
Ali Shahriari1, Maryam Khooshideh2, Mahdi Sheikh*3
1Departement of Anesthesiology, Roozbeh Hospital, Tehran University of Medical Sciences, Tehran (Iran); ashahriari@tums.ac.ir
2Departement of Obstetrics and Gynecology, Arash Hospital, Tehran University of Medical Sciences, Tehran (Iran); khooshide@yahoo.com
3Maternal, Fetal and Neonatal Research Center, Tehran University of Medical Sciences, Tehran (Iran); mahdisheikh@gmail.com
*Correspondence: Mahdi Sheikh, MD, PhD, Maternal, Fetal and Neonatal Research Center, Vali-asr Hospital, Imam Khomeini Hospital complexes, Keshavarz Blvd., Tehran 1419733141 (Iran); Phone: 0098-912-8481663; Fax: 0098-21-22834332; Email: mahdisheikh@gmail.com
ABSTRACT
Preoperative checking of the anesthetic equipment which is the primary responsibility of the nurse anesthetist is crucial for patient safety. There are many misconnection possibilities with circle system that can contribute to as highly as 35% of adverse anesthetic outcomes. A 32-year old man was admitted to the operating room (OR) for appendectomy. After the induction of anesthesia and beginning mask ventilation the anesthesiologist noticed that ventilation was not effective, therefore performed endotracheal intubation. The tracheal tube was connected to the Y piece and the mechanical ventilation was started by anesthesia machine. The lungs were not expanding effectively, therefore manual ventilation was began by an ambu bag. Beginning the manual ventilation the anesthesiologist realized an increased resistance against ventilation and an elevated airways pressure. The SpO2 fell to 79% and tachycardia was evident. Physical examinations were suggestive of pneumothorax that occurred within the first 4-5 minutes of starting machine ventilation. Rechecking the anesthesia machine revealed an error in the connection of the anesthesia circuit. We briefly review the current literature and give suggestions to eliminate these mismanagements in the operating room which can be life threatening.
Keywords: Pneumothorax; Anesthesia circuit; Complication; breathing circuit obstruction
Citation: Shahriari A, Khooshideh M, Sheikh M. Pneumothorax caused by anesthesia circuit misconnection. Anaesth Pain & Intensive Care 2016;20(2):214-216
Received: 10 March 2016; Reviewed: 16 March 2016; Corrected: 20 March 2016; Accepted: 28 May 2016
INTRODUCTION
Preoperative checking of the anesthetic equipment which is the primary responsibility of the nurse anesthetist is crucial for patient safety.1 There are many misconnection possibilities with circle system that can contribute to as highly as 35% of adverse anesthetic outcomes, some of these adverse outcomes can be life-threatening.2 We present a case of anesthesia circuit misconnection that caused the development of pneumothorax within minutes.
CASE REPORT
A 32-year old man was admitted to the operating room (OR) for appendectomy. Except for leukocytosis, his initial laboratory findings were normal. In the OR preoperative blood pressure, electrocardiogram, and peripheral capillary oxygen saturation (SpO2) were normal. Anesthesia circuit tubes were connected to the old anesthesia machine (ALPHA DELTA®, Siare, Italy, 1975), circle system, and after a leak test by closing the adjustable pressure limiting (APL) valve, occluding the Y-piece, and pressurizing the circuit to 25 cmH2O with the oxygen flush valve, the induction of anesthesia was started by giving 2 mg midazolam, 150 µg fentanyl, 400 mg thiopentone, and 40 mg atracurium intravenously. Beginning mask ventilation the anesthesiologist noticed that ventilation was not effective, therefore performed endotracheal intubation. The tracheal tube was connected to the Y piece and the mechanical ventilation was started by anesthesia machine. The lung expansion was not adequate, so manual ventilation was started by an Ambu® reanimation bag. During the manual ventilation the anesthesiologist realized an increased resistance against ventilation and an elevated airways pressure (40 cmH2O). The SpO2 fell to 79% and tachycardia was evident. Physical examination was suggestive of pneumothorax that occurred within the first 4-5 minutes of starting machine ventilation, therefore tube thoracostomy tube was inserted into the chest wall at the 5th intercostal space in the left mid axillary line which resulted in reducing the airway resistance and obtaining an acceptable ventilation. Rechecking the anesthesia machine revealed an error in the connection of the anesthesia circuit. The expiration tube and the bag were connected incorrectly to the machine (Figures 1 and 2).
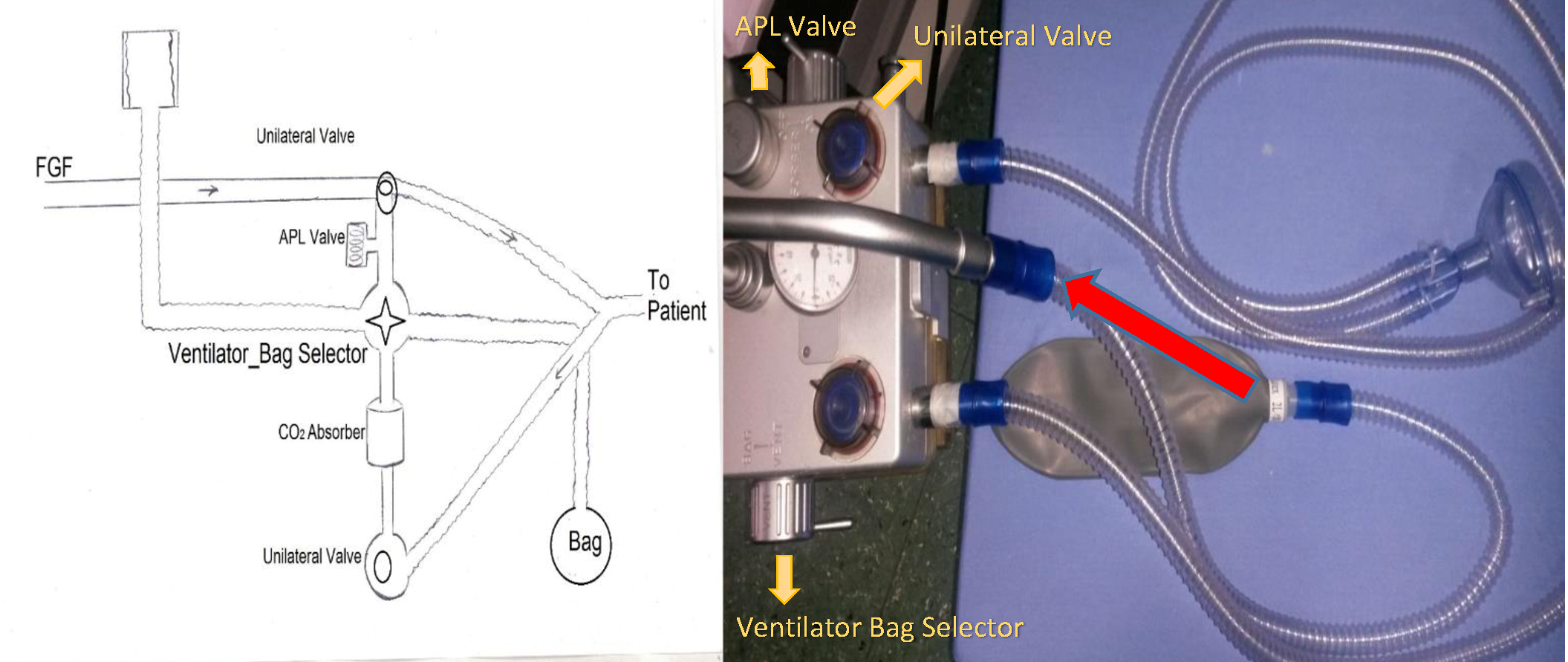
Figure 1: The correct connection of the breathing circuit, the Y piece and the bag (red arrow) are correctly connected to the machine.
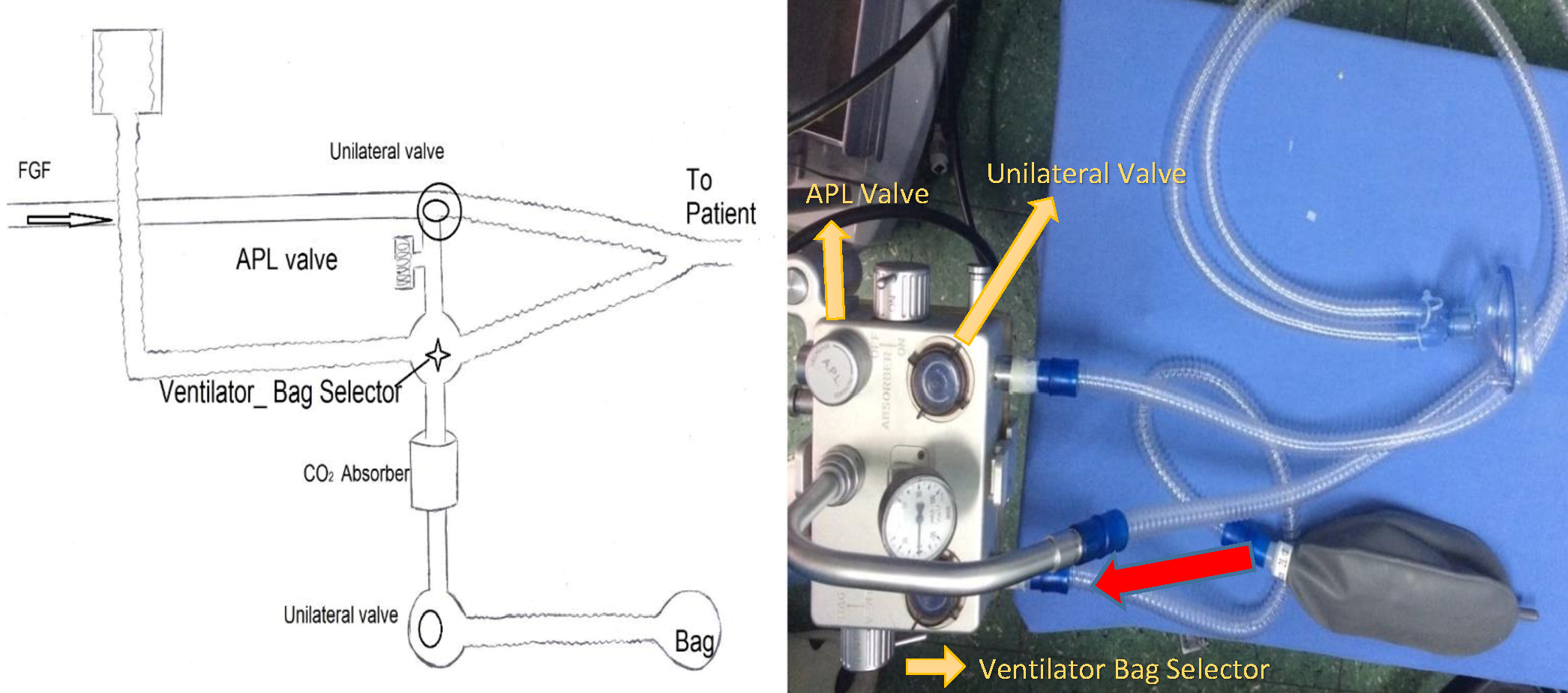
Figure 2: The incorrect connection of the breathing circuit (this case), the expiration tube is incorrectly connected to the connection point of the bag, and the bag is incorrectly connected the connection point of the expiration tube (red arrow).
The anesthesia was continued by mechanical ventilation using 100% O2 and 1% isoflurane. After operation the patient was awakened normally after injection of neostigmine + atropine for reversal of muscle relaxant with an uneventful recovery. Postoperative chest x-ray showed an air rim of more than 1 cm occupying almost 30% of the hemithorax. The chest tube was removed after 3 days when no air was escaping from it and the chest x-ray confirmed re-expansion of the lung.
DISCUSSION
There are many misconnection possibilities with circle system that can contribute to up to 35% of adverse anesthetic outcomes.2 Some of these complications occur after cleaning the anesthetic equipment and cannot be totally eliminated by positive pressure test.3,4 Eckhout and Bhatia reported a case of mechanical obstruction of the expiratory limb of anesthesia circuit which remained undetected until the induction of anesthesia. Although a check of the circuit was performed before the addition of circuit extensions in that case, the obstruction was missed.4
The mechanism causing pneumothorax is this case seems to be barotrauma; airways overpressure due to technical problems can progress to pneumothorax and cardiovascular collapse.3,5 The diagnosis of pneumothorax rests on thinking of the possibility whenever circulatory or respiratory compromise develops in the presence of high risk situations.3,5 In this situation flush valve should not be used because inappropriate use of flush valve can accelerate barotrauma and pneumothorax, thus leading to cardiovascular collapse.3
To eliminate these mismanagements we recommend performing the two bag test,1 after checking the breathing system, vaporizers and ventilator, as the following: Attach the patient end of the breathing system to a test lung or bag. Set the fresh gas flow to 5 l/min and start manual ventilation. Check the whole breathing system and pay attention to the movements of the patient and unidirectional valves. Squeeze both bags to check the function of the APL valve. Turn on the ventilator to ventilate the test lung. Turn off the fresh gas flow or reduce to minimum. Open and close each vaporizer in turn. No loss of volume in the system should be noticed. To prevent intrusion of foreign bodies the breathing systems must be protected with a test lung or bag when not in use.
Financial support: None
Conflict of interest: None
Author contribution: AS + MK: Reporting the case; manuscript editing. MS: Reporting the case; manuscript writing and editing
REFERENCES
- Association of Anaesthetists of Great Britain and Ireland (AAGBI), Hartle A, Anderson E, Bythell V, Gemmell L, Jones H, et al. Checking anaesthetic equipment: association of anaesthetists of Great Britain and Ireland. Anaesthesia 2012;67:660-8. doi: 10.1111/j.1365-2044.2012.07163.x. [PubMed] [Free full text]
- Goneppanavar U, Prabhu M. Anaesthesia machine: checklist, hazards, scavenging. Indian J Anaesth 2013;57:533-40. doi: 10.4103/0019-5049.120151. [PubMed] [Free full text]
- Atlee J. Complications in anesthesia. 2nd Ed. Philadelphia: Elsevier/Saunders; 2007.
- Eckhout GV, Bhatia S. Another cause of difficulty in ventilating a patient. J Clin Aneth. 2003;15:137-9. [PubMed]
- Bacon A, Paix A, Williamson J, Webb R, Chapman M. Crisis management during anaesthesia: pneumothorax. Qual Saf Health Care. 2005 Jun;14(3):e18. [PubMed] [Free full text]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube