
Arvind Sivasundar*, Surajit Giri**, Shiv Kumar Singh***
*Consultant Anesthesiology, Seethapathy Clinic and Hospital, Chennai, Tamilnadu, (India)
**Consultant Anesthesiology, Sivasagar, Assam, (India)
*** Consultant, Department of Anesthesiology, Royal Liverpool University Hospitals, Liverpool L7 8XP (UK)
Correspondence: Dr Shiv Kumar Singh, Consultant Anesthesiologist, Department of Anesthesiology, 11th Floor, Royal Liverpool University Hospitals, Prescot Street, Liverpool L7 8XP (UK); Email: Shvkmrsngh@aol.com
ABSTRACT
Anesthesia in an obstetric emergency presents an additional risk to the mother, and may potentially have harmful effects on the fetus. Maternal risks can be significantly reduced by using regional anesthesia, whenever possible and general anesthesia be resorted to only when absolutely required. This is especially relevant in the developing countries where deaths under anesthesia may be significantly higher than in the ‘west’.
While CS done because of maternal hemorrhage or umbilical cord prolapse usually mandate general anesthesia, CS done because of a non-reassuring fetal status often permits the administration of a regional anesthesia. Close communication with the obstetrician helps determine whether the fetus, mother, or both are in immediate jeopardy requiring GA, or there is time to safely administer RA.
There are situations where both neuraxial blocks and general anesthesia may both be contraindicated. In these situations, the use of regional anesthesia techniques such as transversus abdominis plane (TAP) block can be useful, providing not only anesthesia, but also postoperative pain relief.
The loss of resistance technique for TAP blocks is a simple and reliable technique which can be done without the need for ultrasound guidance. An understanding of the ‘cushion effect’ significantly improves the success rate of this technique.
Key words: Cesarean section; Neuraxial blocks; Transversus abdominis plane block;
Citation:Sivasundar A, Giri S, Singh SK. Role of regional anesthesia in obstetric emergencies. Anaesth Pain & Intensive Care 2015;19(1):71-79
INTRODUCTION
No specialty of medicine is more inundated with emergencies than obstetrics. Obstetric emergencies carry a unique challenge for the attending anesthesiologist in terms of provision of anesthesia and perioperative analgesia. Anesthetic care provided to a parturient is, in a sense, the culmination of all the principles of obstetric anesthesia. While the safety of the mother is paramount, fetal wellbeing cannot be compromised. In the recent past, maternal mortality due to anesthesia has declined, as indeed has maternal mortality due to other causes. [1,2] In the west it has been estimated that anesthesia is responsible for 6-7 % of maternal deaths. [1] The figures for the Asian countries is difficult to gather as there is no robust data. The majority of these deaths occur during general anesthesia and can be attributed to failed ventilation and oxygenation and / or failed intubation as well as secondary to pulmonary aspiration of gastric contents. [1,2] Associated factors include obesity and emergency procedures. Many recommend that regional anesthesia (RA) is preferred and general anesthesia (GA) be resorted to only when absolutely required. In the west as per the recent literature, the number of death directly due to anesthesia is relatively small and those that are reported are multifactorial and difficult to classify/ categorise as “anesthetic death”. [1] This trend may not be true for the developing world where the deaths under anesthesia may still be very high. [2]
ANESTHESIA FOR EMERGENCY CESAREAN SECTION
Regarding the choice of anesthetic technique for a cesarean section (CS), the factors that need to be considered are the indication for the surgery, the urgency of the procedure, the health status of the mother and fetus, and the presence of a pre-existing functioning epidural catheter. Regional techniques are appropriate in most elective cesareans and in many urgent cesareans. In emergency CS, however, it may be difficult to choose either GA or RA. Traditionally, an urgent surgery is for a condition that is potentially life threatening and requires surgery within 24 hours while an emergent surgery is required for a condition which is immediately life-threatening, mandating immediate surgery within hours. In obstetrics this is further complicated because we are dealing with two (sometimes more) lives. Extra caution with respect to one may jeopardise the well being of the other. For example, in a CS for a full stomach mother with a non-reassuring cardiotocograph (CTG), the choice of GA may produce better fetal outcome, while putting the mother at a high risk of aspiration. If, on the other hand, RA is chosen, the risk of maternal aspiration is reduced, but the fetal outcomes may not be as good.
OBSTETRIC EMERGENCIES
Obstetric emergencies may be broadly classified based upon maternal and fetal concerns. Emergencies due to maternal concerns include hemorrhage (placenta praevia, placenta accreta, abruption and uterine rupture) and deteriorating maternal medical illness. Severe maternal hemorrhage typically dictates the administration of GA while the choice of anesthetic technique for patients with a medical illness depends on the nature of the illness and the maternal condition. Emergencies due to fetal concerns include severe fetal distress and umbilical cord prolapse. Cord prolapse usually require a GA whereas the choice of anesthesia is more difficult in cases of fetal stress and distress. Obstetricians are often concerned about the anesthesiologist’s ability to perform RA with speed to perform a timely delivery, or that RA may cause hypotension and compromise utero-placental perfusion of an already hypoxic fetus. Clinical studies, however, show that the administration of RA does not result in an increased risk to the fetus, even in cases of modest fetal distress. [3,4]
FETAL DISTRESS AND REGIONAL ANESTHESIA
Fetal distress is a widely used but poorly defined, imprecise, vague, nonspecific term and has a limited positive predictive value. It is often associated with delivery of an infant who is in perfect condition at birth. The American College of Obstetricians and Gynecologists (ACOG) has suggested that this term be replaced with ‘non reassuring fetal status’. Whereas fetal distress implies an ill fetus, non-reassuring fetal status describes the clinician’s interpretation of data regarding the fetal status. [5] Notwithstanding this, many obstetricians continue to use the term fetal distress to describe a whole range of CTG abnormalities. In some cases, the global use of this term has resulted in unnecessarily urgent delivery under general anesthesia, when in fact; the particular CTG abnormality may have permitted administration of a regional anesthesia. Maternal mortality in Asian countries is 14 times higher than the developed countries, 140 per 100,000 live births, At the country level, India (50,000/year) and Nigeria (40,000/year) account for one third of all global maternal death (289,000/ year in 2013). [2] It is probably still true that, all things considered RA is a safer alternative to GA in a pregnant patient. Other advantages of RA include less neonatal exposure to potentially depressant drugs, decreased risk of pulmonary aspiration and an awake mother during the birth of her child. Blood loss is also, usually low in cases done under RA compared to GA. Royal College of Anesthesiologists suggests that more than 50% of category-1 CS should be done under RA. The percentage should be more than 85% for category 2-3 and 95% for category-4. [6]
Of course, the experience of the practitioner does affect the speed with which the neuraxial block is administered, an experienced anesthesiologist administering SA as quickly as GA. Close communication with the obstetrician is necessary to determine whether the fetus, mother, or both are in immediate jeopardy requiring GA, or there is time to safely administer RA.
Before administering SA to a patient who requires urgent CS, it is important to ensure that severe hypotension does not occur. The possibility that fetal distress may be secondary to an abruption with unrecognised hypovolaemia should also be kept in mind. Since time is of the essence, a relatively larger sized needle may be used (23 to 25 G). Finally, it is important to be prepared to use an alternative technique if one encounters an unexpected technical difficulty. Clear communication between the anesthesiologist and the obstetrician is important. The obstetrician must indicate the severity of fetal heart rate abnormality. Likewise, the anesthesiologist must voice his/her concerns, if any. For example, the obstetrician may be more amenable to agreeing to a regional technique if the anesthesiologist suspects that the intubation may be a difficult one.
EARLY INSERTION OF SPINAL OR EPIDURAL CATHETERS
The ASA task force on obstetric anesthesia suggests that early insertion of a spinal or epidural catheter for obstetric (e.g., twin gestation or pre-eclampsia) or anesthetic indications (e.g., anticipated difficult airway or obesity) should be considered to reduce the need for GA if an emergent procedure becomes necessary. In these cases, insertion of a spinal or epidural catheter may precede the onset of labor or a patient’s request for labor analgesia. [7]
PRE-ECLAMPSIA, ECLAMPSIA AND NEURAXIAL ANESTHESIA
The cure for severe pre-eclampsia and eclampsia is delivery of the fetus. A vaginal delivery is hoped for and CS is indicated in case of failed induction, malposition or worsening blood pressure. The role of neuraxial anesthesia in these conditions is becoming clearer now with the better understanding of maternal and fetal outcomes. In the presence of existing epidural catheters and need for emergency CS, epidural can be topped up with higher concentration of LA with/without opioids. Role of spinal anesthesia (SA) in pre-eclamptics requiring emergency surgery is better understood now. SA is simple to perform, provides rapid onset and a dense block. Addition of opioids not only improves the quality of the block but also provides excellent post-operative analgesia. It has been now proven beyond doubts that as long as systolic blood pressure is maintained greater than 80% or more of the baseline, no effect on Apgar scores and umbilical artery pH is observed. Contrary to common belief it has been observed that the incidence of spinal induced hypotension and the vasopressor requirement is much lower in preeclamptic parturients when compared with normal parturients undergoing CS delivery. [8,9] It is advocated that liberal IV fluids for pre-loading or co-loading should be avoided in these cases. A recent retrospective review comparing two tertiary referral obstetric units has shown that preeclamptic parturients with liberal fluid administration had a higher incidence of acute pulmonary edema over parturients with restricted fluid administration during the perioperative period. [10]
Unlike severe pre-eclamptic patients, patients with PIH and HELLP syndrome pose a significant anesthetic challenge. Coagulopathy in these parturients is usually due to low platelet count and, less commonly, disseminated intravascular coagulation. The presence of coagulopathy precludes the provision of RA for CS delivery. Studies investigating coagulation in these parturients using thromboelastography observed that coagulopathies with the platelet count greater than 100,000/mm3 was rare. With platelet count less than 100,000/mm3 or on the decline, prompt coagulation evaluation is recommended. [11]
HEMORRHAGIC EMERGENCIES IN OBSTETRIC
As far as hemorrhagic emergencies in obstetrics are concerned, there is no doubt that GA is preferred and it is the availability of resources that reduces maternal complications; large-bore intravenous catheters, fluid warmer, forced-air body warmer, availability of blood bank resources, equipment for infusing intravenous fluids and blood products rapidly (examples include, but are not limited to, hand- squeezed fluid chambers, hand-inflated pressure bags, and automatic infusion devices) (Figures 1-A, 1-B & 1-C). [7]
Figure 1-A: Hand-inflated pressure bag for 1000 ml infusion bottle

Figure 1-B: Hand-inflated pressure infuser for blood bags

Figure 1-C: Automatic programmable infusion pump

REGIONAL ANESTHESIA TECHNIQUES OTHER THAN NEURAXIAL BLOCKS
Looking into the literature, we find mention of CS under local infiltration and even without any anesthesia in dire emergencies or when anesthesiologist is not available.[12] In the modern era this would be considered as unethical or even barbaric. There are situations where neuraxial blocks and GA, both may be contraindicated or may be considered unsafe. In these situations, knowledge and use of regional anesthesia techniques like “loss of resistance” (LOR) blocks or PNS/ US Guided blocks can be very useful. These blocks not only provide anesthesia but also post-operative pain relief in the parturient, thus avoiding the use of opioids and their associated side effects. As part of multimodal analgesia, these blocks not only improve patient satisfaction but also allow for increased bonding between mother and child.[13]
SURGICAL INCISION AND THE BLOCKS
As we are all aware, in most of the obstetric emergencies, approach to the abdomen involves incision that lies in the infraumbilical region, which is supplied by T10- L1 dermatomes. These segments can be blocked by transversus abdominis plane (TAP) block or in case of transverse or pfannensteil incision, selective ilioinguinal and iliohypogastric nerves (IIN and IHN) can be blocked for surgery and analgesia. Any incision extending above the umbilicus would require posterior rectus sheath block. In this section we describe these blocks and their use in obstetrics. [14]
TRANSVERSUS ABDOMINIS PLANE (TAP) BLOCK
LA deposited under the Internal Oblique fascia and above the transversus abdominis (TA) muscle, the transversus abdominis plane (TAP), consistently blocks the peripheral nerves originating from T6 – L1 that supply the anterior abdominal wall[15] (Figure 2).
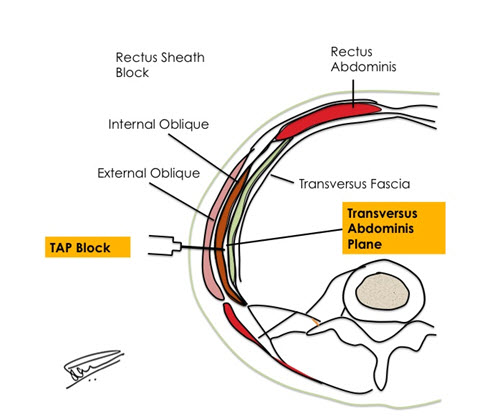
Figure 2: Transversus Abdominis (TA) Plane and TAP Block
There are numerous studies demonstrating different levels of spread of LA, anywhere from L1 to T6 and then there are some cadaveric studies that have demonstrated LA ascending even up to T10 level. [16] In our experience we have found that 20ml of LA in TA plane consistently blocks segments from T10 to L1. In 2001 Rafi et al described TAP block in the Triangle of Petit (TOP) using double “pop” (loss of resistance technique), the first one from External Oblique (EO) fascia and second one from the Internal Oblique (IO) fascia. [17] Subsequent studies have shown that it is not easy to palpate and locate the TOP, especially in the obese and, particularly in parturients with increased fatty tissue and lax skin in the flanks. [18]
The analgesic efficacy of the TAP block has been demonstrated in different surgical settings in prospective randomized trials as compared to placebo. The efficacy has been demonstrated in abdominal surgery [19], hysterectomy [20], retropubic prostatectomy [21], CS [22], laparoscopic cholecystectomy [23] and appendectomy [24]. All these studies have reported superiority of the TAP block in reducing pain and morphine consumption as demonstrated by reduction in visual analogue scale (VAS) scores.
In a meta-analysis on TAP blocks for postoperative analgesia in obstetric emergencies, it was found that they were more effective in patients who did not receive intra-thecal opioids as compared to those who did. [25] In the recent years, there has been resurgence of ultrasound guided TAP blocks. Leave alone the developing world, even in the developed countries many do not have access and/ skills to use this technique. Due to its simplicity, loss of resistance (LOR) TAP block still remains an attractive option for those who are devoid of this luxury.
LOSS OF RESISTANCE TAP BLOCK
For a successful LOR TAP Block, there are three pre-requisites:
- Short beveled or blunt tipped needle, for appreciation of “bounce” and “pop” over the fascia.
- Understanding of the “cushion effect”, and
- Understanding techniques for eliminating the “cushion effect”.
For effective TAP blocks, one has to thoroughly understand the concept of the “cushion effect”, first described by one of the authors (Singh SK).[26] We have found that “cushion effect” is the most consistent cause for failure of LOR blocks. For an effective and successful TAP block and for appreciation of LOR from EO and IO fascia, anesthesiologist must eliminate the “cushion effect”.
WHAT IS CUSHION EFFECT?
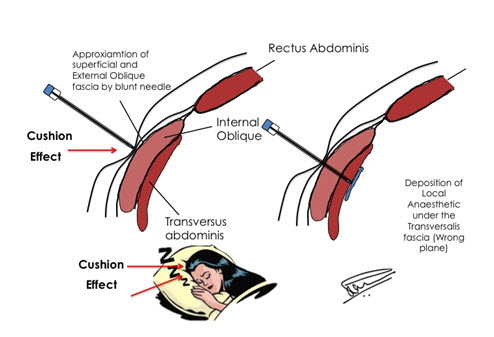
Blunt tip needles help in appreciation of “bounce” and “pop” over the fascial layers. They give an excellent feedback to the anesthesiologist of the loss of resistance but, as the needle tip is blunt, it requires considerable amount of force to negotiate the skin. The subcutaneous tissue below the skin acts as a “cushion” and the applied force squashes the skin, subcutaneous tissue and external oblique muscle itself. Because of the force and resistance of tissues, the blunt needle not only breaks through the skin barrier but also pierces the other tissues including the EO fascia. The subsequent search for “two pops” may lead to either deposition of LA in the deeper planes or even puncture of the viscera in very thin and lean patients. These risks are higher with needles that are thicker and very blunt e.g. an 18G Tuohy needle (Figure 3).
Figure 3: The “Cushion Effect” as seen with blunt and short bevel needles. Deposition of LA in the “wrong plane” when “Cushion effect” is not eliminated
NEEDLES FOR LOR BLOCKS
Various different kinds of LOR needles can be used for LOR blocks
- Simple 21 G hypodermic needle that has been blunted (Figures 4 & 5)
- Epidural needle
- Pencil point spinal needles like Whitacare needle
- Commercially available short bevelled LOR needles
Depending upon the resources and availability, the anesthesiologist can choose any of the needles that they are comfortable with. The details of how to blunt hypodermic needles can be found in the article by Singh and Gulyam Kuruba.[26]
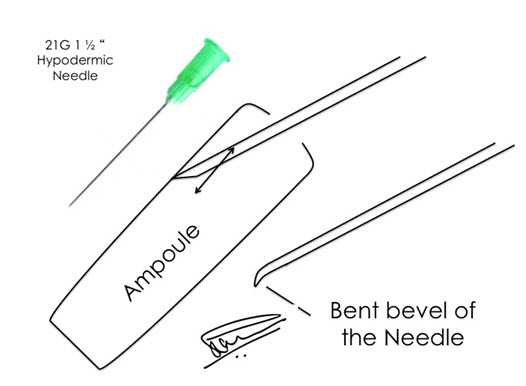
Figure 4: Blunting 21G Hypodermic Needle for LOR blocks. The bevel faces away from the wall and is scratched to form a “beak” pointing inwards.
ELIMINATING THE “CUSHION EFFECT”
There are many ways in which the “cushion effect” can be eliminated. Once this is mastered, the success rate for any LOR blocks improves tremendously. Various methods that can be used are
- Making a small nick in the skin using either a larger hypodermic needle or a surgical blade
- Withdrawing the needle back to just under the skin after initial puncture
- Needle through needle technique, using an introducer with sharp bevel through the skin and then use blunt tipped needle through the introducer.
- In the elderly, the skin and subcutaneous tissues can be “pinched” and puncture made through the skin.
Of the techniques described above, the needle through needle technique is easy to master and provides excellent feedback to the operator in terms of “bounce” and “pops”.
NEEDLE THROUGH NEEDLE TECHNIQUE (PENCIL POINT NEEDLE e.g. WHITACRE NEEDLE)
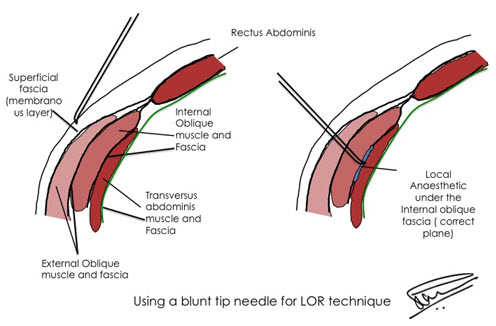
In this technique a sharp introducer is used to puncture the skin. The introducer tip should lie just below the skin in the subcutaneous tissue. This may require the introducer to be withdrawn after initial puncture esp in lean patients and the elderly who have minimal subcutaneous fat. The short beveled blunt needle or pencil point needle like the Whitacre spinal needle is then inserted through the introducer. Once we have negotiated the first layer of muscle i.e. the EO, we actively look for the gentle “bounce” over the EO fascia before piercing it with a feel of “pop”. The needle is then further advanced through the IO muscle till the tip lies over the IO fascia and the same sequence of “bounce” followed by “pop” and deposition of LA in the plane is done. We have found that this technique, using the “bounce” followed by “pop” consistently increases the success rates and potentially deceases, and in-fact, almost totally eliminates the complications like peritoneal puncture or visceral injuries. [26] (Figure 6)
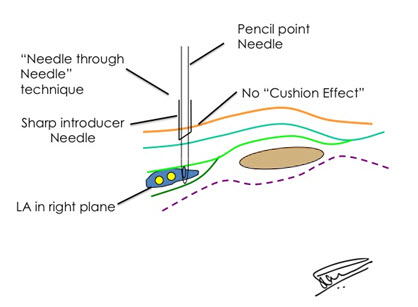
Figure 6: Needle through Needle for eliminating “Cushion Effect” for correct needle tip placement
LANDMARKS FOR TAP BLOCK AND ILIOINGUINAL NERVE (IIN) & ILIOHYPOGASTRIC NERVE (IHN) BLOCKS IN THE TA PLANE
For lower abdominal transverse or pfannestiel incisons, we recommend the use of IIN and IHN blocks in the TA plane. The landmark for this block is the anterior superior iliac spine (ASIS). The approach we follow, is based on a study by Eichenberger et al. [27] Our injection point is about 5 cm cranial and 5 cm posterior to the ASIS over the iliac crest. At this point, both the IIN and IHN lie between the IO and TA muscles in the TA plane, so basically, this is a TAP block. This location of nerves has been confirmed by cadaveric studies done as far back as 1952 and more recently by Rozen and colleagues in 2008. [14] (Figures 7 & 8)
For lower abdominal midline incision below the umbilicus, it is better to perform a standard TAP block. For this we mark the midpoint between the highest point of iliac crest and the costal margin in the midaxillary line. The introducer and the needle is inserted perpendicular to the skin and we look for the gentle “bounce” followed by “pop” as describe earlier in the article.
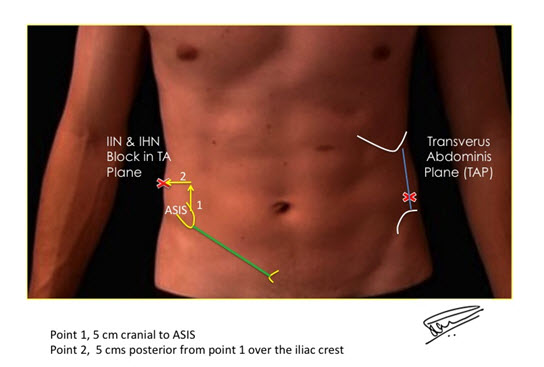
Figure 7: Landmarks for IIN and IHN in TA Plane
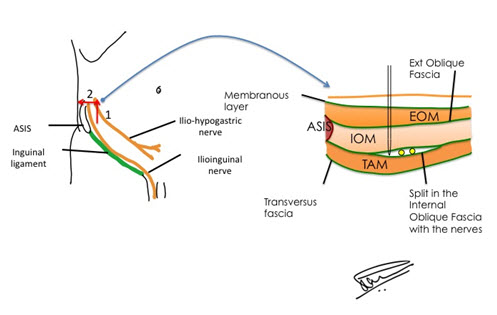
Figure 8: IIN & IHN Block in TA Plane
Legend: ASIS – Ant Superior Iliac Spine; EOM – External Oblique Muscle; IOM – Internal Oblique Muscle; TRAM – Transversus Abdominis Muscle.
LOCAL ANESTHETICS FOR THE BLOCKS
These blocks are done bilaterally and hence it is important that the volume and the total dosage are kept within the safe limits of 2 ml/kg for (levo-) bupivacaine and 3mg/kg for ropivacaine. The volume needed is 15–20 ml on each side for the effective blockade of the nerves.
USING EPIDURAL NEEDLES AND CATHETERS IN LOR BLOCKS
Needle insertion point is as described above in the article. In this technique, it is important to make a small nick in the skin using a No. 11 surgical blade or after initial puncture of skin with the needle itself, withdraw the needle tip till the skin and then look for the LOR to air or saline. Advantage of using epidural needle is that, we can thread an epidural catheter for continuous post-operative infusion or intermittent boluses of LA where prolonged analgesia is required. Disadvantage being, the catheter need to be inserted bilaterally and at times it can be tricky to retain the catheter in place.
SOME IMPORTANT ASPECTS OF LOR TAP BLOCKS
- Foremost, we have to remember that TAP blocks or IIN and IH nerve blocks only provide myocutaneous analgesia and do not cover pain arising from the viscera. Visceral pain often occurs from inflammation, ischemia or pressure. This pain is often mild and can be taken care off with simple analgesics like paracetamol and NSAIDs.
- These blocks are volume blocks and it is important to keep the safe dosage and volumes in mind. Ideally 0.4-0.5ml/kg/side of LA is required for an effective block. Use of lower volumes may lead to failure. Low concentration and larger volumes are better than high concentration and low volumes.
- The block onset is slower with long acting LA and you may need as long as thirty minutes for an effective block to set in. For quick onset, Lignocaine can be used at the outset and a repeat block performed at the end of the surgery with longer acting LA.
COMPLICATIONS
No technique is without any disadvantages or side effects. These cannot be eliminated but can be minimized with appropriate education and training. All kind of complications have been reported in the literature and include the following;
- Visceral organ injury [28]
- LA systemic toxicity (LAST)
- Peritoneal puncture
- Deposition of LA in wrong plane
However in our practice, we have not encountered such complications till date as we regularly address the “cushion effect” in all the LOR blocks and are very meticulous in looking for active “bounce” followed by “pop”. Visceral injuries (liver injury) are not unique to blind blocks and have been reported even with use of US guided TAP blocks. [29]
DO WE NEED TO STOP DOING LOR BLOCKS?
Use of blind technique has been questioned recently in a publication titled “should we stop doing Blind LOR TAP block?” by McDermott et al published in BJA. [ref] In this study 36 adult patients were recruited and experienced anesthesiologists were asked to perform LOR TAP blocks with real time imaging during injection. The study found only 23.6% injections were in proper plane and the incidence of peritoneal puncture was as high as 18%. There are many deficiencies in this study, namely
- They have not addressed the issue of “cushion effect”. There is no mention about how the cushion effect was eliminated. The authors are probably oblivious of this effect that is the commonest cause for failures and malpositioning of needle tip in the wrong planes.
- There is no mention about use of appropriate technique like “bounce” followed by “pop” for localization of right planes.
- There is no mention about the use of, looking for end points like “free back flow” of LA in the needle hub after completion of the injection which would rule out malposition of the tip. If the needle tip lies in the abdominal cavity there will not be any free backflow of LA unlike when LA is deposited in the TA plane. Similarly no free flow of LA is observed when LA injection is intra-muscular.
- Last but not the least, what training have these experienced anesthesiologists had in LOR blocks?
So in brief, LOR blocks are here to stay.
CONCLUSION
While it may be prudent to choose general anesthesia for emergency cesarean sections due to maternal hemorrhage or cord prolapse, RA in the form of a subarachnoid block does play a role in the anesthetic management of emergency cesarean sections where the indication is a non reassuring CTG. TAP blocks or IIN and IH nerve blocks in TAP plane can not only be used for anesthesia in situations where GA or neuraxial blocks may be contra-indicated, they can also be used for post-operative analgesia in obstetric emergencies or in combination with GA to reduce the requirements for opioids. These blocks can be administered with minimal resources and great effectiveness if the anatomy and the “cushion effect” are understood. It is also important to master the end points i.e. “bounce” followed by “pop” and free flow of LA at the end of injection ensure deposition of LA in the right plane.
REFERENCES
- Steve Yentis and Paul Clyburn on behalf of the MBRRACE-UK Anaesthetic chapter writing group, Lessons for Anaesthesia, In Knight M, Kenyon S, Brocklehurst P, Neilson J, Shakespeare J, Kurinczuk JJ (Eds.) on behalf of MBRRACE-UK. Saving Lives, Improving Mothers’ Care – Lessons learned to inform future maternity care from the UK and Ireland Confidential Enquiries into Maternal Deaths and Morbidity 2009–12. Oxford: National Perinatal Epidemiology Unit, University of Oxford 2014: p45-55.
- WHO, UNICEF, UNFPA, The World Bank and the United Nations Population Division.Trends in maternal mortality: 1990 to 2013, Estimates by WHO, UNICEF, UNFPA, The World Bank and the United Nations Population Division. May 2014. Available at: http://www.who.int/reproductivehealth/publications/monitoring/maternal-mortality-2013/en/
- Gale R, Zalkinder-Luboshitz I, Slater PE. Increased neonatal risk from the use of general anesthesia in emergency caesarian section: A retrospective analysis of 374 cases. J Reprod Med. 1982 Nov;27(11):715-9. [PubMed]
- Marx GF, Luykx WM, Cohen S. Fetal-neonatal status following caesarian section for fetal distress. Br J Anaesth 1984 Sep;56(9):1009-13. [PubMed]
- American College of Obstetricians and Gynecologists; Committee on Obstetric Practice, (1998) Inappropriate use of the terms fetal distress and birth asphyxia. Number 197, February1998 (replaces no.137, April 1994). Int J Gynaecol Obstet. 1998 Jun;61(3):309-10. [PubMed]
- Royal College of Anaesthetists, (2012) ‘Raising Standards: A Compendium of audit Recipes’, 3rd edition, London: RCoA Publication. Available at: http://www.rcoa.ac.uk/ARB2012
- American Society of Anesthesiologists Task Force on Obstetric Anesthesia. Practice Guidelines for Obstetric Anesthesia: An Updated Report by the American Society of Anesthesiologists Task Force on Obstetric Anesthesia’, Anesthesiology 2007 Apr;106(4):843-63. [PubMed]
- Halpern SH and Leighton BL, (2005) ‘Epidural analgesia and the progress of labor, In Halpern SH, Douglas MJ (ed.) Evidence-Based Obstetric Anesthesia, Oxford UK: Blackwell, pp. 10–22.
- Sia AT, Fun WL, Tan TU. The ongoing challenges of regional and general anaesthesia in obstetrics. Best Pract Res Clin Obstet Gynaecol 2010;24:303–12. [PubMed] doi: 10.1016/j.bpobgyn.2009.12.001.
- Gogarten W. Spinal anaesthesia for obstetrics. Best Pract Res Clin Anaesthesiol. 2003 Sep;17(3):377-92.[PubMed]
- Bromage PR. Shnider SM and Levinson G (1993), ‘Neurologic complications of regional anesthesia for obstetrics’, in Anesthesia for Obstetrics, 3rd ed, Baltimore: Williams and Wilkins, pp. 443–4.
- Avery DM. Obstetric Emergencies. American Journal of Clinical Medicine 2009;6(2):42-47
- Farragher RA and Laffey JG, (2006) ‘Postoperative pain management following cesarean section’, In Shorten G, Carr D, Harmon D (ed.), Postoperative pain management: an evidence-based guide to practice, 1st edition, Philadelphia PA: Saunders Elsevier, pp. 225–38.
- Rozen WM, Tran TMN, Ashton MW, Barrington MJ, Ivanusic JJ, Taylor GI. Refining the course of the thoracolumbar nerves. A new understanding of the innervations of the anterior abdominal wall. Clin Anat. 2008 May;21(4):325-33. [PubMed] doi: 10.1002/ca.20621.
- McDonnell JG, O’Donnell BD, Farrell T, Gough N, Tuite D, Power C, Laffey JG. Transversus abdominis plane block: a cadaveric and radiological evaluation. Reg Anesth Pain Med 2007;32:399-404. [PubMed]
- Tran TMN, Ivasunic JJ, Hebbard P, Barrington MJ. Determination of spread of injectate after ultrasound-guided transverses abdominis plane block: a cadaveric study. Br J Anaesth 2009;102:123-7. [PubMed] doi: 10.1093/bja/aen344.
- Rafi AN. Abdominal field block: a new approach via the lumbar triangle. Anaesthesia 2001;56:1024-6. [PubMed]
- Jankovic ZB, du Feu FM, McConnell P. An anatomical study of the transversus abdominis plane block: location of the lumbar triangle of Petit and adjacent nerves. Anesth Analg 2009;109(3):981-5. [PubMed] doi: 10.1213/ane.0b013e3181ae0989.
- McDonnell JG, O’Donnell BD, Curley G, Hefferman A, Power C, Laffey JG. Analgesic efficacy of transversus abdominis plane (TAP) block after abdominal surgery: a prospective randomized controlled trial. Anesth Analg 2007;104:193-7. [PubMed]
- Carney J, McDonnell JG, Ochana A, Bhinder R, Laffey JG. The transversus abdominis plane block provides effective postoperative analgesia in patients undergoing total abdominal hysterectomy’, Anesth Analg 2008;107:2056-60. [PubMed] doi: 10.1213/ane.0b013e3181871313.
- O’Donnell BD, McDonnell JG, McShane AJ. The transversus abdominis plane (TAP) block in open retropubic prostatectomy. Reg Anesth Pain Med 2006;23:91. [PubMed]
- McDonnell JG, Curley G, Carney J, Benton A, Costello J, Maharaj CH, Laffey JG. The analgesic efficacy of transversus abdominis plane block after cesarean delivery: a randomized controlled trial. Anesth Analg 2006;106:186-91. [PubMed] doi: 10.1213/01.ane.0000290294.64090.f3.
- El-Dawlatly AA, Turkistani A, Kettner SC, Machata AM, Delvi MB, Thallaj A, et al. Ultrasound-guided transverses abdominis plane block: description of a new technique and comparison with conventional systemic analgesia during laparoscopic cholecystectomy. Br J Anaesth 2009;102:763-7. [PubMed] doi: 10.1093/bja/aep067.
- Niraj G, Searle A, Mathews M, Misra V, Baban M, Kiani S, Wong M. Analgesic efficacy of ultrasound-guided transversus abdominis plane block in patients undergoing open appendicectomy. Br J Anaesth 2009;103:601-5. [PubMed] [Free full text]
- Mishriky BM, George RB, Habib AS. Transversus abdominis plane block for analgesia after cesarean delivery: A systematic review and meta-analysis. Can J Anaesth 2012;59(8):766–78. [PubMed] doi: 10.1007/s12630-012-9729-1.
- Shiv Kumar Singh and S. M. Gulyam Kuruba, “The Loss of Resistance Nerve Blocks,” ISRN Anesthesiology, vol. 2011, Article ID 421505, 10 pages, 2011. doi:10.5402/2011/421505 [Free full text]
- Eichenberger U, Greher M, Kirchmair L, Curatolo M, Morigg lB. Ultrasound-guided blocks of the ilioinguinal and iliohypogastric nerve: accuracy of a selective new technique confirmed by anatomical dissection. Br J Anaesth 2006;97(2):238–243. [PubMed]
- Farooq M, Carey M. A case of liver trauma with a blunt regional anesthesia needle while performing transversus abdominis plane block. Reg Anesth Pain Med 2008;33:274. [PubMed] doi: 10.1016/j.rapm.2007.11.009.
- Lancaster P, Chadwick M. Liver trauma secondary to ultrasound-guided transversus abdominis plane block. Br J Anaesth 2010;104:509-10. [PubMed] doi: 10.1093/bja/aeq046



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube