
Kiran Jangra, MD*, Sandeep Kataria, MD**, Surender K. Malhotra, MD***
*Senior Resident, **Assistant Professor, ***Professor
Department of Anesthesiology & Intensive Care, Postgraduate Institute of Medical Education and Research, Chandigarh-160012 (India)
Correspondence: Prof. Surender K. Malhotra, Department of Anesthesiology & Intensive Care, PGIMER, Chandigarh-160012 (India); Phone: 0091-9814435137; Fax: 0091-172-2744401; E-mail: drskmalhotra@yahoo.com
Key Words: Tracheal tube, Intubation depth mark, obstruction
Citation: Jangra K, Kataria S, Malhotra SK. Intubation depth mark on pediatric tracheal tube: A potential threat for an airway obstruction. Anaesth Pain & Intensive Care 2013;17(3):—
Tracheal tube (TT) obstruction during anesthesia and in intensive care units is not uncommon. One of the various causes of TT obstruction is foreign body inside the tube. This foreign body may be in the form of a tube plastic material1 or some manufacturing defect.2 That is the rationale why TT is made of transparent material and its visual inspection is recommended before use. Despite the recommended practice of visual inspection and testing of TTs for any manufacturing defects, some potential causes of airway obstruction may still go unnoticed.3,4
In this communication, we draw attention to a drawback in the design of a pediatric TT (Mallinckrodt, St. Louis, USA) because of which a foreign body at the distal end may go unnoticed, leading to its possible obstruction. In this particular TT, intubation depth mark provided in black color to aid positioning in relation to the vocal cords and accurate placement, is entirely opaque (Arrow A, Fig 1). This will obscure the view of any intraluminal foreign body by simple external visual inspection. Majority of tracheal tubes by other manufacturers provide intubation depth marks in the form of single or double line marks instead of entire opaque painting (Arrow B, Fig 1). The opaque length of this tube should just cross the glottis to place TT at correct depth. If any foreign body is present intraluminally in this portion, it will not be apparent on external visual inspection due to total opacity.
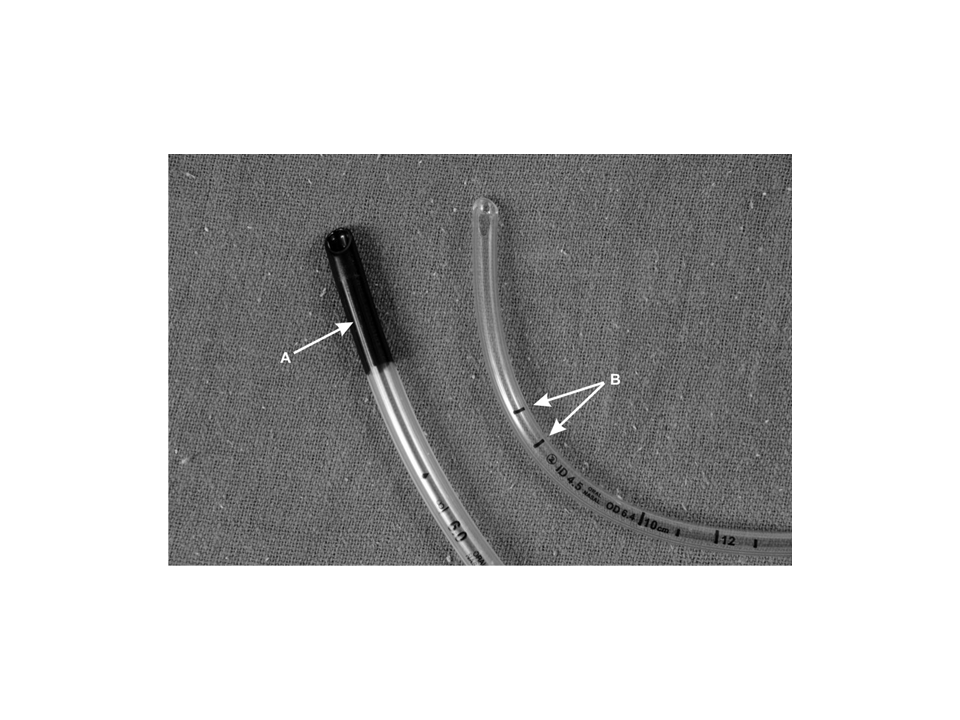
Figure1: Two types of Intubation depth marks on pediatric tubes
As a part of routine preoperative checking of anesthesia equipment, the TT should be checked for patency of the lumen in addition to pilot balloon cuff assembly.
We suggest that TT with opaque black intubation depth mark should be visually inspected before use from the bevel end too.
REFERENCES
- Barst S, Yossefy Y, Lebowitz P. An unusual cause of airway obstruction. Anesth Analg 1994;78:190-199. [PubMed]
- Henderson MA. Airway obstruction with a cuffed single-use plastic endotracheal tube. Anaesth Intensive Care 1993;21:370-372. [PubMed]
- Gettelman TA, Morris GN. Endotracheal tube failure: undetected by routine testing. Anesth Analg 1995;81:1313 [PubMed]
- Khalid S. and Kariman E. Endotracheal tube defects: Hidden causes of airway obstruction. Saudi J Anaesth 2010;4(2):108–110. [PubMed] [Full free text] doi: 10.4103/1658-354X.65123.



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube