
Somboon Thienthong*, Wimonrat Sriraj*, Pulsuk Siripul**, Allen Finley***,
Kesanee Boonyawattanangkool*, Sucheela Kasetwetin*
*Faculty of Medicine, **Faculty of Nursing
Khon Kaen University, Khon Kaen (Thailand)
***IWK Health Center, Dalhousie University, 6299 South St, Halifax, NS B3H 3J5, (Canada)
Correspondence: Somboon Thienthong, Faculty of Medicine, Khon Kaen University, Khon Kaen, Thailand 40002; E-mail: somthi@kku.ac.th
ABSTRACT
Background: Health professionals often underestimate children’s pain and do not treat it as a priority. To raise awareness, the International Association for the Study of Pain has launched a campaign “Global Year against Pain in Children” in 2005, but evidence shows that the pain in children still remains undertreated.
Objective: to determine the prevalence of postoperative pain and the methods for pain treatment in pediatric patients
Methodology: This survey was done on a one-day period in 7 hospitals in northeastern Thailand. Participants were all in-patient children of the age <15 years old or their parents. Exclusion criteria were newborn and critically ill infants. Interesting data included; pain prevalence (pain score > 1 during the past 24 hrs), patients’ perception of receiving pain treatment. Self report pain was measured with the use of either numerical rating scale (0 to 10 scales) or the Faces Pain Scale-Revised (0-5 faces). For those who were unable to self report pain, the Neonatal Infant Pain scale was used. Types of surgery, days after surgery, prescription for pain relief and non-pharmacological measures used for pain relief were also recorded.
Results: One hundred and thirty three of 487 patients (27.3%) were surgical cases. The prevalence of postoperative pain during the past 24 hrs was 69.2%, but those who had moderate to severe pain was 43.6%. Most of children (78.2%) experienced mild or no pain at the time of interview. Almost a half (44.6%) of them perceived they had pain medication upon request and more than half of them (60.1%) used non-pharmacological methods for supplementary pain relief. Two most common prescribed medications were paracetamol (51.9%) and morphine (25.6%). The proportion of medication administered to patients was less than those found in the prescription such as 24.8% vs 51.9% for paracetamol and 8.3% vs 25.6% for IV morphine. Only three conventional routes, oral, intravenous and intramuscular /subcutaneous routes, were found in the prescription for pain treatment.
Conclusion: Postoperative pain in children is still undertreated. Raising awareness and improving knowledge for healthcare providers are needed to be improved.
Keywords: Postoperative pain; Pediatric; Pain management
Citation: Thienthong S, Sriraj W, Siripul P, Finley A, Boonyawattanangkool K, Kasetwetin S. A survey of postoperative pediatric pain management among seven hospitals in northeastern Thailand. Anaesth Pain & Intensive Care 2014;18(1):59-71
BACKGROUND
Health professionals often underestimate children’s pain, and do not treat it as a priority.1 To raise this awareness, the International Association for the Study of Pain (IASP) launched a campaign “Global Year against Pain in Children” in 2005.2 However, evidences show children’s pain is still undertreated. A report in 2011 from Canadian children’s hospitals found that 7 out of every 10 procedures – things like blood sampling and inserting or removing intravenous lines and catheters – children received no pain treatment specific to that procedures.3 de Moura (2011) also reported that the prevalence of pain on the first post-operative day for girls was very high (91.7%).4 In previous studies in Thailand, a survey by Charuluxananan about postoperative pain treatment revealed that 71% of 260 nurse anesthetists across the country reported no record of pain assessment at the surgical ward and intramuscular injection was the most preferable route.5 This finding was similar with the results of a survey in health care providers in northeastern Thailand in that pain assessment was non-standardized and health care providers needed to improve their knowledge and skills about pediatric pain care.6 Although there are evidences that indicated pain in children is still undertreated, but the prevalence of post-operative pain and details of treatment modalities in Thai children were not elucidated. Therefore, the objective of this study was to determine prevalence of postoperative pain and methods of postoperative pain treatment in pediatric patients in northeastern Thailand.
METHODOLOGY
The present study, a descriptive study, was a part of an action research project (pediatric pain management in rural and urban Thailand) aimed at translating knowledge and building a community of practice to improve pediatric pain care in a seven hospitals located in the Isan region, northeastern Thailand. The protocol was approved by the ethical committees of all participated hospitals. Among those seven hospitals, three were large (800-1000 beds) hospitals (one university hospital and two regional hospitals) and four were medium (400-700 beds) provincial hospitals.
The survey was done on a one-day for each hospital on every ward that taking care for pediatric patients between August and November 2012. Participants were all in-patients children of age <15 years old or their parents who were willing to participate. Exclusion criteria were newborn and critically ill infants. The survey had two parts of data collection included; the data that were documented in the patients’ chart (about 80%) and the data obtained by interviewing patients or their parents. For interviewing process, there were four questions, two questions were for pain assessment and other two were for pain treatment. For pain assessment, self report pain was measured with the use of either a numerical rating scale (0 to 10 scales) or the Faces Pain Scale-Revised (FPSR: 0-5 faces). For those who were unable to self report pain, the Neonatal Infant Pain scale (NIPS) was used. For pain treatment, a structured questionnaire developed by the research team about patients’ perception of receiving pain treatment and non-pharmacological pain relief with yes-no-not sure answer was used. Interesting data for the survey included; pain prevalence (pain score > 1 during the past 24 hrs), pain intensity at the time of interview (recent pain), prevalence of severe pain during the past 24 hours (pain score > 7), date and types (minor, moderate, major) of surgery7, pain medications prescribed by physicians, patients’ perception of receiving pain treatment and non-pharmacological pain relief measures used.
Nurse students in the pediatric master degree program from the Faculty of Nursing and pediatric ward nurses from the University Hospital were trained for data collection in this survey, and the data in the collection sheet were verified by Thai researchers. Descriptive statistics were used for data presentation and analyses.
RESULTS
Total number of pediatric patients found in the survey was 487, but only 133 patients (27.3%) were surgical cases and eligible for data analysis. Distribution of pediatric patients in each hospital, age, gender, postoperative days and type of surgery were presented in Table 1. Surgery for small infants was performed in regional or university hospitals but not in the provincial hospitals. Severity of pain and patients’ perception of pain treatment were presented in Table 2. Prevalence of pain was 69.2%, but when focusing on moderate to severe pain, the prevalence was 43.6%. The proportion of moderate to severe pain classified by postoperative days after surgery was presented in Table 3. Most of children (78.2%) experienced mild or no pain at the time of interview. Almost half (44.6%) of them perceived they had pain medication upon request and more than half (60.9%) used non-pharmacological supplementing methods for pain relief. Pain treatment modalities were presented in Table 4. The two most common prescribed medications was paracetamol (51.9%) and morphine (25.6%). The proportion of medication administered to patients was less than those ordered in the prescription record, 24.8% vs 51.9% for paracetamol and 8.3% vs 25.6% for IV morphine (Fig 1). Only four conventional routes; oral, intravenous, intramuscular and subcutaneous, were found in the prescription.
Table 1: Demographic data of pediatric patients
|
Provincial Hospitals |
Regional Hospitals |
Total N=133 N (%) |
||||||
|
KL |
MS |
BR |
SR |
KK |
SG |
NR |
||
| Age (yr) | ||||||||
| <1 Infant |
0 |
0 |
0 |
0 |
7 |
4 |
4 |
15 (11.3) |
| 1-2 Toddler |
2 |
0 |
1 |
3 |
3 |
12 |
8 |
29 (21.8) |
| 3-4 Pre-School |
2 |
2 |
0 |
3 |
2 |
4 |
7 |
20 (15.0) |
| 5-11 School age |
7 |
4 |
11 |
1 |
7 |
4 |
11 |
45 (33.8) |
| 12-15 Adolescent |
2 |
0 |
2 |
3 |
4 |
6 |
7 |
24 (18.1) |
| Gender | ||||||||
| Male |
8 |
3 |
11 |
8 |
13 |
16 |
21 |
80 (60.2) |
| Female |
5 |
3 |
3 |
2 |
10 |
14 |
16 |
53 (39.8) |
| Postoperative day (N=120) | ||||||||
| Day 0 |
0 |
0 |
2 |
2 |
3 |
0 |
3 |
10 (8.3) |
| Day 1 |
2 |
3 |
3 |
0 |
3 |
7 |
8 |
26 (21.7) |
| Day 2 |
4 |
0 |
1 |
1 |
5 |
9 |
5 |
25 (20.8) |
| Day 3 |
0 |
0 |
6 |
1 |
0 |
0 |
1 |
8 (6.7) |
| Day >3 |
7 |
2 |
1 |
6 |
9 |
12 |
14 |
51(42.5) |
| Type of surgery (N=126) | ||||||||
| Minor surgery |
4 |
3 |
7 |
6 |
2 |
16 |
12 |
50 (39.7) |
| Moderate surgery |
9 |
2 |
6 |
6 |
16 |
12 |
15 |
66 (52.4) |
| Major surgery |
0 |
0 |
0 |
0 |
5 |
0 |
5 |
10(7.9) |
Table 2: Severity of pain and patients’ perception of pain treatment
|
|
4xProvincial Hospitals |
3xRegional Hospitals |
Total N (%) |
| Pain in the past 24 h (N = 133) | |||
| No pain |
8 |
33 |
41(30.8) |
| Mild (2) |
12 |
14 |
26(19.6) |
| Moderate (4-6) |
8 |
26 |
34(25.6) |
| Severe (8-10) |
13 |
11 |
24(18.0) |
| NA/ missing |
2 |
6 |
8(6.0) |
| Recent Pain (N = 133) | |||
| No pain |
19 |
54 |
73(54.9) |
| Mild (2) |
14 |
17 |
31(23.3) |
| Moderate (4-6) |
5 |
13 |
18(13.5) |
| Severe (8-10) |
3 |
3 |
6(4.5) |
| NA/ missing |
2 |
3 |
5(3.8) |
| Perception of pain treatment (N = 92) | |||
| Yes |
16 |
25 |
41(44.6) |
| No |
13 |
28 |
41(44.6) |
| Not sure |
3 |
3 |
6(6.5) |
| NA/missing |
3 |
1 |
4(4.3) |
| Non-Pharmacological Used (N = 92) | |||
| Used |
24 |
32 |
56(60.9) |
| Not used |
9 |
20 |
29(31.5) |
| NA/missing |
2 |
5 |
7(7.6) |
Table 3: Proportion of patients experienced moderate to severe pain by postoperative day (N=83)
| Postoperative day |
N(%) |
| Day 0 (N = 7) |
1(14.3) |
| Day 1 (N = 21) |
5(23.8) |
| Day 2 (N = 16) |
4(25.0) |
| Day 3 (N = 5) |
0(0) |
| Day>3 (N = 34) |
12(35.3) |
Table 4: Pain treatment modalities (N =133)
| Treatment modalities |
Provincial Hospitals |
Regional Hospitals |
Total
N(%) |
|||||
| KL | MS | BR | SR | KK | SG | NR | ||
| Pain medications ordered | ||||||||
| Oral paracetamol | 9 | 4 | 9 | 6 | 10 | 10 | 21 | 69(51.9) |
| IV morphine | 6 | 0 | 0 | 1 | 10 | 4 | 13 | 34(25.6) |
| IV fentanyl | 0 | 1 | 0 | 0 | 2 | 3 | 0 | 6(4.5) |
| IV tramadol | 2 | 0 | 2 | 0 | 0 | 0 | 1 | 5(3.8) |
| IM / SC pethidine | 2 | 0 | 0 | 0 | 0 | 0 | 1 | 3(2.3) |
| IV paracetamol | 1 | 0 | 0 | 0 | 3 | 1 | 1 | 6(4.5) |
| Oral ibuprofen | 0 | 0 | 0 | 0 | 1 | 0 | 0 | 1(0.8) |
| Pain medications administration | ||||||||
| IV morphine | 0 | 0 | 0 | 0 | 6 | 1 | 4 | 11(8.3) |
| IV fentanyl | 0 | 0 | 0 | 0 | 1 | 2 | 0 | 3(2.3) |
| IV tramadol | 0 | 0 | 1 | 0 | 0 | 1 | 0 | 2(1.5) |
| IM / SC pethidine | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0(0) |
| IV pethidine | 0 | 0 | 2 | 1 | 0 | 0 | 1 | 4(3.0) |
| Oral paracetamol | 5 | 4 | 6 | 5 | 1 | 3 | 9 | 33(24.8) |
| IV paracetamol | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0(0) |
| Oral ibuprofen | 0 | 0 | 0 | 0 | 0 | 0 | 0 | 0(0) |
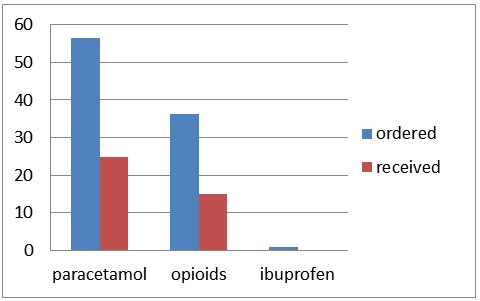
Fig 1: Percent of pain medication compared between ordered and administration in seven hospitals (N = 133)
DISCUSSION
The prevalence of postoperative pain in the present survey was 69.2%. It is difficult to compare pain prevalence of this study with other previous studies because there are some differences in situations or criteria between the surveys. For example, de Moura et al4 reported higher prevalence of pain (91.7%) than the present survey because they focused pain on the first postoperative day and the participants were selected for adenotonsillitis and bone fractures cases which had tendency to have severe pain after surgery7. Bagi et al8 surveyed on general surgical condition as we did in the present study, but they reported higher pain prevalence (93%) because their survey was done during the first 18 hrs after surgery. Similarly, Kozlowski et al9 reported pain prevalence about 86% but the participants in their study were the mixture of medically and surgically treated cases.
In the present study, the prevalence of moderate to severe pain intensity was 43.6%. The low proportion of moderate to severe pain in this study might be associated with the small number of major surgical cases (7.9%). Also, about a half (49.2%) of patients had surgery more than 3 days ago that means their pain intensity was subsided. In addition, age and gender difference may also affect on reporting pain. Female usually reported higher pain intensity than male as same as older children usually reported higher pain scores than the younger9,10. In the present study, the proportion of female was lower than male (39.8% vs 60.2%) but the proportion of participants age below and above 5 years was not different (48.1% vs 51.9%).
The present survey provided evidences about pediatric pain management in the following points: firstly; for the prescription for pain treatment, the most common clinical practices found was oral paracetamol (51.9%), where as prescription for opioid and NSAIDs were only 10.6% and 0.8%. These findings were quite similar with the pevious survey by Karling et al11 who reported that 15% of healthcare professionals never or infrequently used potent opioids. Our previous survey on healthcare professionals’ attitude about opioid usage in children also confirmed that they really concerned about its adverse effects, especially for respiratory depression6. A combination of opioid and NSAIDs or multimodal analgesia which is recommended for improving postoperative pain treatment was not found in the present survey. Secondly; about the routes of analgesic administration, the present results revealed only three conventional methods; oral, intravenous and intramuscular/subcutaneous routes. This suggests that the recommendation of avoiding intramuscular route in children was not well generalized because intramuscular route was still prescribed at least in 2 of 7 participated hospitals. Thirdly; as for the pain medications administration, the frequency of analgesics actually administered to patients was less than the numbers appeared in the prescription. For example, prescription for paracetamol was 51.9% but only 24.8% was administered to the patients. Although such a discrepancy was commonly found in normal practices but the range of the gap should not be so big. Kozlowski et al9 reported that only 27%-50% of the children with an ordered for paracetamol as needed (p.r.n.) received at least one dose of the drug, for more potent analgesic drug like opioids the percentage of administration was lower than paracetamol (10%-33%). Smyth et al12 studied about decision-making of nurses associated with the selection and administration of appropriate analgesia to children, and found that it was very complex. Fourthly; supporting equipment such as patient-controlled pump (PCA pump) was available in the regional hospitals participated in this study, it was not used for children in this survey. Enough numbers of infusion pumps were also supplied but case of usage of opioid infusion technique was not found in this survey as well. Opioid infusion is safe and useful especially for short acting drug like fentanyl; UK national audits verified that the overall incidence of 1:10,000 of serious harm with opioid infusion techniques in children is comparable to the risks with pediatric epidural infusions and central blocks 13. Therefore, infusion technique is an alternative choice for increasesing opioid delivery and improving analgesia in situation that PCA pump is limited and for children that unable to use PCA pump.
The present survey had few weak points; firstly, the number of patients from each hospital was quite different and distribution of patients from each department was unequal leading to have a small number of major cases and lower pain prevalence. These factors were unable to control because it was related to a one day survey. If the survey was done on the day after minor surgery, it was understood that pain intensity in those cases was low; opposite to the major surgery of which pain intensity was much higher. Secondly, situation of health care providers of each hospitals were not recorded, so that the variations in the numbers or disciplines of physicians or experiences of nurses may have some account for different clinical practices.
CONCLUSION
Postoperative pain in children is still undertreated in the hospitals in northeastern Thailand. Raising awareness and improving knowledge for physicians, nurses and other healthcare providers about postoperative pain in children are assumed to be important and needed to be improved.
ACKNOWLEDGEMENTS:
The authors would like to thank all the volunteer research nurses from the hospitals who participated in this survey and the hospital directors who supported it and Professor Yukifumi Nawa for assistance in manuscript preparation. This research was made possible by a Teasdale-Corti Team Grant from the Global Health Research Initiative, administered by the International Development Research Centre (IDRC), Canada.
REFERENCES
- McGrath PJ, Finley GA. Attitudes and beliefs about medication and pain management in children. J Palliative Care 1996;12:46-50. [PubMed]
- 2005-2006 Global years against pain in children. Available online http://www.iasp-pain.org/Advocacy/Content.aspx?ItemNumber=1306. Accessed in Nov 2013.
- Stevens BJ, Abbott LK, Yamada J, Harrison D, Stinson J, Taddio A, et al. Epidemiology and management of painful procedures in children in Canadian hospitals. CMAJ 2011;183:E403-10. [PubMed] [Free Full Text]
- de Moura LA, de Oliveira AC, Pereira Gde A, Pereira LV. Postoperative pain in children: a gender approach. Rev Esc Enferm USP 2011;45:833-8. [PubMed][Free Full Text]
- Charuluxananan S, Thienthong S, Rungreungvanich M, Srirojanakul W, Punjasawadwong Y, Sriprajittichai P. A Survey of Post Anesthetic Pain in Thailand. J Med Assoc Thai 2009;92:1028-32. [PubMed]
- Forgeron PA, Jongudomkarn D, Evans J, Finley GA, Thienthong S, Siripul P, et al. Children’s pain assessment in northeastern Thailand: perspectives of health professionals. Qual Health Res 2009;19;71-81. [PubMed] [Free Full Text
- Dahmani S, Dupont H, Mantz J, Desmonts JM, Keita H. Predictive factors of early morphine requirements in the post-anaesthesia care unit (PACU). Br J Anaesth 2001;87:385-9. [PubMed] [Free Full Text]
- Bagi IA, Ahmed ME. Postoperative pain and analgesic prescription in Khartoum: evaluation of current practice. East Afr Med J 1993;70:502-5. [PubMed]
- Kozlowski LJ, AffiliationsDivision of Pediatric Anesthesiology and Critical Care Medicine, Department of Anesthesiology and Critical Care Medicine, Johns Hopkins University School of Medicine, Baltimore, MarylandAddress correspondence to Lori Kozlowski, RN, MS, CPNP, Department of Anesthesiology and Critical Care Medicine, The Johns Hopkins Charlotte R. Bloomberg Children’s Center, Room 6363, 1800 Orleans Street, Baltimore, Maryland 21287.Kost-Byerly S, Colantuoni E, Thompson CB, Affiliations·Department of Biostatistics, Johns Hopkins Bloomberg School of Public Health, Baltimore, MarylandVasquenza KJ, Rothman SK, et al. Pain prevalence, intensity, assessment and management in a hospitalized pediatric population. Pain Manag Nurs 2014;15:22-35. [PubMed]
- Guinsburg R, de Araújo Peres C, Branco de Almeida MF, de Cássia Xavier Balda R, Cássia Berenguel R, Tonelotto J, et al. Differences in pain expression between male and female newborn infants. Pain 2000;85:127-33. [PubMed]
- Karling M, Renström M, Ljungman G. Acute and postoperative pain in children: a Swedish nationwide survey. Acta Paediatr 2002;91:660-6. [PubMed]
- Smyth W, Toombes J, Usher K. Children’s postoperative pro re nata (PRN) analgesia: nurses’ administration practices. Contemp Nurse 2011;37:160-72. [PubMed]
- Morton NS, Errera A. APA national audit of pediatric opioid infusions. Paediatr Anaesth 2010;20:119-25. [PubMed]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube