
Kjetil Larsen, CES[1]
[1]Corrective exercise specialist, Training & rehabilitation, Oslo (Norway)
Correspondence: Kjetil Larsen, CES, Corrective exercise specialist, Training & rehabilitation, Sandakerveien 22E, 0473 Oslo, (Norway); Phone: +47 975 45 192; E-mail: Kjetil@trainingandrehabilitation.com
ABSTRACT
A 27-year-old woman presented with dominant symptoms including chronic migraine, dizziness and nausea with suspected intracranial hypertension (ICH). The patient also had a purpuric (cyanotic) facial discoloration, suggestive of compromised cerebral perfusion. However, her lumbar puncture opening pressure (LPOP) was borderline high, with 20 cm H2O. There was no evidence of partially empty sella turcica nor obliteration of the cerebral cisterns upon MRI. She was initially diagnosed with chronic migraines by her neurologist. However, closer inspection revealed posterior scleral flattening, flattened pons, and most importantly stenosis of the internal jugular veins (IJV) between the C1 transverse processes and styloid processes, due to anterior subluxation of the atlanto-occipital facets. Doppler waveforms of the internal carotid arteries were abnormal and suggestive of ICH, with a significantly delayed systolic upstroke but with normal speeds. Manual compression of the IJVs reproduced her symptoms within 7 sec. Occult biomechanical ICH may have severe and long-lasting consequences for the patient and thus its detection, and distinguishing from the “common migraine” is necessary, so that the patient may receive proper treatment.
Keywords: Idiopathic intracranial hypertension; Pressure, intracranial; Hypertension, intracranial; Migraine; Dizziness; Craniocervical junction
Citation: Larsen K. Occult intracranial hypertension as a sequela of biomechanical internal jugular vein stenosis: A case report. Anaesth Pain & Intensive Care 2018;22(2):238-242
Received – 30 June 2018, Reviewed – 30 June 2018, Corrected & Accepted –3 July 2018
INTRODUCTION
Because of the many overlapping symptoms between intracranial hypertension (ICH) and migraines, some of these being headache, nausea and/or vomiting, vision impairment, dizziness, vertigo, light sensitivity, etc., the two may be clinically indistinguishable if the initial tests, especially lumbar puncture opening pressure (LPOP) is within reference range, or if there is no evidence of papilledema on fundoscopy.1 In this case report I will discuss the history, examination and conclusions in a 27-year-old woman whose chronic symptoms were compatible with ICH, yet had a negative LPOP as well as normal sella turcica and cerebral cisterns. Ultimately, internal jugular vein stenosis between the C1 transverse process (TP) and styloid process was detected, as well as abnormal carotid Doppler waveforms in the carotid artery, and thus the presence of biomechanically induced ICH (BICH) was demonstrated.
CASE REPORT
A 27-year-old woman presented to my clinic with a history of chronic migraines, dizziness, periodic vertigo, nausea and neck pain. She also felt continuous intracranial pressure, as if her eyes would “pop out”. The patient had been in and out of the hospital in her city of residence for approximately 5 years, due to her chronic symptoms. Her neurologist had tried many types of medications, including opiates and anti-migraine medication with no effect, until they tried acetazolamide (cerebrospinal fluid (CSF) production inhibitor) and furosemide (diuretic) in combination. Taken separately, the two medications had no effect earlier. She was taken off acetazolamide and furosemide, although well-working, during her second pregnancy in 2015, but was not allowed to reintroduce both of them by her neurologist, because they had similar effects.
She was initially diagnosed with chronic migraine in 2013, but because of her continuous feeling of increased intracranial pressure, and because the CSF suppressants and diuretics had positive effect, a lumbar puncture was performed to evaluate her CSF pressure. The examination revealed 20 cmH2O and was thus deemed ~normal, but in the very upper limit (normal range 18-20 cmH2O).2,3 She also sought consultation of a private ophthalmologist, who confirmed that both eyes did have somewhat of a papilledematous appearance. Cerebral MRI was done, but deemed negative, most likely due to the normal appearance of the sella turcica and cerebral cisterns. She then had had an upright MRI examination of her head abroad just a few months prior to visiting my clinic, but its report did not explain her symptoms either, except for a suspicion toward hypermobility syndrome, which had been associated with ICH.4
The patient’s symptoms initially improved post spinal puncture, but then quickly exacerbated. A CSF leak was proven and a blood patch was used to heal the perforated dura. However, a few weeks after the leak healed, her old symptoms returned. Similar sequelae in patients with idiopathic intracranial hypertension (IIH) have also been reported by Holbrook et al.5 This, once again, suggested either venous drainage impairment or CSF hyper-production.
I reviewed her MR images and was able to identify a significant forward subluxation (8.5 mm) of the C1 facets in relation to the occipital condyles and that it was obstructing both internal jugular veins (IJVs), by measuring the C1 transverse processes (TPs) in relation to the bimastoid line.6 This stenotic occurrence has also been documented by others.7–10 There was also flattening of the posterior sclera and the pons, as well as slight distention of the optic nerve sheaths, which are common imaging findings of ICH.2,5 However, the appearance of the sella turcica and the cerebral cisterns were normal. Compatible with this, the patient had very rigid and saturated carotid arteries upon palpation, and a Doppler ultrasound examination showed that there were normal speeds but abnormal waveforms, with delay of the systolic upstroke indicating distal resistance with compromised cerebral perfusion secondary to ICH.11 The palpable rigidity and saturation as well as Doppler findings were present bilaterally.
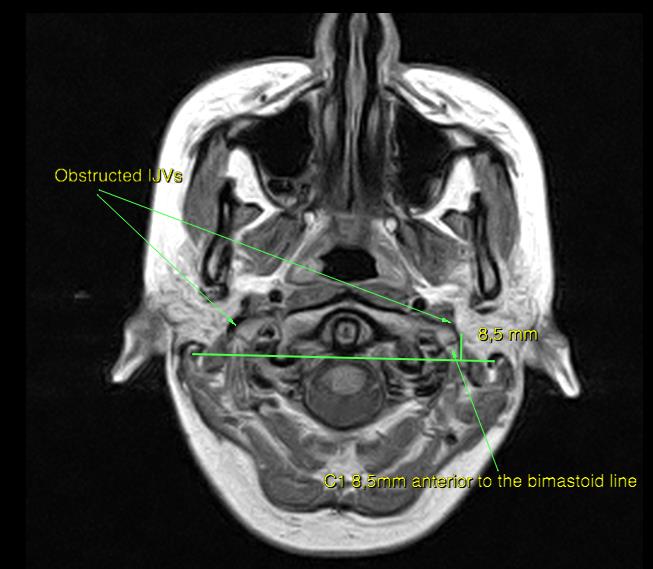
Figure 1: MRI PD, axial slice
The atlas has subluxed 8.5 mm forward, evident by comparing its TPs in relation to the bimastoid line.6 The atlas now blocks the jugular foramen as well as the internal jugular veins.
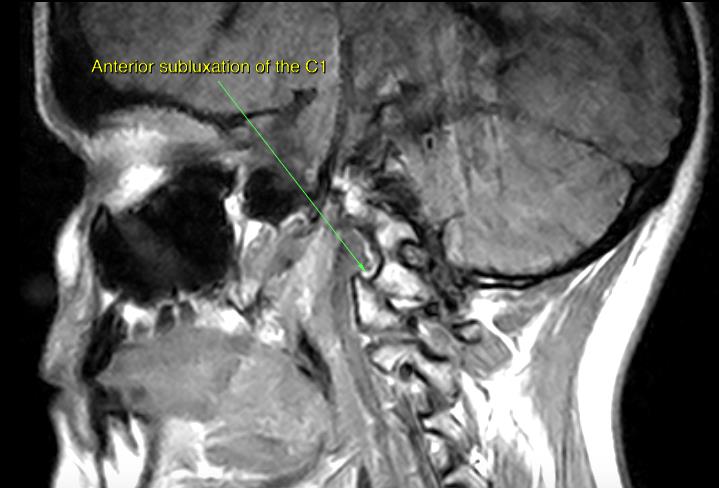
Figure 2: MRI T1, sagittal slice
Sagittal view of the facet joint subluxation. Similar problems
at the atlantoaxial (AA) joints have been documented by
Atul Goel.12

Figure 3: MRI PD, axial
There is evidence of flattened posterior globes and slight optic
nerve sheath distention, which is often seen in patients with
increased intracranial pressure (ICP).2,5

Figure 4: MRI T1, sagittal
There is a flattened presentation of the pons, which is often seen
in patients with increased ICP.2,5
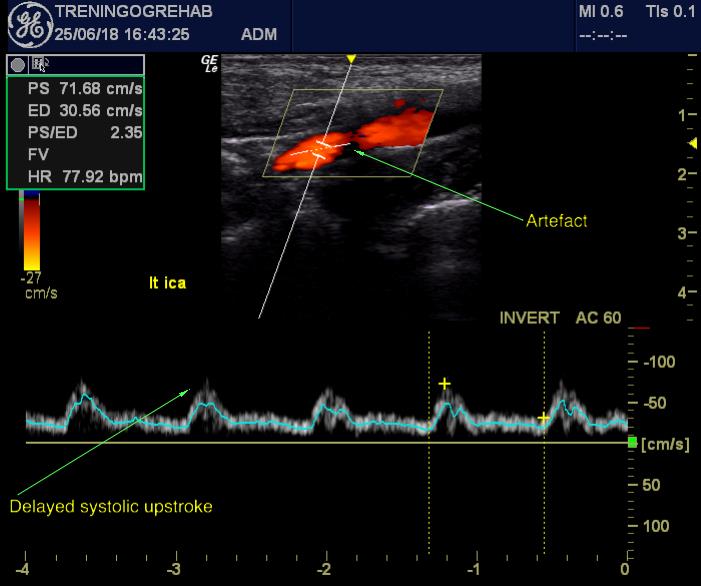 Figure 5: Doppler – Internal carotid artery, distal
Figure 5: Doppler – Internal carotid artery, distal
Doppler examination of the ICAs revealed normal speeds, but
abnormal waveforms. There is a delayed systolic upstroke with
an imbalanced P1-2 presentation, where the P2 is dominant,
indicative of ICH.11
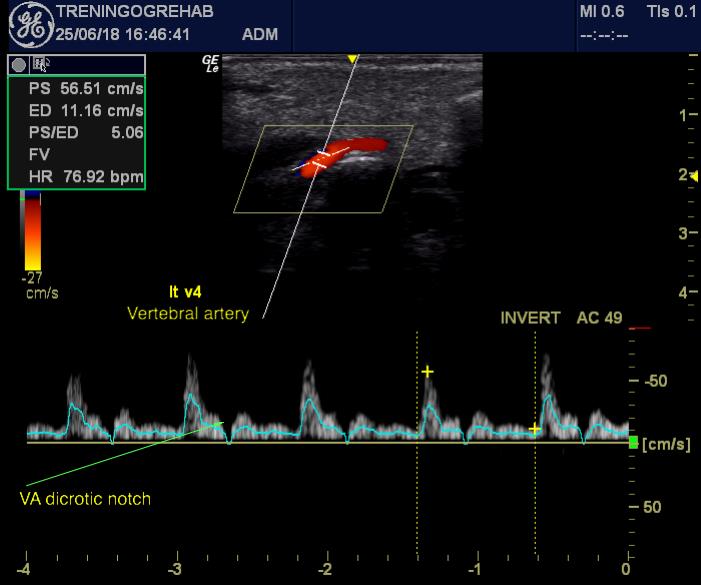
Figure 6: Doppler – vertebral artery, segment V4
There was also presence of a vertebral artery dicrotic notch at
the early diastole, which may possibly be interpreted as
further evidence of vessel saturation. The slightly
elevated systolic peak is relatively normal at the V4 segment. It
has, however, been suggested that dicrotic notch evaluation of
the carotid arteries may be helpful when assessing stiffness of
the vessels.13
Further physical examination:
Upon examination, the patient initially presented with a conspicuous purpuric head and neck discoloration which was absent elsewhere on the body. Based on her clinical history and MR images, this suggested mild cyanosis due to poor cerebral perfusion. There was also an obvious distention of the external jugular veins (EJV) when lying supine, suggesting excess secondary venous drainage, which has also been documented in both ICH and migraine patients.14–15 I was able to quickly and significantly worsen her migraine, from 4 to 8 on the numeric rating scale (NRS), and perceived ICP as well as facial discoloration within 7 sec of manual compression of the IJVs (Queckenstedt’s maneuver).16 Anecdotally, in controls, manual compression of the IJVs may take up to 20 sec before significant ICP perceptions occur, but without concomitant pain (personal experience with BICH patients).
The patient also presented with poor cervical posture and depressed scapulae. We set her into a trial posture where she gently flexed her head and neck (cf. the above-mentioned), as well as raised the shoulders to decompress the subclavian arteries (Cyriax test). Within 2 min her purpuric facial discoloration vanished, and the chronic migraine reduced from 8 on the NRS scale to 3. The palpable carotid artery rigidity and dilation also normalized in “good” posture (the latter when lying supine). As an additional provocative trial, I had her do body weight squats in ‘good’ and ‘bad’ postures, to see if increased heart rate and poor posture exacerbated her migraine and dizziness. In ‘bad posture’, I led her hinge back for craniocervical extension, to further compromise the IJVs, as well as pulled her shoulders back and down, to compress the subclavian arteries. In ‘good posture’, I had her raise her clavicle rostrocranially and go into craniocervical flexion. Results: she could perform eight easy repetitions with just very mild dizziness and no pain exacerbation (we stopped due to lack of symptoms), but only 0,5 repetitions (failed due to severe dizziness and nearly syncope) in ‘bad posture’. Again, the results were clearly compatible with BICH.
The patient was sent home with postural corrective measures to raise her shoulders and to improve her neck posture (i.e. to stop hinging back at the neck, but rather be “long” in the neck)6,19,20 to decompress the SA and IJV, as well as with strengthening exercises for the deep neck flexors, extensors and scapular elevators6 to ameliorate the atlantal displacement. She was also recommended to have another talk with her neurologist about reintroducing acetazolamide and furosemide as a temporary intervention during the ongoing conservative intervention.
DISCUSSION
This patient presented with typical symptoms of chronic idiopathic ICH. She responded to CSF suppressants and diuretics in combination. Had conspicuously blocked IJVs as well as a flattened pons, flattened posterior sclera and optic sheath distention upon MRI. Abnormal ICA waveforms upon Doppler ultrasound examination. And, nonetheless, papilledema verified by an ophthalmologist. On the top of it all, I was able to precisely reproduce her symptoms in mere seconds with manual compression of the IJVs, as well as with the GP/BP maneuver for BICH. All of this cumulative evidence supports a diagnosis of BICH.
However, the sella turcica and cerebral cisterns appear normal (also imaging criteria for IIH,2,5 and the LPOP was in the very upper limit of the reference range. LPOP has been shown to sometimes be negative in ICH patients, and some of these authors recommend that there is performed another lumbar puncture examination 24 hours later, if the patient’s symptoms and the LPOP do not harmonize.21–22 Suh21 also describes two cases where there were conspicuous symptoms of IIH, such as evidence of optic disc swelling (papilledema), yet normal lumbar puncture opening pressures, sella turcica, scleral appearance and venous diameters. Both patients responded to Diamox, 250 mg and 500 mg twice per day. Holbrook5 also reported a case of intracranial hypertension who incurred hypotension post lumbar puncture due to CSF leakage. After resolving the leak, her chronic headache was proven to return at just 19 cmH2O. Digre states that [occult] IIH patients without papilledema may have lower ICP, and thus they propose =>20 cmH2O as the upper limit,23 as does Osborn.2 Opening pressures above 20 cmH2O were closely associated with venous stenosis.24 Thus, the diagnosis of ICH is not as black and white as it may be portrayed by the negative LP.
A common cause of BICH is depressed scapulae and hinge-neck posture, especially in combination. This may significantly elevate ICP due to positional obstruction of both the subclavian artery and internal jugular vein. Postural correctives for the neck and elevation of the clavicles may ameliorate this problem. Poor cervical posture, especially upper cervical extension (“hinge neck”) may lead to greater obstruction of the IJVs, as they wrap around the TPs of the C16,17 when the jugular foramen moves posteriorly in relation to the C1. This may impair cerebral perfusion and thus lead to BICH. The patient may be more susceptible to this problem if the atlas has subluxed forward, because the atlantostyloid interval (ASI) will be narrow to begin with. Depression of the scapulae may lead to compression of the costoclavicular space, and thus obstruct the distal subclavian artery (SA).18–19 The distal SA obstruction will redirect more blood into the cranium, which is quite unfortunate if the IJVs are blocked from poor posture and/or anterior subluxation of the C1, resulting in a significant imbalance between arterial inlet volume and venous drainage, with subsequent BICH.
Conversely, pulling the shoulders ‘back and down’ as a postural corrective may brutally exacerbate the symptoms of a patient with BICH, as it may cause compression of the SA,18,19 and is thus strongly discouraged. Further, forward subluxation of the C1 may also obstruct the IJV and jugular foramen, as seen in this case study. In my experience, forward subluxation of the atlas is a common occurrence in these patients. Identification of ICH is important, due to its potentially serious implications.25
CONCLUSION
Intracranial hypertension may easily be misdiagnosed as commonly occurring migraine, based on their similar symptoms. If the most common tests and presentations of ICH are normal, such as lumbar puncture opening pressure, papilledema and sella turcica content, one could mistakenly reject ICH as the suspected etiology. However, there have been several reports of ICH despite normal conventional imaging and lumbar puncture findings. Identification of ICH is important, due to its potentially serious implications. This case report demonstrates how biomechanical factors may lead to occult ICH.
Conflict of interest: None declared by the author
REFERENCES
- Mathew NT, Ravishankar K, Sanin LC. Co-existence of migraine and idiopathic intracranial hypertension without papilledema. Neurology. 1996;46:1226–30. doi: 10.1212/WNL.46.5.1226. [PubMed]
- Osborn AG, Hedlund G, Salzman KL.Osborn’s Brain. 2nd edition. Elsevier;2017.
- Agamanolis, PD. Neuropathology Chapter 14: Cerebrospinal fluid. Accessed on:30th June, 2018. Available at: http://neuropathology-web.org/chapter14/chapter14CSF.html
- Henderson FC, Austin C, Benzel E, Bolognese P, Ellenbogen R, Francomano CA, et al. Neurological and spinal manifestations of the Ehlers–Danlos syndromes. Am J Med Genet C Semin Med Genet. 2017 Mar;175(1):195-211. [PubMed] doi: 10.1002/ajmg.c.31549.
- Holbrook J, Saindane AM. Imaging of Intracranial Pressure Disorders. Neurosurgery.2017;80(3):341–354. [PubMed] [Free Full Text] doi: 10.1227/NEU.0000000000001362.
- Larsen K. Atlas joint instability: causes, consequences and solutions. Accessed on: 2018 June 27. Available at: https://treningogrehab.no/atlas-joint-instability-causes-consequences-solutions/.
- Dashti SR, Nakaji P, Hu YC, Frei DF, Abla AA, Yao T, et al. Styloidogenic jugular venous compression syndrome: diagnosis and treatment: case report. Neurosurgery. 2012 Mar;70(3):E795-9. [PubMed] doi: 10.1227/NEU.0b013e3182333859.
- Gweon HM, Chung T, Suh SH. Evaluation of the cause of internal jugular vein obstruction on head and neck contrast enhanced 3D MR angiography using contrast enhanced computed tomography. J Korean Soc Magn Reson Med. 2011 Apr;15(1):41-47. [Free Full Text]
- Higgins N, Trivedi R, Greenwood R, Pickard J. Brain slump caused by jugular venous stenoses treated by stenting: a hypothesis to link spontaneous intracranial hypotension with idiopathic intracranial hypertension. J Neurol Surg Rep. 2015 Jul;76(1):e188–e193. [PubMed] [Free Full Text] doi: 10.1055/s-0035-1555015
- Seoane E, Rhoton AL Jr. Compression of the internal jugular vein by the transverse process of the atlas as the cause of cerebellar hemorrhage after supratentorial craniotomy. Surg Neurol. 1999 May;51(5):500-5. [PubMed]
- Rodríguez-Boto G, Rivero-Garvía M, Gutiérrez-González R, Márquez-Rivas J. Basic concepts about brain pathophysiology and intracranial pressure monitoring. Neurologia. 2015;30(1):16-22. [PubMed] doi: 10.1016/j.nrl.2012.09.002.
- Goel A. Posterior atlantoaxial ‘facetal’ instability associated with cervical spondylotic disease. J Craniovertebr Junction Spine. 2015 Apr-Jun;6(2):51-5. [PubMed] [Free Full Text] doi: 10.4103/0974-8237.156039.
- Hermeling E, Hoeks AP, Winkens MH, Waltenberger JL, Reneman RS, Kroon AA, et al. Noninvasive assessment of arterial stiffness should discriminate between systolic and diastolic pressure ranges. Hypertension. 2010;55:124-30. [PubMed] [Free Full Text] doi: 10.1161/HYPERTENSIONAHA.109.143867
- Alperin N, Lee SH, Mazda M, Hushek SG, Roitberg B, Goddwin J, et al. Evidence for the importance of extracranial venous flow in patients with idiopathic intracranial hypertension (IIH). Acta Neurochir Suppl. 2005;95:129-32. [PubMed]
- Koerte IK, Schankin CJ, Immler S, Lee S, Laubender RP, Grosse C, et al. Altered cerebrovenous drainage in patients with migraine as assessed by phase-contrast magnetic resonance imaging. Invest Radiol. 2011 Jul;46(7):434-40. [PubMed] doi: 10.1097/RLI.0b013e318210ecf5.
- Chou CH, Chao AC, Lu SR, Hu HH, Wang SJ. Cephalic venous congestion aggravates only migraine-type headaches. Cephalalgia. 2004;24:973–9. [PubMed]
- Flanagan MF. The role of the craniocervical junction in craniospinal hydrodynamics and neurodegenerative conditions. Neurol Res Int. 2015;2015:794829. [PubMed] [Free Full Text] doi:10.1155/2015/794829.
- Larsen K. Postural cues for scapular retraction and depression promote costoclavicular space compression and thoracic outlet syndrome. Anaesth Pain & Intensive Care 2018;22(2):256-267
- Magee DJ. Orthopedic physical assessment. 6th edition. Saunders; 2013.
- Osar, E. Corrective exercise solution to common hip and shoulder dysfunction. 1st edition. Lotus Pub; 2012.
- Suh SY, Kim SJ. IIH with normal CSF pressures? Indian J Ophthalmol. 2013 Nov;61(11):681–2. [PubMed] [Free Full Text] doi: 10.4103/0301-4738.119416
- Friedman DI, Jacobson DM. Diagnostic criteria for idiopathic intracranial hypertension. Neurology. 2002 Nov 26;59(10):1492-5. [PubMed]
- Digre KB. Not so benign intracranial hypertension. BMJ. 2003;326:613–4. [PubMed] [Free Full Text]
- Bono F, Salvino D, Tallarico T, Cristiano D, Condino F, Fera F, et al. Abnormal pressure waves in headache sufferers with bilateral transverse sinus stenosis. Cephalalgia. 2010;30:1419–25. [PubMed] doi: 10.1177/0333102410370877.
- Corbett JJ, Savino PJ, Thompson HS. Visual loss in pseudotumor cerebri. Follow-up of 57 patients from five to 41 years and a profile of 14 patients with permanent severe visual loss. Arch Neurol. 1982;39:461–74 [PubMed]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube