, mechanical changes in the chest wall and changes in pulmonary volumes and capacities.17 Older adults are more sensitive to depressing effects of inhalational anaesthetics, sedatives and opioids, so the incidence of post-operative hypoxemia is higher in this group of patients.18
Monitoring patient’s oxygenation with pulse oximetry and detecting hypoxemia also depends on the level of motivation of PACU staff to detect it.19 It is possible that the recognition of factors leading to hypoxemia could be used to educate and encourage PACU staff aiming at improving surveillance and patients monitoring, thus detecting hypoxemic episodes and early managing them.
Respiratory complications in the post anesthesia period result in morbidity and mortality thus consolidating the need for vigilant monitoring. In the PACU respiratory complications are secondary to major unanticipated ventilation problems, including hypoxemia, hypoventilation (respiratory rate <8 breaths/min or arterial carbon dioxide partial pressure [PCO2] >50 mmHg) or upper-airway obstruction (laryngospasm or stridor), that necessitates a physical or pharmacological treatment (e.g. insertion of an oral/nasal airway, ventilation, tracheal intubation, opioid antagonism, muscle relaxant reversal).7 Pulmonary complications including hypoxemia may even be more likely than cardiac complications to predict long-term mortality after surgery in high-risk population.20 High risk patients for post-operative hypoxemia in context of preoperative assessment, type of surgery and intraoperative course should be identified and triaged accordingly in the PACU for supplemental oxygen therapy, thus separating them from low risk patients for postoperative hypoxemia. Careful monitoring with a pulse oximetry and giving oxygen if appropriate are essential to prevent desaturation during early postoperative period.21
In a study keeping SpO2 94% as cut off, the incidence of hypoxemia on arrival in PACU was 12%.22 The study concluded that postoperative oxygen therapy should be reserved for patients with SpO2 of < 94 % on arrival in the PACU. Significant cost saving can be done by appropriately providing oxygen supplementation to patient in need and avoiding from those patients who do not require it.22 The study has consolidated our suggestion to administer supplemental oxygen when it is required. Di Benedetto RJ et al. emphasized the administration of oxygen in PACU based on pulse oximetry values (SpO2 < 94%) and suggested considerable cost savings without compromising patient care. They showed in their study that supplemental oxygen was unnecessary in 63% of patients for the duration of their PACU stay. Cost savings to the 307 patients in one study not receiving oxygen was $31,928 if it had been billed separately.7
In the current study, incidence of hypoxemia was only 2.4% (SpO2 less than 94%). Hypoxia was transient and all patients responded to oxygen therapy without any hypoxic damage. The major cause of transient hypoxia was morbid obesity and age greater than 50 years. It was more common in patients undergoing laparotomies and ENT surgeries.
Monitoring using pulse oximetry is now standard of care practice in the PACU. It is now time to apply the objective data it supplies, thereby creating cost savings while maintaining patient care standards. Unnecessary application of oxygen face mask, when patient is recovering from anesthesia and getting awake at times, is uncomfortable for patients. Some patients may get claustrophobic due to its application.
Unjustified oxygen supplementation has resource wastage impact. If oxygen is delivered at a rate of 6 liter/minute for half an hour (which is observed as mean duration of supplemental oxygen in this study), it results in consumption of 180 liters of oxygen. In our hospital if patient receives oxygen supplementation in PACU he/she will be charged approximately 10 USD. Routinely around 30 elective patients admitted in PACU daily, so it becomes 300 USD per day and multiplying it for a month then it would be 9000 USD per month. Hence, using oxygen supplementation out of habit and without specific clinical indication will have huge financial impact. On the other hand if we provide oxygen to our PACU patients appropriately for specific indication and with justification then we may be saving cost as well as important medical resource.
With the proof of oxygen as a drug, it should be administered cautiously and in critical cases should be improvised as per the individual patient needs. As healthcare professionals, oxygen should not be administered merely on verbal orders, instead should be prescribed with written orders with specified flow rate, and duration keeping in mind the side effects that can occur as a result of prolonged oxygen therapy.
Oxygen supplementation may have false sense of security regarding appropriate oxygenation and ventilation. In patients with regular spontaneous ventilation, supplemental oxygen often masked the ability to detect abnormalities in respiratory function in the PACU. Without the need for capnography and arterial blood gas analysis, pulse oximetry is a useful tool to assess ventilatory abnormalities, but only in the absence of supplemental inspired oxygen. In patients able to maintain SpO2 > 90% on a Fraction of inspired oxygen (FiO2) of 0.21, pulse oximetry monitoring during room air breathing is a useful tool to assess ventilation, without the need for capnography or arterial blood gas analysis.23
The limitation of the study was that it was an observational study limited to PACU stay of the post-surgical patients who were in ASA I, II, and III physical status. The patients were not followed in the ward or special care to monitor any desaturation events plus the intervention done. Pulse oximetry has well-known technical limitations and various sources of artifact that may have influenced the quality of our data. Sensor malposition can lead to apparent hypoxemia. Poor peripheral perfusion, hypothermia, shivering, hypotension, and advanced age have been shown to yield low-quality pulse oximetry readings.24
The study has demonstrated the scope of the problem with suggestions for future direction to rationalize supplemental oxygen in the PACU of the national tertiary care hospitals, by formulating nationwide guidelines.
CONCLUSION
This study showed that the supplemental oxygen practice is not standardized in the PACU. Majority of the patients received oxygen supplementation without any specific clinical indication. Hypoxic events in PACU are not common in the presence of vigilant healthcare staff with optimal monitoring and if they occur, they can easily be managed with timely intervention. Hence guidelines need to be formulated to standardize this clinical practice thus avoiding the wastage of an important resource.
Conflict of interest: None declared by the authors
Acknowledgements: We express our sincere gratitude to Mr. Amir Raza for analyzing the data and to Ms. Asma Hasnain for proof reading the scientific content
Authors’ contribution:
MIAK & ASS: Conduct of study, literature search, statistical analysis or manuscript editing
FK: Concept of research question
REFERENCES
- Singh V, Gupta P, Khatana S, Bhagol A. Supplemental oxygen therapy: Important considerations in oral and maxillofacial surgery. Natl J Maxillofac Surg. 2011;2:10-14. doi: 10.4103/0975-5950.85846. [PubMed] [Free full text]
- Apfelbaum JL, Silverstein JH, Chung FF, Connis RT, Fillmore RB, Hunt SE, et al. Practice guidelines for postanesthetic care: an updated report by the American Society of Anesthesiologists Task Force on Postanesthetic Care. Anesthesiology. 2013;118:291-307. doi: 10.1097/ALN.0b013e31827773e9.
- Gift AG, Stanik J, Karpenick J, Whitmore K, Bolgiano CS. Oxygen saturation in postoperative patients at low risk for hypoxemia: is oxygen therapy needed? Anesth Analg. 1995;80:368-372. [PubMed]
- Moller JT, Johannessen NW, Espersen K, Ravlo O, Pedersen BD, Jensen PF, et al. Randomized evaluation of pulse oximetry in 20,802 patients: II. Perioperative events and postoperative complications. Anesthesiology. 1993;78:445-453. [PubMed]
- Bitterman H. Bench-to-bedside review: oxygen as a drug. Crit Care. 2009;13:205. doi: 10.1186/cc7151. [PubMed] [Free full text]
- Rose DK, Cohen MM, Wigglesworth DF, DeBoer DP. Critical respiratory events in the postanesthesia care unit. Patient, surgical, and anesthetic factors. Anesthesiology. 1994;81:410-418. [PubMed]
- DiBenedetto RJ, Graves SA, Gravenstein N, Konicek C. Pulse oximetry monitoring can change routine oxygen supplementation practices in the postanesthesia care unit. Anesth Analg. 1994;78:365-368. [PubMed]
- Rothen HU, Sporre B, Engberg G, Wegenius G, Hedenstierna G. Airway closure, atelectasis and gas exchange during general anesthesia. Br J Anaesth. 1998;81:681-686. [PubMed]
- Powell JF, Menon DK, Jones JG. The effects of hypoxaemia and recommendations for postoperative oxygen therapy. Anaesthesia. 1996;51:769-772. [PubMed]
- Merchant R, Bosenberg C, Brown K, Chartrand D, Dain S, Dobson J, et al. Guidelines to the practice of anesthesia revised edition 2010. Can J Anaesth. 2010;57:58-87. doi: 10.1007/s12630-009-9209-4. [PubMed] [Free full text]
- Eichhorn JH, Cooper JB, Cullen DJ, Maier WR, Philip JH, Seeman RG. Standards for patient monitoring during anesthesia at Harvard Medical School. JAMA. 1986;256:1017-1020. [PubMed]
- Vegfors M, Cederholm I, Lennmarken C, Löfström JB. Should oxygen be administered after laparoscopy in healthy patients? Acta Anaesthesiol Scand. 1988;32:350-352. [PubMed]
- Smith DC, Canning JJ, Crul JF. Pulse oximetry in the recovery room. Anaesthesia. 1989;44:345-348. [PubMed]
- Murray RS, Raemer DB, Morris RW. Supplemental oxygen after ambulatory surgical procedures. Anesth Analg. 1988;67:967-970. [PubMed]
- Russell GB, Graybeal JM. Hypoxemic episodes of patients in a postanesthesia care unit. Chest. 1993;104:899-903. [PubMed]
- Filho GRO, Gracia JHS, Ghellar MR, Nicolodi MA, Boso AL, Dal Mago AJ. Factors Associated to Hypoxemia in the Immediate Postoperative Period. Rev Bras Anestesiol. 2001;51:185-195. doi: 10.1590/S0034-70942001000300001. [Free full text]
- Hedenstierna G, Lofstrom J. Effect of anesthesia on respiratory function after major lower extremity surgery. A comparison between bupivacaine spinal analgesia with low-dosemorphine and general anesthesia. Acta Anaesthesiol Scand. 1985;29:55-60. [PubMed]
- George JM, Nair L, Dhara SS. Postoperative hypoxaemia during transport and in the recovery area. Ann Acad Med Singapore. 1995;24:807-811. [PubMed]
- Rheineck-Leyssius AT, Kalkman CJ, Trouwborst A. Influence of motivation of care providers on the incidence of postoperative hypoxaemia in the recovery room. Br J Anaesth. 1996;77:453-457. [PubMed]
- Qaseem A, Snow V, Fitterman N, Hornbake ER, Lawrence VA, Smetana GW, et al. Risk assessment for and strategies to reduce perioperative pulmonary complications for patients undergoing noncardiothoracic surgery: a guideline from the American College of Physicians. Ann Intern Med. 2006;144:575-580. [PubMed]
- World alliance for patient safety. WHO guidelines for safe surgery. Geneva: WHO 2008. [Full free text]
- Osinaike BB, Amanor-Boadu SD. Routine oxygen administration in the pacu: should everybody have it? SAJAA. 2006;12:72. [Full free text]
- Fu ES, Downs JB, Schweiger JW, Miguel RV, Smith RA. Supplemental oxygen impairs detection of hypoventilation by pulse oximetry. Chest. 2004;126:1552-1558. doi: 10.1378/chest.126.5.1552. [PubMed]
- Sato C, Tanaka H, Kawamoto M, Yuge O, Ogawa R. Low oxygen saturation during early postoperative period in adult patients receiving opioids by intravenous patient-controlled analgesia. Masui. 2004;53: 659-663. [PubMed]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube