
Nur Yapar, MD*, Mert Akan, MD**, Vildan Avkan-Oguz, MD*,
Cem M. Ergon, MD***, Munir Hancer, MD****, Mine Doluca, MD*****
*Professor, Dept of Infectious Diseases and Clinical Microbiology
**Assistant Professor, Dept of Anesthesiology and Reanimation,
***Associate Professor, ****Consultant, *****Professor
Dept of Microbiology and Clinical Microbiology
Faculty of Medicine / Intensive Care Unit of Anesthesiology, Dokuz Eylül University, Faculty of Medicine, Izmir (Turkey)
Correspondence: Dr. Mert Akan, Department of Anesthesiology, Dokuz Eylül University, Faculty of Medicine
Balcova, 35340, Izmir, Turkey; Tel: +90 (232) 4122954; Fax: +90 (232) 4122800; E-mail: mert.akan@deu.edu.tr
ABSTRACT
Background: Invasive fungal infections are important and life threatening infections seen in immunocompromised and critically ill patients. Candida species are the most common fungal pathogens among those patients and the most commonly recognized clinical manifestation is candidemia. The aim of this study was to investigate the incidence, risk factors and 30-day mortality associated with candidemia in the intensive care unit (ICU).
Materials and Methods: A retrospective cohort study in a tertiary care hospital ICU was undertaken from January 2004 to December 2008. Demographic and clinical data were collected from medical and microbiology laboratory records retrospectively.
Results: In five years period, 66 candidemia cases were identified among 1076 cases. Overall incidence of candidemia was 12.3 per 1000 admissions and 23.1/10000 patient days. Candida albicans was the most common species (53.1%) isolated from blood specimens followed by Candida parapsilosis (21.1%). The frequencies of tracheotomy, femoral artery catheterisation, red blood cell transfusions, parenteral nutrition, abdominal surgery, and previous use of antibiotics were significantly high in candidemia group. In multivariate logistic regression model, parenteral nutrition and use of broad spectrum antibiotic combinations were found to be associated with candidemia. Crude mortality rate at 30th day was 43.9% and mortality rate of candidemia associated with C. albicans was significantly higher than with non-albicans Candida strains.
Key words: Candidemia; Intensive care units; Incidence; Risk factors; Mortality
Citation: Yapar N, Akan M, Avkan-Oguz V, Ergon CM, Hancer M, Doluca M. Risk factors, incidence and outcome of candidemia in a Turkish intensive care unit: a five-year retrospective cohort study. Anaesth Pain & Intensive Care 2014;18(3):265-71
INTRODUCTION
In parallel with advances organ transplantation and cancer treatment, survival rates of immunocompromised patients at risk of fungal infections have improved. Likewise, in recent years the use of invasive monitoring and aggressive therapeutic techniques increased in the intensive care units (ICUs) and this also contributed to an increase in the ratio of patients susceptible to fungal infections.1-4 Invasive fungal infections are important and life threatening infections seen in immunocompromised and critically ill patients. Candida species are the most common fungal pathogens isolated from those patients and the most commonly recognized clinical manifestation is candidemia.3 Candida species are the fourth leading cause of nosocomial blood stream infections (BSIs) in USA and sixth in Turkey.5,6 In a prospective survey conducted by European Confederation of Medical Mycology (ECMM) in seven European countries, incidence rates of candidemia were reported between 0.20 and 0.38 per 1000 hospital admissions. Of those patients, 40.2% was hospitalized in intensive care units.7 In our hospital, the incidence of candidemia was reported as 0.56/1000 hospital admissions in 2000-2003 period and 53.8% of the patients with candidemia were hospitalized in ICU.8 Candida infections are also associated with high mortality rates, increased length of hospital stay and health care costs.4,5,9-11
METHODOLOGY
Data collection:
Crude mortality rate from candidemia was defined as the death rate within 30 days after the first isolation of Candida spp. form blood culture.
Cultivation of blood samples:
BACTEC 9240 (plus, aerobic/F, Becton Dickinson, Sparks, MD, USA) blood culture system was used for taking blood samples. For this purpose, 10 ml of blood taken from peripheral veins and placed lines was inoculated into the sample bottles and sent to microbiology laboratory. Bottles were then placed in a BACTEC blood culture device in laboratory and incubated for seven days. 0.1-ml aliquotswere withdrawn from each positive bottle if growth signal was flagged by the system and they were subcultured on to blood agar (Becton Dickinson, BD Diagnostics, Heidelberg, Germany), chocolate agar (Becton Dickinson, BD Diagnostics, Heidelberg, Germany) and Eosin Methylene Blue agar (Becton Dickinson, BD Diagnostics, Heidelberg, Germany). Agar plates were incubated at 37ºC for 24-48 hours and the growth on the plates were evaluated. If yeast growth was obtained, agar plates were processed in Mycology laboratory.
Identification of yeasts:
Statistical analysis:
The chi-square test or Fisher’s exact test was used for evaluating categorical variables and the t-test for continuous variables. Fisher’s Exact test is employed when sample sizes are small, in practice. Therefore we used this test for small sample sizes. A p-value of <0.05 was considered statistically significant. Variables that found as significant in these tests were considered as candidates for the multivariate analysis. To investigate risk factors independently associated with candidemia, we performed multivariate, backwards stepwise, logistic regression analysis. All statistical analyses were performed with Statistical Package for the Social Sciences (SPSSTM, Version 15.0, Chicago, Il, USA) and CDC software EPI INFOTM (version 6.0, Atlanta,GA,USA).
RESULTS
Incidences
During five year study period, 5353 patients admitted to the ICU were included in the study and 1076 of them were hospitalized more than two days. Of these1076 patients, 66 developed candidemia. The median interval from ICU admission to the onset of candidemia was 15 (3-188) days.
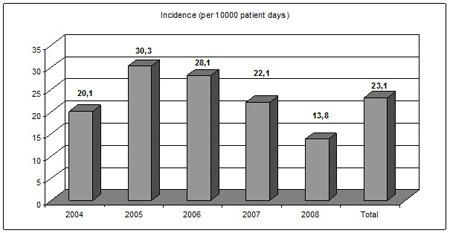
Total incidence rate of candidemia was 12.3 per 1000 admissions and 23.1/10 000 patient days. A significant increase in candidemia incidence was noted between year 2004 and 2005 (p=0.03). After which, there was a gradual decline in candidemia (Figure 1).
Figure 1: Annual incidence rates of candidemia
Demographic and clinical characteristics
Of the 66 candidemia cases, 53% (n=35) were males and 47% (n=31) were females. Mean age was 54.4 (SD±23.9) years in candidemia group and 53.2 (SD±23.0) years in control group. Of the candidemia cases, 43.9% (n=29) were surgical and 56.1% (n=37) were medical patients. There was no statistically significant difference in terms of demographic features or underlying illnesses between cases and controls (Table 1).
Table 1: Patient characteristics and underlying diseases
|
Parameter |
Cases |
Controls |
p |
| Age |
54.4±23.9 |
53.2±23.0 |
0.698 |
| Gender (Male) |
35 (53) |
637 (63) |
0.103 |
| Diabetes mellitus |
9 (13.6) |
165 (16.3) |
0.564 |
| Chronic renal failure |
5 (7.5) |
52 (5.1) |
0.394 |
| COPD* |
6 (9) |
118 (11.7) |
0.523 |
| Trauma |
8 (12.1) |
213 (21.1) |
0.08 |
| Corticosteroid therapy |
5 (7.5) |
50 (4.9) |
0.378 |
| Cancer chemotherapy |
7 (10.6) |
51 (5) |
0.053 |
| Liver transplantation |
7 (10.6) |
87 (8.6) |
0.579 |
| Malignancy |
20 (30.3) |
210 (20.8) |
0.06 |
| APACHE II (mean) |
22.9±6.8 |
20.4±7.6 |
0.04 |
*COPD: Chronic obstructive pulmonary disease
Fungal isolates
Table 2: Number of Candida species isolated from blood in years
|
Candida species |
Years |
||||||
|
2004 |
2005 |
2006 |
2007 |
2008 |
Total |
||
| Candida albicans |
6 |
8 |
7 |
10 |
4 |
35 |
|
| Candida parapsilosis |
1 |
3 |
6 |
1 |
3 |
14 |
|
| Candida tropicalis |
1 |
2 |
1 |
1 |
0 |
5 |
|
| Candida glabrata |
0 |
0 |
2 |
1 |
1 |
4 |
|
| Candida utilis |
0 |
1 |
1 |
2 |
0 |
4 |
|
| Candida lusitaniae |
0 |
2 |
0 |
0 |
0 |
2 |
|
| Candida krusei |
0 |
1 |
0 |
0 |
0 |
1 |
|
| Candida kefyr |
0 |
0 |
1 |
0 |
0 |
1 |
|
| Total |
8 |
17 |
18 |
15 |
8 |
66 |
|
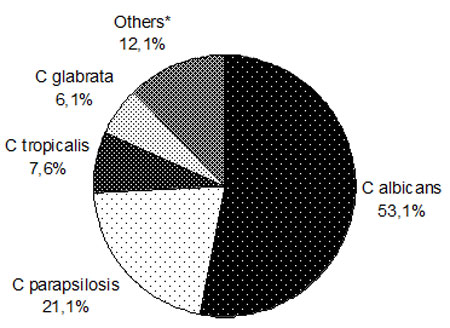
Figure 2: Species distribution of isolates [*Others: C. utilis, C. lusitaniae, C. krusei, C. kefyr ]
Risk Factors
At first, we performed chi-square test for evaluation of invasive procedures and therapeutic approaches as possible risk factors. The frequencies of tracheotomy, femoral artery catheterization, RBC transfusion, TPN, abdominal surgery, and previous use of antibiotics were significantly high in candidemia group (Table 3). In multivariate logistic regression model, TPN (p= 0.02, OR= 1.86, 95% CI= 1.07-3.23) and previous use of broad spectrum antibiotic combinations (more than two antibiotics) (p<0.001, OR=3.2, 95% CI=1.86-5.53) were associated with an increased risk of candidemia.
Table 3: Invasive procedures and therapy of patients
|
Invasive procedures and therapy |
Cases |
Controls |
p |
| Presence of urinary catheter |
65 (98.4) |
995 (92.4) |
0.984 |
| Presence of CVC |
66 (100) |
956 (88.8) |
0.054 |
| Mechanical ventilation |
64 (96.9) |
936 (86.9) |
0.187 |
| Hemodialysis |
10 (15.1) |
108 (10.0) |
0.261 |
| Tracheotomy |
24 (36.3) |
192 (17.8) |
<0.01 |
| Erythrocyte transfusion |
51 (77.2) |
556 (51.6) |
<0.01 |
| Prior surgical procedures (total) |
45 (68.2) |
618 (57.4) |
0.25 |
|
34 (51.5) |
376 (34.9) |
0.02 |
|
5 (7.5) |
84 (7.8) |
0.832 |
| Nasogastric tube |
64 (96.9) |
950 (88.2) |
0.326 |
| TPN |
42 (63.6) |
413 (38.3) |
<0.01 |
| Catheterization of femoral artery |
15 (22.7) |
123 (11.4) |
0.01 |
| Previous use of antibiotics |
64 (96.9) |
843 (78.3) |
<0.01 |
|
39 (59.1) |
246 (22.8) |
<0.01 |
|
14 (21.2) |
181 (16.8) |
0.501 |
|
17 (25.7) |
199 (18.4) |
0.234 |
|
42 (63.6) |
232 (21.5) |
<0.01 |
|
29 ((43.9) |
163 (15.1) |
<0.01 |
|
8 (12.1) |
123 (11.4) |
0.989 |
|
33 (50) |
323 (30.0) |
<0.01 |
|
25 (37.9) |
181 (16.8) |
<0.01 |
| Antifungal agents |
6 (9) |
68 (6.3) |
0.463 |
Outcome
Mean length of stay of patients was 30.9±33. days in candidemia group and 12.9±13 days in control group (p<0.001). Crude mortality rate on day 30 was 43.9% (29 out of 66) in the candidemia group whereas it was 32.2% (326 of 1010) in the control group. There was no significant difference between the mortality rates of candidemia and control groups (p=0.05). Twenty out of 35 patients (57.1%) and 9 out of 31 (29%) died in C. albicans group and non-albicans Candida group, respectively. Mortality rate of candidemia associated with C. albicans was significantly higher than with non-albicans Candida strains (p=0.02, OR=3.26, 95%CI=1.05-10.4).
DISCUSSION
The median interval from ICU admission to onset of candidemia was 15 (3-188) days in our study which is comparable to formerly published reports [10]. The mean interval between ICU admission and candidemia was 19.0±2.9 days in a French study [17]. Anunnatsiri et al. [19]found that median duration of hospitalization prior to candidemia was 16.5 days. In our study, average length of hospital stay was 18 days longer in candidemia patients than control consistent with the literature [20].
Candida parapsilosis is known to adhere to bio prosthetic surfaces such as catheters forming a biofilm layer of glycosylated serum and can cause epidemics especially in pediatric ICUs [3,5]. The frequency of this pathogen can be explained by inadequate catheter care, increase in use of parenteral nutrition or poor infection control practices mentioned above. The retrospective nature of our study limits the investigation of these factors.
Candida glabrata is one of the fluconazole resistant non-albicans Candida species was not common in our study group. This pathogen has become an important and common species in the United States [24]. In contrast, it is much less common cause of BSIs in most other countries. In some studies from Latin America, Asia-Pacific, Europe and Turkey frequency of candidemia due to C. glabrata was reported between 4% and 10% [5,8,25,26]. In Artemis Disk Global Antifungal Surveillance Program, a total of 201 653 isolates were collected from 133 centers between January 2001 and December 2007. The frequency of C. glabrata isolation was lower in Turkey (3.1%) than other countries [27]. The reasons for the frequency variation of C. glabrata are not clear but may include prior azole exposure, age, geographic location, blood culture systems used for diagnosis or other unknown features [5].
Risk factors for candidemia can be divided in to two groups: Host related factors and underlying health conditions; health-care associated factors such as catheters, surgical interventions and medications. In our study, there was no statistically significant difference in terms of underlying illnesses between the cases and controls except for higher APACHE II scores in candidemia group than in controls.ACHE II scores of cases were significantly higher than control patients. However we could not reach APACHE II scores of all patients from medical records reviewed retrospectively which is one of the limitations of our study.
Predisposing factors for candida BSIs described in literature are: previous exposure to antibiotics or antifungals, central venous or urinary catheters, total parenteral nutrition, steroids, prolonged hospitalization, abdominal surgery, immunosuppressive therapy, and renal failure [5,16,23,28]. We found similar risk factors in our study group. However, central venous catheterization and mechanical ventilation were not found to be significant in our study. In multivariate analysis, TPN and previous use of broad spectrum antibiotic combinations especially containing glycopeptides, carbapenems, aminoglycosides and beta lactam- beta lactamase inhibitors were found to be independently associated with an increased risk of candidemia.
Mortality was significantly higher for patients infected with C. albicans than the others infected with non-albicans Candida species in the study presented here. This is in contrast to the study by Bassetti et al. [23] who found that crude mortality was 55% in all patients with candidemia although, there was no statistically significant difference between the mortality rates of albicans and non-albicans candidemia patients. Similarly, Chow et al. [30] found the mortality rates of BSIs due to C. albicans and non-albicans Candida species 58% and 57% respectively. In contrast, Dimopoulos et al. [18] reported significantly high mortality for BSIs due to non-albicans species. In our study , the most common non-albicans Candida isolate was C. parapsilosis which has relatively low mortality among others and this could influence on mortality rates.
CONCLUSION
In conclusion, candidemia is an important and life threatening infection in the ICU. According to our study, in our hospital C. albicans is the predominant species and we found no increase in annual rates of azole resistant non-albicans Candida species during the study period. Important risk factors were invasive procedures and medications. Candidemia should be suspected in patients with these risk factors and diagnostic/therapeutic interventions should be performed immediately.
Acknowledgement: The authors would like to thank to Prof. Dr. Reyhan Ucku for her support on statistical analyses.
Conflict of Interest: There is no potential conflict of interest or source of funding to declare.
REFERENCES
- Richardson MD. Changing patterns and trends in systemic fungal infections. J Antimicrob Chemother 2005;56:i5-11. [PubMed] [Free FullText]
- De Pauw BE. Increasing fungal infections in the intensive care unit. Surgical Infections 2006;7:S93-96. [PubMed]
- Pappas PG. Invasive candidiasis. Infect Dis Clin N Am 2006;29:485-506. [PubMed]
- Tufano R. Focus on risk factors for fungal infections in ICU patients. Minerva Anestesiol 2002;68:269-272. [PubMed]
- Pfaller MA, Diekema DJ. Epidemiology of invasive candidiasis: a persistent public health problem. Clin Microbiol Rev 2007;20:133-163. [PubMed] [Free Full Text]
- Inan D, Saba R, Yalcin AN, Yilmaz M, Ongut G. Device-associated nosocomial infection rates in Turkish medical-surgical intensive care units. Infect Control Hosp Epidemiol 2006;27:343-348. [PubMed]
- Tortorano MA, Peman J, Bernhardt H, et al. Epidemiology of candidaemia in Europe: Results of 28-month European Confederation of Medical Mycology (ECMM) hospital-based surveillance study. Eur J Clin Microbiol Infect Dis 2004;23:317-322. [PubMed]
- Yapar N, Uysal U, Yucesoy M, Cakir N, Yuce A. Nosocomial bloodstream infections associated with Candida species in a Turkish university hospital. Mycoses 2006;49:134-138. [PubMed]
- Guery BP, Arendrup MC, Auzinger G, Azoulay E, Borges Sá M, Johnson EM. Management of invasive candidiasis and candidemia in adult non-neutropenic intensive care unit patients: Part II. Treatment Intensive Care Med 2009;35:206-214. [PubMed]
- Bouza E, Munoz P. Epidemiology of candidemia in intensive care units. Int J Antimicrob Agents 2008;32:S87-91. [PubMed]
- Petri MG, König J, Moecke HP, et al. Epidemiology of invasive mycosis in ICU patients: a prospective multicenter study in 435 non-neutropenic patients. Intensive Care Med 1997;23:317-325. [PubMed]
- De Pauw B, Walsh TJ, Donnely JP, et al. Revised definitions of invasive fungal disease from the European Organization for Research and Treatment of Cancer/Invasive Fungal Infections Cooperative Group and the National Institute of Allergy and Infectious Diseases Mycoses Study Group (EORTC/MSG) Consensus Group. Clin Infect Dis 2008;46:1813-1821.
- Winn WC, Allen SD, Janda WM, Koneman EW, Procop G, Schreckenberger PC, Woods G. In: The Color Atlas and Textbook of Diagnostic Microbiology. 6th ed. Philadelphia: JB Lippincott Co; 2006:1216-1230.
- Larone DH. In: Medically Important Fungi: A Guide to Identification. 4th ed. Washington, DC: ASM press; 2002:109-143.
- Guery BP, Arendrup MC, Auzinger G, Azoulay E, Borges Sá M, Johnson EM. Management of invasive candidiasis and candidemia in adult non-neutropenic intensive care unit patients: Part I. Epidemiology and diagnosis. Intensive Care Med 2009;35:55-62. [PubMed]
- Luzzati R, Allegranzi B, Antozzi L, et al. Secular trends in nosocomial candidaemia in non-neutropenic patients in an Italian tertiary hospital. Clin Microbiol Infect Dis 2005;11:908-913. [PubMed]
- Bougnoux ME, Kac G, Aegerter P, d’Enfert C, Fagon JY, CandiRea Study Group. Candidemia and candiduria in critically ill patients admitted to intensive care units in France: incidence, molecular diversity, management and outcome. Intensive Care Med 2008;34:292-299. [PubMed]
- Dimopoulos G, Ntziora F, Rachiotis G, Armaganidis A, Falagas ME. Candida albicans versus non-albicans intensive care unit-acquired bloodstream infections: Differences in risk factors and outcome. Anesth Analg 2008;106:523-529. [PubMed]
- Anunnatsiri S, Chetchotisakd P, Mootsikapun P. Fungemia in non-HIV infected patients: a five-year review. Int J Infect Dis 2009;13:90-96. [PubMed]
- Zaoutis TE, Argon J, Chu J, et al. The epidemiology and attributable outcomes of candidemia in adults and children hospitalized in the United States: a propensity analysis. Infect Dis 2005;41:1232-1239. [PubMed] [Free Full Text]
- Leroy O, Gangneux JP, Montravers P, et al. Epidemiology, management, and risk factors for death of invasive Candida infections in critical care: A multicenter, prospective, observational study in France (2005-2006). Crit Care Med 2009;37:1612-1618. [PubMed]
- Xess I, Jain N, Hasan F, Mandal P, Banarjee U. Epidemiology of candidemia in a tertiary care centre of north India: 5-year study. Infection 2007;35:256-259. [PubMed]
- Bassetti M, Trecarichi EM, Righi E, et al. Incidence, risk factors, and predictors of outcome of candidemia. Survey in 2 Italian university hospitals. Diagn Microbiol Infect Dis 2007;58:325-331. [PubMed]
- Moran C, Grussemeyer CA, Spalding JR, Benjamin DK, Reed SD. Comparison of costs, length of stay and mortality associated with Candida glabrata and Candida albicans bloodstream infections. Am J Infect Control 2010;38:78-80. [PubMed] [Free Full Text]
- Comert F, Kulah C, Aktas E, Eroglu O, Ozlu N. Identification of Candida species isolated from patients in intensive care unit and in vitro susceptibility to fluconazole for a 3-tear period. Mycoses 2006;50:52-57. [PubMed]
- Bakir M, Cerikcioglu N, Barton R, Yagci A. Epidemiology of candidemia in a Turkish tertiary care hospital. APMIS 2006;114:601-610. [PubMed]
- Pfaller MA1, Diekema DJ, Gibbs DL, Newell VA, Barton R, Bijie H,. Geographic variation in the frequency of isolation and fluconazole and voriconazole susceptibilities of Candida glabrata: an assessment from the ARTEMIS DISK global antifungal surveillance program. Diagn Microbiol Infect Dis 2010;67:162-171. [PubMed]
- Ostorsky-Zeichner L, Pappas PG. Invasive candidiasis in the intensive care unit. Crit Care Med 2006;34:857-862. [PubMed]
- Aliyu SH, Enoch DA, Abubakar II, et al. Candidaemia in a large teaching hospital. A clinical audit. Q J Med 2006;99:655-663. [PubMed] [Free Full Text]
- Chow JK, Golan Y, Ruthazer R, et al. Factors associated with candidemia caused by non-albicans Candida species versus Candida albicans in the intensive care unit. Clin Infect Dis 2008;46:1206-1213. [PubMed] [Free Full Text]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube