
Jadoon H, Khan TH, Ahmed F, Tasneem S. Malignant hyperthermia: survival without dantrolene – a case report.
Humaira Jadoon, FCPS*, Tariq Hayat Khan, MCPS, FCPS**, Fida Ahmed, MCPS*, Shahida Tasneem, DA, MCPS*
*Consultant Anesthesiologist; **Consultant Anesthesiologist & Pain Specialist
Department of Anesthesiology & Pain Management, KRL General Hospital, G-9/1, Islamabad (Pakistan)
Correspondence: Dr. Humaira Jadoon, FCPS, Department of Anesthesiology & Pain Management, KRL General Hospital, G-9/1, Mauve Area, Islamabad (Pakistan); E-mail: drhumairajadoon@gmail.com
ABSTRACT
We encountered a case of malignant hyperthermia in a 52 year old male undergoing open reduction/internal fixation of humerus fracture under general anesthesia. Isoflurane has been reported as a potent triggering agent of malignant hyperthermia. Dantrolene remains the gold standard for treating this life threatening syndrome but it is not available in many countries including Pakistan. However, we successfully managed our patient by timely recognition of this syndrome and administering prompt and effective symptomatic treatment.
Key words: Malignant hyperthermia; Dantrolene
Citation: Jadoon H, Khan TH, Ahmed F, Tasneem S. Malignant hyperthermia: survival without dantrolene – a case report. Anaesth Pain & Intensive Care 2016;20(2):236-239
Received: 24 May 2016; Reviewed: 26 May 2016; Corrected: 6 June 2016; Accepted: 15 June 2016
INTRODUCTION
Malignant hyperthermia is a hypermetabolic syndrome characterized by hyperthermia, hypercarbia, acidosis, tachycardia, muscle rigidity and rhabdomyolysis. The syndrome is triggered in susceptible individuals by potent inhalation agents, succinylcholine, vigorous exercise and heat. We encountered a case of malignant hyperthermia in adult patient in whom the only MH triggering agent administered was isoflurane. Dantrolene was not available but the patient was successfully managed without any residual morbidity by timely recognition and prompt intervention and aggressive management.
CASE REPORT
A 52 years old male patient, 80 kg, thick muscular build, was scheduled for open reduction/internal fixation of left humerus fracture. Patient had had no general anesthesia previously. There was no family history of problems with anesthesia and some of his family members had successfully undergone surgery under general anesthesia without any complication. Neither the patient nor his family members had history of neuromuscular disease. His preoperative medical history was insignificant except hypertension that was well controlled with tablet amlodipine 10 mg once daily. His preoperative physical, airway and laboratory examination were within normal limits.
On the day of surgery patient received his usual morning dose of antihypertensive with a sip of water. His preoperative vital signs were heart rate: 84 beats/min, blood pressure: 140/90 mmHg, respiratory rate: 16/min and axillary temperature: 98 °F.
Patient was given pre-induction by midazolam 2 mg, nalbuphine 6 mg and ondansetron 4 mg before induction with etomidate 20 mg and atracurium 30 mg. An attempt at inserting i-gel size 4 failed sue to poor mouth opening. Anesthesia was deepened with 5% isoflurane in O2 and N2O and i-gel was inserted with the help of assistant. Brachial plexus block was done by interscalene approach with 0.125 % ropivacaine 20 ml for postop analgesia, and anesthesia maintained with oxygen, nitrous oxide and isoflurane. Patient was placed in right lateral position and surgery started. Soon after start of surgery patients EtCO2 increased from 40 mmHg to 57 mmHg while SpO2 remained stable. Patient was hyperventilated manually with 100 % oxygen to lower raised EtCO2, and suspecting leakage of the gases due to a smaller sized i-gel, it was replaced with i-gel No. 5 with difficulty. During this attempt patient rapidly desaturated and EtCO2 increased to 80 mmHg. Help was called, the patient was immediately put in supine position, jaw opened with difficulty and ETT size 8 passed with the help of a bougie. EtCO2 and heart rate increased to 100 mmHg and 130 beats/min respectively. Chest remained clear and airway pressures were normal. Oral temperature was checked and found to be 104.5○ F. On examining the limbs, a generalized muscular rigidity was observed with inability to flex the limbs. Diagnosis of malignant hyperthermia was made. Isoflurane discontinued, another anesthesia machine without any vaporizers and with open circuit was rolled in and attached to the patient to manually ventilate him with 100% oxygen 10 L/min using Bain’s circuit. Ringer lactate infusion stopped and patient was hydrated with normal saline.

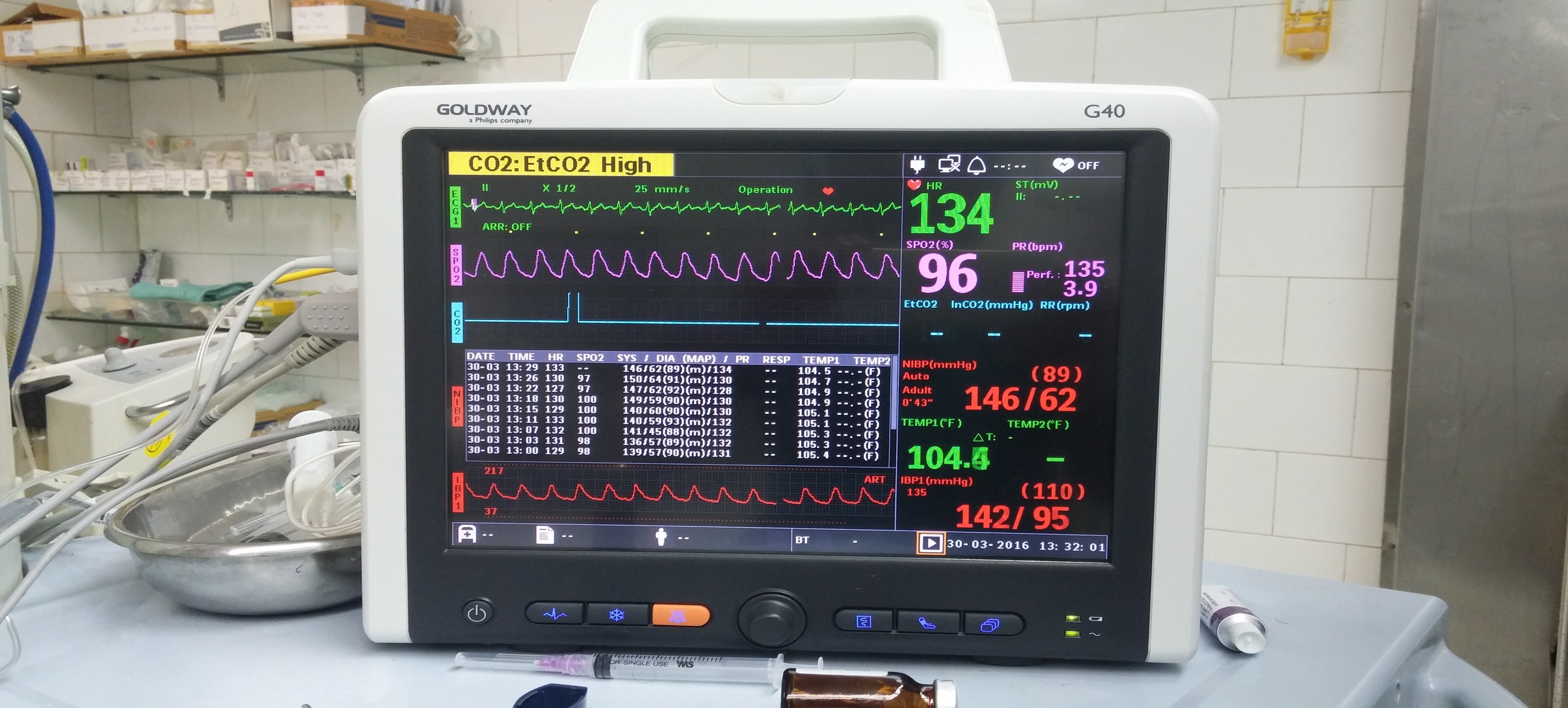
Anesthesia was maintained using propofol and surgeon was asked to close the wound promptly. Continuous temperature monitoring started using nasopharyngeal temperature probe. The maximum temperature recorded was 107.5○ F (Picture 1).
Picture 1: Shows a part of vital signs monitored midway between active resuscitation. EtCO2 is higher than 100 mmHg so the monitor shows only ‘CO2: EtCO2 High’
Urinary catheter was inserted to check urine output. Invasive arterial and central venous pressure monitoring commenced. Peripheral cooling instituted using ice cold water sponging, cooling fans and ice packs. Patient was cooled down centrally using ice cold saline for intravenous infusion, and gastric and urinary bladder lavage. Arterial blood gases revealed pH 7.003, PaCO2 100 mmHg, PaO2 112.5 mmHg, and base excess –6.3 mmol/L. Serum K+ was 5.8 mEq/L while serum Na+ was 140 mEq/L. Inj sodium bicarbonate 40 mEq was given intravenously along with infusion of 25% dextrose water 100 ml plus regular insulin 10 IU to lower raised hyperkalemia. Blood sugar was checked half hourly and was found to be within normal limits. He was given injection frusemide 40 mg and urine output was maintained greater than 100 ml/hr in operating room. Blood pressure and heart rate were controlled with labetolol. Later on patient became hypotensive for which noradrenaline infusion was started along with intravenous fluids. A countrywide search for availability of dantrolene in all major medical institutions was made with negative results.
Patient was shifted to intensive care on ventilatory support. His vitals remained stable in the ICU. He was extubated the next morning. His serum creatinine was increased to 2.0 mg/dl. Rest of the laboratory workup was normal. There was no active complaint by the patient except muscle rigidity and body aches. His creatinine phosphokinase levels are shown in Table 1.
Table 1: Creatinine phosphokinase (CPK) levels of patient
| Time period | CPK ( IU/L) |
| 0 postop day – 12 pm | 2170 |
| 0 postop day – 10 pm | 14395 |
| 1st postop day – 10 am | 17689 |
| 1st postop day – 10 pm | 15830 |
| 2nd postop day | 13243 |
| 3rd postop day | 7448 |
| 4th postop day | 5497 |
| 5th postop day | 2442 |
| 6th postop day | 1573 |
| 7th postop day | 364 |
To avoid rhabdomyolysis associated renal injury he received volume loading, diuretics, and forced alkaline diuresis. By 2nd postop day, the patient’s renal function tests normalized, and his neurological examination did not reveal any detectable derangement. He was rescheduled for surgery a week after stabilization. Surgery was done employing total intravenous anesthesia. Anesthesia remained uneventful and he was discharged home on 3rd postop day. Patient and his family were counseled about malignant hyperthermia before discharge.
DISCUSSION
Malignant hyperthermia is a hypermetabolic syndrome characterized by hyperthermia, hypercarbia, increased oxygen consumption, acidosis, tachycardia, tachypnea, rigidity and rhabdomyolysis. We made diagnosis of malignant hyperthermia on the basis of clinical features. According to the clinical grading scale developed by Larach et al for diagnosis of malignant hyperthermia our patient’s MH score was 73 and MH rank was 6, which meant that the likelihood of malignant hyperthermia was almost certain1 (Table 2 & 3). The possibilities of neuroleptic malignant syndrome and serotonin syndrome were excluded, as patient was not on any neuroleptic or antidepressant drugs. Pheochromocytoma and thyrotoxic crises were less likely as they are not associated with muscle rigidity. Moreover, degree of CO2 production and metabolic acidosis is much lower in these disorders.2
The syndrome occurs upon exposure to potent inhalation agent, succinylcholine, vigorous exercise or heat. The agents administered for induction and maintenance of anesthesia in our case included etomidate, atracurium, nitrous oxide and isoflurane. Isoflurane has been reported to be one of the potent triggering agents of malignant hyperthermia.3
Table 2: Clinical indicators for calculating MH Raw score in the present case1
| Process | Indicators | Points |
| 1. Rigidity
|
Generalized muscular rigidity | 15 |
| 2. Muscle breakdown | Elevated CK> 10,000 iu after anesthetic without succinylcholine | 15 |
| 3. Respiratory acidosis | Arterial PaCO2 >60 mmHg with appropriately controlled ventilation | 15 |
| 4. Temperature increase | Inappropriately rapid increase in temperature (in anesthesiologists judgment) | 15 |
| 5. Cardiac involvement | Inappropriate sinus tachycardia | 3 |
| 6. Other indicators that are not part of a single process |
Arterial pH < 7.25 |
10 |
Table 3: Clinical significance of MH Raw score and its rank1
| Raw score | MH Rank | Description of likelihood |
| 0 | 1 | Almost never |
| 3-9 | 2 | Unlikely |
| 10-19 | 3 | Somewhat less than likely |
| 20-34 | 4 | Somewhat greater than likely |
| 35-49 | 5 | Very likely |
| 50+ | 6 | Almost certain |
Patients who are susceptible to malignant hyperthermia may have neuromuscular disorders.4,5 A positive family history of malignant hyperthermia in a first-degree relative is a strong indicator of MH susceptibility. Our patient had no neuromuscular disease and his family members had successfully undergone surgeries under general anesthesia.
Management of malignant hyperthermia syndrome requires early detection and prompt intervention. Dantrolene is the drug of choice for reversing malignant hyperthermia syndrome. Dantrolene inhibits the release of calcium from sarcoplasmic reticulum by binding to the ryanodine receptors, thereby halting the uncontrolled muscle contractions.6 The mortality rate from MH was reduced from 80% to less than 10% following the development of dantrolene.7 Dantrolene is not available in Pakistan but we were able to rescue our patient with prompt diagnosis and quick aggressive supportive measures with the help of a trained professional team. We came across only one case report of malignant hyperthermia published from Pakistan that was diagnosed clinically and the patient died, as dantrolene was not available.8
Patients recovering from malignant hyperthermia may develop complications as a consequence of hyperthermia and excessive muscle breakdown. Many complications are recorded, the most common being the neurological, cardiac dysfunctions, pulmonary edema, disseminated intravascular coagulation, renal and hepatic dysfunctions.9 Our patient developed renal dysfunction due to acute rhabdomyolysis that responded well to aggressive hydration, forced alkaline diuresis and diuretics. As myoglobinemia due to excessive muscle destruction increases the risk of kidney injury, urine output should be maintained greater than 2 ml/kg/hr.10 CK levels were monitored as a guide to the status of muscle destruction.
Caffeine halothane contracture test (CHCT) is considered gold standard for diagnosis of malignant hyperthermia. Since facility of this test is not available in Pakistan so we could not definitely diagnose malignant hyperthermia in our patient and we relied on clinical grading scale developed by Larach et al.1 Correlation between CHCT and this clinical grading scale has been studied and it is found that high MH scores5,6 are significantly correlated to CHCT.11 Successful surgery of our patient later on with MH non-triggering general anesthesia reaffirmed that diagnosis of malignant hyperthermia was pertinent.
We strongly endorse the use of end tidal CO2 and temperature monitoring during anesthesia as hypercarbia and rapidly increasing temperature are the most common clinical signs of acute malignant hyperthermia.12 Early detection and aggressive supportive management can save the patient without major complications.
The gold standard for treating malignant hyperthermia remains the dantrolene. Other calcium channel blockers like procainamide have been studied but they are found to be ineffective in halting the syndrome.12 Dantrolene is not marketed in Pakistan currently. Although malignant hyperthermia is a rare disorder but as its consequences are grave and mortality is very high in the absence of dantrolene, it must be made available so that no patient die because of its non-availability.
Conflict of interest: None declared by the authors
Author responsibility: All authors took part in the case management; HJ-Manuscript preparation; THK-Editing
REFERENCES
- Larach MG, Localio AR, Allen GC, Denborough MA, Ellis FR, Gronert GA, et al.A clinical grading scale to predict malignant hyperthermia susceptibility. Anesthesiology. 1994;80:771-9. [PubMed] [Free full text]
- Rosenberg H, Brandom BW, Sambuughin N. Malignant hyperthermia and other inherited disorders. In: Barash PG, Cullen BF, Stoelting RK, Cahalan MK, Stock MC, editors. Clinical Anesthesia. 2nd Philadelphia: Lippincott Williams & Wilkins; 2009. p. 598-621.
- McGuire N, Easy WR. Malignant hyperthermia during isoflurane anaesthesia. Anaesthesia. 1990 Feb;45(2):124–127.[PubMed]
- Klingler W, Rueffert H, Lehmann-Horn F, Girard T, Hopkins PM. Core myopathies and risk of malignant hyperthermia. Anesth Analg. 2009;109:1167–73. doi:10.1213/ANE.0b013e3181b5ae2d. [PubMed]
- Benca J, Hogan K. Malignant hyperthermia, coexisting disorders, and enzymopathies: risks and management options. Anesth Analg. 2009; 109:1049–53. doi: 10.1213/ane.0b013e3181adca28. [PubMed]
- Zhao F, Li P, Chen SR, Louis CF, Fruen BR. Dantrolene inhibition of ryanodine receptor Ca2+ release channels: Molecular mechanism and isoform selectivity. J Biol Chem. 2001;276:13810-6. [PubMed] [Free full text]
- Rosenberg H, Fletcher JE. An update on the malignant hyperthermia syndrome. 1994 Nov;23(6 Suppl):84-97. [PubMed]
- Nasir KK, Zafar AB, Mansoor F, Mushtaq S, Ahmad J, Khan IM. Malignant hyperthermia. J Coll Phys Surg Pak. 2004;14:39-40.
- Larach MG, Gronert GA, Allen GC, Brandom BW, Lehman EB. Clinical presentation, treatment and complications of malignant hyperthermia in North America from 1987 to 2006. Anesth Analg. 2010;110:498-507. [PubMed]
- Bosch X, Poch E, Grau JM. Rhabdomyolysis and acute kidney injury. N Engl J Med. 2009;361:62–72. [PubMed] [Free full text]
- Studo RT, Cunha LB, Carmo PL, Matos AR, Trachez MM, Cardoso LA, et al. Use of the caffeine halothane contracture test for the diagnosis of malignant hyperthermia in Brazil. Braz J Med Biol Res. 2010;43:549-56. [PubMed] [Free full text]
- Nelson P, Litman RS. Malignant hyperthermia in children: an analysis of the North American malignant hyperthermia registry. Anesth Analg. 2014;118:369-74. doi: 10.1213/ANE.0b013e3182a8fad0. [PubMed]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube