
Fazal Wahab Khan, Yasir Bilal Khan, Mahnur Khan, Mohsin Abbas, Saulat H. Fatimi
Department of Cardiothoracic Surgery, Aga Khan University Hospital, Karachi, (Pakistan)
Correspondence: Fazal Wahab Khan, Associate Professor, Department of Cardiothoracic Surgery, Aga Khan University, Stadium Road, Box 3500, Karachi 74800, (Pakistan)
ABSTRACT
A 58 years old man with a history of ischemic heart disease presented with massive hemoptysis. On evaluation with CT chest, he was found to have a large aspergilloma in the left upper lobe. Coronary angiogram was also performed for increasing episodes of angina which showed critical 100% ostial left anterior descending (LAD) stenosis. In view of aspergilloma and hemoptysis, patient could not have conventional open heart surgery and heparinization. Therefore, coronary artery bypass grafting (CABG) was performed on beating heart and this was followed by left upper lobectomy at the same time. Patient had an uneventful post-operative course.
Key words: Aspergilloma; Coronary artery disease; Cardiac surgery; Off-pump Coronary Artery Bypass Grafting; Lobectomy
Citation: Khan FW, Khan YB, Khan M, Abbas M, Fatimi SH. Simultaneous off-pump coronary artery bypass grafting (CABG) and right upper lobectomy for critical left anterior descending artery (LAD) stenosis and aspergilloma. Anaesth Pain & Intensive Care. 2016;20 Suppl 1:S158S160
Received: 19 August 2016; Reviewed: 29 August 2016; Accepted: 10 September 2016
INTRODUCTION
Aspergilloma is the best-recognized and most common form of pulmonary involvement due to Aspergillus. It usually develops into a preformed lung cavity with pulmonary cavities secondary to Tuberculosis being the most frequently associated condition.1 Severe hemoptysis may also occur, leading to complications.2 Aspergilloma of the lung concomitant with severe ischemic heart disease is uncommon. Instead of treating the patient with two surgeries [a lung resection followed (or preceded) by coronary artery bypass grafting (CABG)] a combined procedure could improve the short and long-term outcome. If CABG is performed off-pump, the pulmonary complications of cardiopulmonary bypass (CPB) and its immunosuppressant effects in a lung resection setting can be avoided.3
CASE REPORT
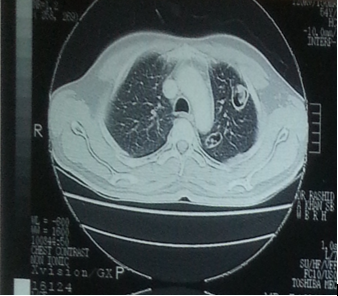
A 58 yrs old man was admitted to our hospital with complaints of hemoptysis and cough. He had co-morbid diseases, e.g., diabetes mellitus type 2 and treated pulmonary tuberculosis. The patient reported that he was diagnosed with pulmonary tuberculosis a year ago and received anti-tuberculous treatment for 9 months. However, the cough and hemoptysis did not subside. He also complained of chest pain that occurred on and off since the last month and the pain radiated to the left arm and lower jaw. Evaluation with chest x-ray and computed tomographic (CT) scan revealed few small cavitatory lesions in his left upper lobe. One of the cavities in the anterior segment measured 2.3×1.9 cm and was associated with adjacent atelectasis and pneumonic changes. There was also a focal varicoid type bronchiectasis; and granulomas were noted in the adjacent lung parenchyma. There was no evidence of pneumothorax or interstitial disease on the CT scan of chest.
The patient also had an episode of acute chest pain a month before his admission in our hospital. At that time, he got his investigations for acute myocardial infarction (MI) done at another hospital. His troponin T levels, done at that time, were 160ng/l suggesting myocardial damage. The echocardiogram revealed moderately reduced left ventricular systolic function with an ejection fraction of 40%. Mid to distal anterior wall, mid to distal septum and apical segments of the heart were severely hypokinetic on the echocardiogram. It also showed grade 1 left ventricular diastolic dysfunction with mild mitral regurgitation. On the basis of these reports, we performed cardiac catheterization on the patient and an angiogram revealed a 100% ostial stenosis in the left anterior descending (LAD) artery with retrograde filling and a 50% stenosis of the first obtuse marginal branch (OM1) of left circumflex artery (LCX). The left main (LMA) and right coronary artery (RCA) were normal. On the basis of these findings, a pre-operative diagnosis of double vessel coronary artery disease and left upper lobe cavitatory lesion with aspergilloma (fungus ball) was made.
The patient was taken to the operating room for a simultaneous off-pump coronary artery bypass graft (OPCABG) surgery and left upper lung lobe resection. Following general anesthesia, intubation was performed with a double lumen endotracheal tube. The patient was placed in the supine position. Midline sternotomy was performed and skeletonized left internal mammary artery (LIMA) was harvested. Anticoagulation with 7500 units/kg of heparin was achieved. Octopus suction stabilizer (Medtronic) was used to stabilize the heart. The LIMA graft was anastomosed to the LAD artery with continuous 7.0 polypropylene sutures. To protect the grafted LIMA, a left sided posterolateral thoracotomy was performed for left upper lobectomy. The right lung was ventilated and the left lung was collapsed. The lung parenchyma was retracted with conventional lung forceps. The interlobar arteries were identified and dissected. Silk sutures 3.0 were used to encircle and ligate the vessels. When the left upper lobe was completely freed, it was retrieved and the remaining lung was expanded to verify that the bronchial seal was adequate. Three chest tubes (32-French) were placed; one in the mediastinum and two in the left pleural cavity. The incision closure was done in continuous layers, postoperatively, the remaining lung expanded without any evidence of air leaks and the patient underwent an uneventful post-operative recovery. He was discharged from the hospital on the 5th postoperative day.
Histopathology of the specimen of lung tissue revealed chronic granulomatous inflammation with fungal ball suggestive of aspergilloma, accompanied by anthracosis. There was no evidence of malignancy.
Figure: CT scan showing an aspergilloma in the upper lobe of left lung
DISCUSSION
Patients with aspergilloma in the lung and a coexisting coronary artery disease that is amenable to surgery are excellent candidates for the type of procedure described here. Usually, the surgical procedures are staged (a lung resection followed or preceded by CABG) because they are considered more feasible and safe. However, this approach also has several drawbacks such as the discomfort of two operations, increased cost and long duration of hospital stay. The blood loss from the site of lesion within the lung and impaired ventilation and perfusion of the lung between the interval of two operations in staged procedures can make the prognosis worse.4,5 On the other hand, in a case when active hemoptysis is present, the morbidity and mortality risks of performing an Off-pump CABG are significantly increased. With on-pump CABG, a suppression of immune system is known to occur with extracorporeal circulation and this can progress toward the dissemination of the disease. The on-pump CABG also carries the risk of intrapulmonary hemorrhage, which in this setting can be life-threatening. In contrast, the off-pump CABG avoids the physiological stress associated with cardiopulmonary bypass (less pulmonary dysfunction and decreased incidence of post-operative renal failure) and aortic cannulation that can lead to cerebrovascular injury due to atherosclerotic embolization. Off-pump CABG reduces the post-operative bleeding, transfusion requirements and/or ICU stay.6,7,8
CONCLUSION
Combined heart surgery and lung lobe resection can be performed without increased mortality and/or morbidity. This synchronous treatment avoids the necessity of another intervention in cooperation with being economically beneficial for the patient and reducing the duration of hospital stay. Avoidance of cardiopulmonary bypass in this case may decrease the incidence of post-operative complications by decreasing blood loss and ventilation requirements.
Competing Interests: The authors have declared that no competing interests exist.
Authors’ Contribution: All authors took equal part in conduction of the case and writing this manuscript including literature search and editing
REFERENCES
- Kawamura S, Maesaki S, Tomono K, Tashiro T, Kohno S. Clinical evaluation of 61 patients with pulmonary aspergilloma. Intern med. 2000;39(3):209-12. [PubMed] [Free full text] doi:10.2169/internalmedicine.39.209
- Soubani AO, Chandrasekar PH. The clinical spectrum of pulmonary aspergillosis. Chest Journal. 2002;121(6):1988-99. [PubMed] doi:10.1378/chest.121.6.1988
- Zhang Y, Wu Y, Yuan B, Liu X, Zhao S, Li Z, et al. Coronary artery bypass grafting with concomitant resection for carcinoma of lung. J Biomed Res. 2010;24(1):77-80. [PubMed] [Free full text] doi:10.1016/S1674-8301(10)60013-9
- Morishita K, Kawaharada N, Watanabe T, Koshima R, Fujisawa Y, Watanabe A, et al. Simultaneous cardiac operations with pulmonary resection for lung carcinoma. Jpn J Thorac Cardiovasc Surg. 2001;49(12):685-9. [PubMed] doi:10.1007/BF02913505
- Prokakis C, Koletsis E, Apostolakis E, Panagopoulos N, Charoulis N, Velissaris D, et al. Combined heart surgery and lung tumor resection. Med Sci Monit. 2008;14(3):CS17-CS21. [PubMed] [Free Full Text]
- Hernandez F, Cohn WE, Baribeau YR, Tryzelaar JF, Charlesworth DC, Clough RA, et al. In-hospital outcomes of off-pump versus on-pump coronary artery bypass procedures: a multicenter experience. Ann Thorac Surg. 2001;72(5):1528-34. [PubMed] [Free full text] doi:10.1016/S0003-4975(01)03202-7
- Cleveland JC, Shroyer ALW, Chen AY, Peterson E, Grover FL. Off-pump coronary artery bypass grafting decreases risk-adjusted mortality and morbidity. Ann Thorac Surg. 2001;72(4):1282-9. [PubMed] doi:10.1016/S0003-4975(01)03006-5
- Prokakis C, Koletsis E, Apostolakis E, Panagopoulos N, Charoulis N, Velissaris D, et al. Combined heart surgery and lung tumor resection. Med Sci Monit . 2008;14(3):CS17-CS21. [PubMed] [Free Full Text]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube