
Muhammad Fuad Bangash, MD, FCCP
Medical Director ICU, SSM Health, Greater Fond Du Lac Region, Fond Du Lac, WI, (USA)
Correspondence: Dr Muhammad Fuad Bangash, MD, FCCP,
Medical Director ICU, SSM Health, Greater Fond Du Lac Region, Fond Du Lac, WI, (USA);
E-mail: fuadmb@yahoo.com
ABSTRACT
Sepsis remains a major source of morbidity and mortality not only in the United States but worldwide. The key to save lives of these patients is to have a multi-pronged approach to the management of sepsis. In this review article we shall go through the specifics of this approach. Sepsis is a life-threatening organ dysfunction caused by dysregulated host response to infection. The septic shock is a subset of sepsis with circulatory and cellular/metabolic dysfunction. Patients with sepsis (formerly severe sepsis) should still be identified by the same organ dysfunction criteria (including lactate level > 2 mmol/L). Organ dysfunction may also be identified using the ‘quick Sepsis-Related Organ Failure Assessment’ (qSOFA). Appropriate source control and immediate treatment with IV antibiotics is a cornerstone of sepsis management. The next step is to resuscitate patients with sepsis-induced hypoperfusion with at least 30 ml/kg of intravenous crystalloid fluid. If the patient is hypotensive despite adequate fluid resuscitation, then use of vasoactive agents like norepinephrine and vasopressin is indicated.
Keywords: Sepsis; quick Sepsis-Related Organ Failure Assessment; Mortality
Citation: Bangash MF. Sepsis: an update in 2018. Anaesth Pain & Intensive Care 2018;22 Suppl 1:S99-S101
Received: 8 Sep 2018, Reviewed: 16 Sep 2018, Accepted: 15 Oct 2018
Despite all the advances in medical science, the morbidity and mortality due to Sepsis remains high1 resulting in more than 2.4 million deaths during 1999-2014. The key to save lives of these patients is to have a multi-pronged approach right from increasing the understanding of the disease definition and diagnosis to efficient management of Sepsis. In this review article I will go through the specifics of this approach and after reading this thoroughly you should be able to go to your specific health-care setting and help save lives!
Sepsis is a life-threatening organ dysfunction caused by dysregulated host response to infection and septic shock is a subset of sepsis with circulatory and cellular/metabolic
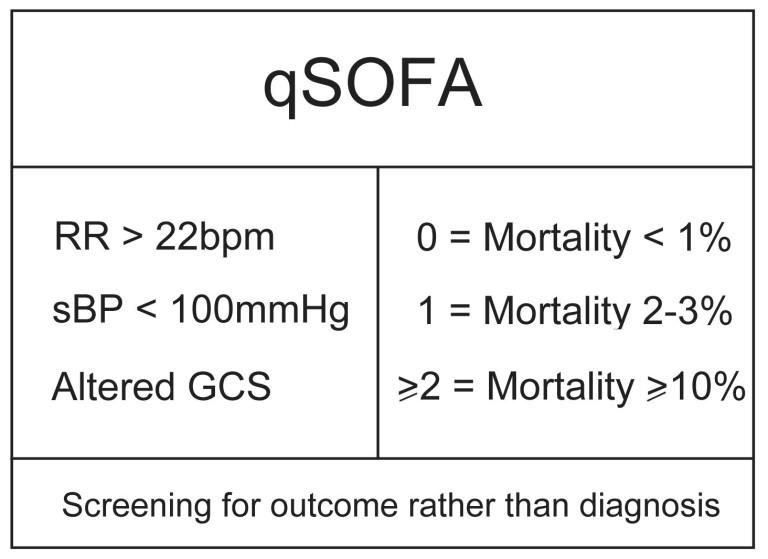
Table 1: qSOFA and its association with mortality
dysfunction associated with higher risk of mortality.2
Patients with sepsis (formerly severe sepsis) should still be identified by the same organ dysfunction criteria (including lactate level greater than 2 mmol/L). Organ dysfunction may also be identified using the ‘quick Sepsis-related Organ Failure Assessment’ (qSOFA) as seen in the Table 1 above.
Despite attempts to increase the recognition and the potential for deadly outcomes especially by Society of Critical Care Medicine, some basic mistakes may be seen in the diagnosis and management of Sepsis in many healthcare settings even during 2018. Many a times, unlike acute ST elevation MI or acute stroke or trauma, patients with sepsis do not receive the same attention. Time is of the essence and each minute lost can exponentially increase the risk of adverse outcome in these patients.
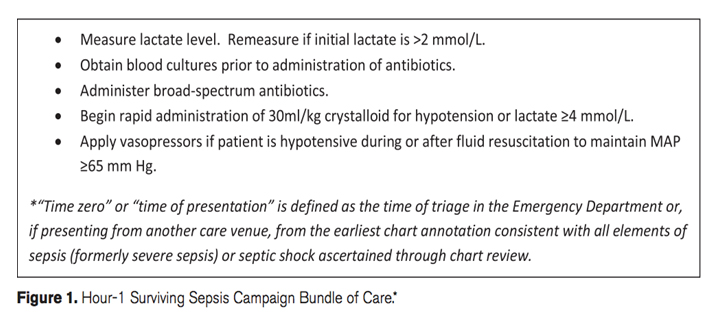
Sepsis and septic shock are medical emergencies and it is recommended that treatment and resuscitation begin immediately.2 For example, if you have a patient who is febrile, has tachycardia and cellulitis of the left leg, he deserves immediate attention with obtaining wound and blood cultures, source control with intervention if needed and IV antibiotics based on the antibiogram of your institution. We all know this but where the rubber meets the road is that to make sure the patient actually gets these interventions right away as simply ordering on paper or EHR (electronic health records) is not enough. Just like a golden hour in trauma, there is a golden hour in sepsis. Every minute counts and if you perform the required interventions in a timely fashion, a marked improvement in your patient’s condition will be witnessed and outcomes will improve in your institution. You have to see the lab technician in the room obtaining cultures, you have to see nurse obtaining and monitoring vital signs frequently and you have to see the right antibiotic by the patient’s bedside being infused into a patent IV. Antibiotics for patients with sepsis are like thrombolytics in a patient with acute coronary block or a patient with stroke. In a retrospective analysis of patients with sepsis admitted to intensive care units (ICUs) from 1989 to 2004, Kumar and colleagues found an average 7.6% decrease in survival with every hour delay in receiving antibiotics after the onset of hypotension.3 Appropriate broad spectrum antibiotics are important because there is going to be no benefit to your patient with sepsis if the bacteria causing the infection are not covered by or susceptible to antibiotics you have prescribed. The author cannot help but recall a patient with Legionella pneumonia who was receiving IV ceftriaxone only for more than 24 hours after admission with fever and headache. How to avoid such grave mistakes? Be vigilant for signs and symptoms of various infections especially in patients with specific risk factors including but not limited to those who are immunocompromised.
The next step is to resuscitate patients with sepsis-Induced hypoperfusion with at least 30 ml/kg of intravenous crystalloid fluid.2 This is best done in the emergency room with close coordination between the ER team and ICU team. If the time that the patient is triaged in ED is time zero, then all of these interventions are best performed as soon as possible preferably within 60 minutes. Assessment of fluid resuscitation can be based on physical examination with signs like leg raise test, capillary refill, hemodynamics and urine output. CVP monitoring which used to be recommended by earlier guidelines is no longer recommended as routine.
IV access can become an issue in these patients and should be manage appropriately with either large bore peripheral IV cannulas or central line insertion if needed. Central line insertion can be achieved quickly in 2018 especially with use of ultrasound guidance.
If the patient is hypotensive despite adequate fluid resuscitation, then use of vasoactive agents like norepinephrine and vasopressin is indicated. Due to potential complications, these agents are best administered through a central line. These agents are titrated to keep MAP > 65 mmHg. After a long time, a new pharmacologic treatment has been added to the Intensivist or anesthesiologist armamentarium in the shape of angiotensin-II.
FDA has approved angiotensin-II infusion for management of patients with vasodilatory shock. Due caution should be exercised as with any new pharmacologic agent and further specific outcome data in septic shock is awaited before recommendation of using angiotensin-II
Patients with sepsis and septic shock should be monitored in units that can provide specialized care which these patients need. This can vary based on resources available and the healthcare setting but well-staffed ICUs with trained and experienced nursing staff, 24/7 Intensivists provide these patients and their families the best possible outcomes. Hand hygiene, DVT prophylaxis and other standard ICU measures can make a big difference in these patients in ensuring good outcomes and preventing complications like C diff colitis and venous thromboembolism.
There is a lot that can be done for patients with sepsis and septic shock based on the current state of our knowledge in 2018. Future directions and areas of research will include but not limited to role of genetics in patient immune response to various infections, earlier identification of specific bacteria in blood stream, newer antibiotics with novel mechanisms of actions and therapeutic interventions targeting these immune responses.
Conflict of interest: None declared by the author
REFERENCES
- Galeski DF, Edwards JM, Kallan MJ, Carr BG. Benchmarking the incidence and mortality of severe sepsis in the United States. Crit Care Med 2013;41:1167-74 [PubMed] [Free full text]
- Surviving Sepsis Campaign: International Guidelines for Management of Sepsis and Septic Shock: 2016 survivingsepsis.org
- Kumar A, Roberts D, Wood KE, et al. Duration of hypotension before initiation of effective antimicrobial therapy is the critical determinant of survival in human septic shock. Crit Care Med 2006;34(6):1589-1596. [PubMed] [Free full text]
- Rhodes A. Evans, Alhazzani W, et al. Surviving Sepsis Campaign: International guidelines for management of Sepsis and Septic Shock: Critical Care Med 2017;43:304-377 [PubMed] [Free full text]
- Hashmi M, Khan FH, Zubairi ABS, Sultan ST, Haider S, Aftab S, et al. Developing local guidelines for management of sepsis in adults: Sepsis Guidelines for Pakistan (SGP). Anaesth Pain & Intensive Care 2015;19(2):196-208 [Free full text]
- Reinhart K, Kissoon N. Sepsis Guidelines for Pakistan. Anaesth Pain & intensive Care 2015;19(2):105-7 [Free full text]
- Khanna A, English SW, Wang XS, et al. Angiotensin II for the treatment of vasodilatory shock. N Engl J Med2017;377:419-430 [PubMed] [Free full text]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube