
Habib Md Reazaul Karim, MBBS, MD, DNB, IDCCM
Department of Anesthesiology, Critical Care and Pain Medicine. NEIGRIHMS, Shillong-793018 (India)
Correspondence: Department of Anesthesiology, Critical Care and Pain Medicine, North Eastern Indira Gandhi Regional Institute of Health & Medical Sciences (NEIGRIHMS), Mawdiangdiang, Shillong, Meghalaya 793018, (India); Phone: +919612372585 (M); E-mail: drhabibkarim@gmail.com
ABSTRACT
Preoperative consultation of surgical patient by cardiologist is intended to treat an inadequately treated cardiac condition before undergoing surgery. This can yield in terms of new therapy, lead to optimization of the patients’ cardiac comorbidity, impact significantly in terms of perioperative management and potentially reduce postoperative adverse cardiac events. However, judicious use of preoperative consultation request is required both for avoiding unnecessary consultation, investigation and delay in proceeding with surgery as well as cost effective health care delivery. This mini review is aimed at finding the practice patterns of anesthesiologists’ preoperative requests for cardiology consultations. Different clinical situations faced in preoperative evaluation of cardiac patients planned for non-cardiac surgery with regard to the need for preoperative cardiac consultation and a step wise approach for determining the probable need of request is also presented.
Key words: Anesthesia; Analgesia; Referral/consultation, Preoperative; Anesthesiologist; Cardiologist, Non-cardiac surgery
Citation: Karim HMR. Is majority of requests by anesthesiologists for cardiologist consultation unjustified? Anaesth Pain & Intensive Care 2016;20 Suppl 1:S109-S114
Received: 18 September 2016; Reviewed: 10 October 2016; Accepted: 15 October 2016
INTRODUCTION
Preoperative anesthesia check up (consultation) has become an integral part of perioperative care for surgical patients. Observational studies examining the clinical utility of preoperative consultation suggest that it reduces postoperative length of stay.1,2 Many a time anesthesiologist needs to refer the patient to other specialty / super specialty health discipline for consultation and request for cardiologists consultation is also one of them. The purposes of a cardiology consultation are to treat an inadequately treated cardiac condition before surgery, to provide data to use in anesthesia management, and possibly to diagnose a medical condition before surgery which can yield in terms of new therapy impacting perioperative management.3,4
It is well known to health care providers that overuse, underuse and misuse are very important concerns in health care delivery which can lead to patients receiving inappropriate or unnecessary care. 5 Unnecessary referral / consultation even lead to delay in risk stratification / fitness declaration and increases hospital stay.6,7 This mini review is aimed at finding the practice patterns of anesthesiologists’ preoperative requests for cardiology consultations. It is also tried to summarize the justified requests which is expected to help anesthesiologists in rationalizing practices.
PREOPERATIVE CARDIOLOGY CONSULTATION PRACTICES
Preoperative cardiology consultation request is mostly given in patients with known or suspected cardiovascular disease planned for non-cardiac surgery. The common cardiac co morbid diseases leading to consultations are hypertension, coronary artery disease, atrial fibrillation, congestive heart failure etc.8 The precise frequency of preoperative cardiology consultation is difficult to figure out as preoperative consultation services are variable among different hospitals.8 Cardiology consultation is also likely to be same and it may even very among anesthesiologists of same hospital. A study including 13,673 patients undergoing a variety of common procedures (primarily low-risk surgeries) had found that 1.28% of the patients received preoperative cardiology consultation.9 In another observational study with relative smaller participants but including intermediate and high risk surgeries as well have found that the rate of referral by anesthesiologists to cardiologist was 5.33%.6 Similarly, the frequencies of cardiology referral / consultation among all the preoperative medical referrals / consultations are also variable. It was reported as 5.7% in facilities having family physicians to 33 – 40% in facilities without family physician.6,9,10 This indicate that the request of preoperative cardiology consultation is quite prevalent and an area of concern.
The reason for request for preoperative cardiology consultation is also variable. In a retrospective review of cardiology consultations at a university hospital, it was found that 53.47% just asked for an “evaluation,” 39.11% asked for a “clearance,” and 4.46% did not specifically request anything and only 2.97% posed a specific question.11 Incidental and insignificant findings in electrocardiogram and even preoperative risk stratifications have also been shown as reason behind preoperative cardiology consultation.6,12 As a result, the cardiologist often makes broadly inclusive, general remarks (like ‘patient cleared for surgery, patient can be taken up with high-risk, use invasive hemodynamic monitoring etc’) about perioperative management of the patient and may recommend preoperative diagnostic work-up.7,13
ARE ALL PREOPERATIVE CARDIOLOGY CONSULTATION REQUESTS JUSTIFIED?
The value of preoperative cardiology consultation cannot be underestimated, but it is uncertain whether these consultations reach their expected goals.14 Preoperative cardiology consultation also seems to be overused.12,15 Although, previous study has shown that assigning the anesthesiologist with the responsibilities of deciding which patients need further evaluation has been associated with a 73% decrease in preoperative consultations,16 anesthesiologists are still asking inappropriate / unnecessary cardiology consultations.6 In a prospective observational study, it was found that 3 out of 4 cardiology referral (75%) was not required / inappropriate.6
Examining the cardiology consultation requests in 712 patients scheduled for elective surgery, Aslanger et al. found that the cardiologists revealed an abnormality in 67.8% and recommended further work up in 58.7% of the patients. However, they contributed to the clinical course in only 36.9%. It was also found that when the algorithm was applied to ‘routine pre-operative evaluation’ requests lacking a specific question, only 7.6% of these consultation requests required further investigation.15 Another study evaluating the indication of the requests for preoperative cardiac consultation for in patients undergoing non-cardiac surgery found that only 26.5% of the requests were according to the 2009 ACC/AHA guidelines.17
A study with 100 patients of positive cardiac history and symptoms and signs suggestive of cardiac disease, screened by anesthetist and referred to single cardiologist for cardiac risk stratification and further treatment (if required) found that only 16% were identified as high risks and only one patient needed further intervention; even though 55% patients had cardiac co morbidities.12 Evaluating the effect of preoperative cardiology consultation prior to elective aortic aneurysm repair on patient morbidity, it was found that although those patients who had a preoperative cardiology consult were at greater risk, there were no decrease in postoperative cardiac complications.18 These clearly indicate that requesting a cardiology consultation in all patients having cardiac co morbidities / undergoing major and high risk surgeries does not change anesthetic management and postoperative outcome much and thus preoperative consultation in all patients cannot be accepted or justified.
WHEN TO REQUEST A CARDIOLOGY CONSULTATION?
The preoperative request for consultation by other specialty should probably be governed by the same rule as for preoperative investigations and should be asked if only it is going to change anesthetic management of the patient. It is recommended that the preoperative investigation should be based on the history, physical examination, perioperative risk assessment, and clinical judgment,19 anesthesiologist should ask for cardiology or other specialty consultation based on the patients history, physical examination, functional capacity (as judged clinically by metabolic equivalents of task), co morbid conditions and type of the indexed surgery and its risk estimate. European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA) recommend a multidisciplinary expert team for pre-operative evaluation of patients with known or high risk of cardiac disease undergoing high-risk non-cardiac surgery.20 In their guideline ESC and ESA also recommends regarding cardiovascular assessment and management of cardiac patients planned for non-cardiac surgery.20
Literature has clearly shown that in terms of perioperative management—other than the management of perioperative acute coronary syndromes—the cardiology consultation has little to add and even non-cardiac surgery can be done in patients with severe aortic stenosis.4,13 Therefore the decision for preoperative cardiac assessment or cardiology consultation probably can be best derived from the stepwise approach to perioperative cardiac assessment and treatment algorithm for coronary artier disease provided by American college of cardiology (ACC) and American heart association (AHA).21 It is clear from the ESC/ESA and ACC/AHA guideline that the further cardiac evaluation of patients planned for non-cardiac surgery should be based on cardiac conditions, type and urgency of the surgery, estimated perioperative risk of major adverse cardiac events on the basis of the combined clinical/surgical risk, functional capacity etc.20, 21 Active cardiac conditions and clinical cardiac risk factors are presented in Boxes 1 and 2 respectively.20,22
| Box 1: Active or unstable cardiac conditions.
(Adapted from 2014 ESC/ESA and 2007 ACC/AHA guideline for non-cardiac surgery)20,22 |
|
| Box 2: Clinical risk factors for cardiac surgery. (Adapted from 2014 ESC/ESA and 2007 ACC/AHA guideline for non-cardiac surgery)20,22 |
|
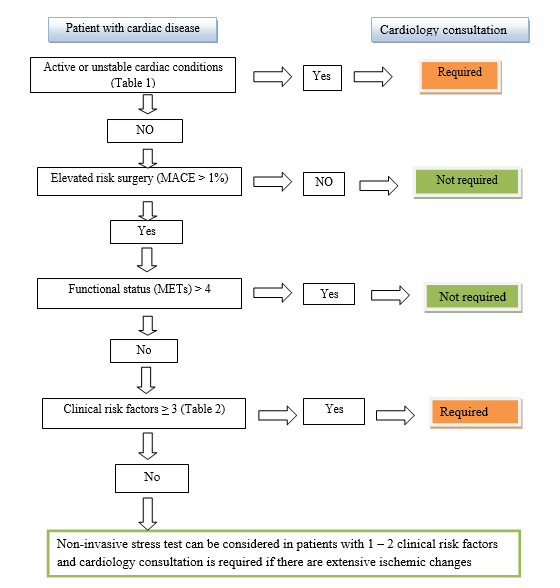
A suggested stepwise algorithm for determining the need of preoperative cardiology consultation request Figure 1. As the reasons for request of preoperative cardiology consultations differ from hospital to hospital and even anesthesiologist to anesthesiologist, possible clinical situations with suggested preoperative cardiologic consultation requests for elective non-cardiac surgery are presented in Table 1 based on the current literature, recommendations and guidelines.
Figure 1: Stepwise flow chart for preoperative cardiac consultation request for elective surgery (MACE- Major adverse cardiac events, METs- Metabolic equivalent of Tasks) adapted from 2014 ACC/AHA and 2014 ESC/ESA guideline for cardiac evaluation for non-cardiac surgery.
It is very much clear that despite having evidence based guidelines inappropriate practices are still well prevalent. The maximum benefit of these recommendations and guidelines probably can be obtained by following and developing institutional / national adapted protocols.23 In an era when anesthesiologists are claiming and considered as perioperative physicians, profession demands behavioral changes of anesthesiologists as well over and above the name change.13 The post graduate training / residency program in anesthesiology should also be adapted accordingly and probably a posting in cardiology and internal medicine is also required for such change.
Table 1: Possible clinical situations with suggested preoperative cardiologist consultation request for elective non-cardiac surgery. (Prepared from 2014 ESC/ESA and 2014 ACC/AHA guideline for non-cardiac surgery and Parks review)3,20,21
| Clinical situations | Comments with regard to cardiac consultation |
| Controlled arterial Hypertension
Uncontrolled arterial Hypertension
Malignant arterial Hypertension |
Proceed with surgery
Proceed with surgery if blood pressure < 180 / 110 mmHg in adults. Consider escalation of dose. If uncontrolled with 3 drugs, request for cardiology consultation Postpone surgery and request cardiology consultation |
| Known case of Coronary Artery Disease, Heart Failure
Acute / severe / decompensated Stable / optimized / chronic |
Postpone surgery and refer to cardiologist for treating / optimization of cardiac condition
Proceed with surgery with risk stratification and reduction strategies / medication continued |
| Unexplained, new onset dyspnea / chest pain | Request cardiologist consultation for ruling out /treating (if required) of active cardiac conditions |
| Post Percutaneous Transluminal Coronary Angioplasty / Coronary Artery Bypass Graft within 6 years | With asymptomatic stable / improved condition and good METs can be proceeded for surgery |
| Severe aortic stenosis symptomatic
Severe aortic stenosis asymptomatic
Severe Mitral stenosis Regurgitant valvular heart disease |
Postpone high risk surgery, request consultation of cardiology and cardiac surgeon for valve replacement / balloon valvuloplasty
Proceed with low and intermediate risk surgery. Request consultation if planned for high risk surgery If with symptoms of severe pulmonary hypertension, postpone surgery and request cardiology consultation Request consultation if there is symptoms and signs of severe heart failure / left ventricular dysfunction |
| Patients with prosthetic valve | Modify anticoagulation and proceed for surgery unless there is valve / ventricular dysfunction |
| Severe pulmonary arterial hypertension (PAH) | Request cardiology consultation for an optimized treatment regimen and proceed with PAH- specific medication continued |
| Arrhythmias / Dysrhythmia | Request consultation if acute, symptomatic and significant arrhythmias / or pacemaker is indicated before proceeding for surgery.
Premature beats, fascicular blocks, bradycardia without symptoms, fist degree and second degree Mobitz type I do not need request for cardiology consultation and can be proceed with surgery |
| Peripheral arterial disease | Request consultation if > 2 clinical risk factors are present |
| Patients with unknown functional capacity | Exercise stress testing may be reasonable to perform for major / elevated risk surgery |
| Drugs (Anticoagulant, beta blocker, anti-hypertensive, statin etc) | Manage as per guideline / recommendations. If beta blocker is indicated but patient is not amenable, request for cardiology consultation |
| Investigations (electrocardiogram, echocardiography, stress test, cardiopulmonary exercise testing etc) | Ask for the investigation if indicated. Cardiology consultation request is required only if the abnormality mandates active cardiac management before proceeding with surgery for better outcome |
| Risk stratification, Clearance | No. It is the anesthesiologists job / duty |
| Pacemaker in situ | Proceed as per recommendation. Go through documents |
CONCLUSION
Mere presence of a cardiovascular disease does not warrant preoperative cardiology consultation. Stable cardiovascular disease including asymptomatic coronary artery disease patient can undergo non-cardiac surgery without preoperative cardiology consultation with appropriate perioperative medication and monitoring by anesthesiologist. A consultation request for risk stratification, clearance for surgery should not be done rather a request for preoperative cardiology consultation should be done if it is going to change the course of perioperative management.
Acknowledgement: None
Competing Interest: None
Author contribution: This manuscript has been prepared by the author, and he accepts full responsibility for the correctness of the material given.
REFERENCES
- Wijeysundera DN, Austin PC, Beattie WS, Hux JE, Laupacis A. A population-based study of anesthesia consultation before major noncardiac surgery. Arch Intern Med 2009;169:595-602.
[PubMed] [Free full text] doi:10.1001/archinternmed.2009.3
- Chan FW, Wong F, Cheung YS, Chui PT, Lai PB. Utility of a preoperative assessment clinic in a tertiary care hospital. Hong Kong Med J 2011;17:441-5.
- Katz RI, Barnhart JM, Ho G, Hersch D, Dayan SS, Keehn L. A survey on the intended purposes and perceived utility of preoperative cardiology consultations. Anesth Analg 1998;87:830–6.
- Park KW. Preoperative cardiology consultation. Anesthesiology 2003;98:754–62.
- Lambrinos, A. Preoperative consultations: a rapid review. Toronto: Health Quality Ontario; 2014 March [cited 2016 Sept 17]:p1-19. [Free full text]
- Karim HM, Yunus M, Bhattacharyya P. An observational cohort study on pre-operative investigations and referrals: How far are we following recommendations? Indian J Anaesth 2016;60:552-9. [PubMed] [Free full text] doi:10.4103/0019-5049.187783
- Braham RL, Ron A, Ruchlin HS, Hollenberg JP, Pompei P, Charlson ME. Diagnostic test restraint and the specialty consultation. J Gen Int Med 1990;5:95–103.
- Wijeysundera DN, Austin PC, Beattie WS, Hux JE, Laupacis A. Variation in the practice of preoperative medical consultation for major elective noncardiac surgery: a population-based study. Anesthesiology 2012;116:25-34.
[PubMed] doi: 10.1097/ALN.0b013e31823cfc03
- Thilen SR, Bryson CL, Reid RJ, Wijeysundera DN, Weaver EM, Treggiari MM. Patterns of Preoperative Consultation and Surgical Specialty in an Integrated Healthcare System. Anesthesiology 2013;118:1028-37.
[PubMed] [Free full text] doi: 10.1097/ALN.0b013e31828ea68a
- Paik H, Lim C-W, Ryu H-G. Characteristics and effectiveness of preoperative consultations in a tertiary hospital. Korean J Anesthesiol 2013;65(6 Suppl):S4-S5.
[PubMed] [Free full text] doi:10.4097/kjae.2013.65.6S.S4
- Kleinman B, Czinn E, Shah K, Sobotka PA, Rao TK: The value to the anesthesia-surgical care team of the preoperative cardiac consultation. J Cardiothor Anesth 1989;3:682–7.
- Malik MN, Fatima N, Farah, Memon MI. Preoperative Anesthesia Referrals to Cardiology and Outcome in a Tertiary care hospital. Ann Pak Inst Med Sci 2014; 10(2):89-92.
- Kleinman B. Preoperative Cardiology Consultation: How Helpful Is It? Anesthesiology 2003;99:1240. [PubMed]
- Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof EL, Fleischmann KE, et al. 2009 ACCF/AHA focused update on perioperative beta blockade incorporated into the ACC/AHA 2007 guidelines on perioperative cardiovascular evaluation and care for noncardiac surgery: a report of the American college of cardiology foundation/American heart association task force on practice guidelines. Circulation 2009;120:e169-276. [PubMed] [Free full text] doi:10.1161/CIRCULATIONAHA.109.192690
- Aslanger E, Altun I, Guz G, Kiraslan O, Polat N, Golcuk E, Oflaz H. The preoperative cardiology consultation: goal settings and great expectations. Acta Cardiol 2011;66:447-52. [PubMed] [Free full text] doi:10.2143/AC.66.4.2126592
- Fischer SP. Development and effectiveness of an anesthesia preoperative evaluation clinic in a teaching hospital. Anesthesiology 1996;85:196-206. [PubMed] [Free full text]
- Antonelli D, Jabaren M, Turgeman Y. Requests for preoperative cardiology consultation for patients undergoing non cardiac surgery. Harefuah 2014;153:515-7, 559-60. Hebrew. [PubMed]
- Eliassen AM, Davis FM, Phillips AR, Robinson AB, Henke PK. Effect of Preoperative Cardiology Specialty Consultation Prior to Elective Aortic Aneurysm Repair on Patient Morbidity. J Vasc Surg 2015;61 (6 suppl):S58. [Free full text] doi: 10.1016/j.jvs.2015.04.106.
- Feely MA, Collins CS, Daniels PR, Kebede EB, Jatoi A, Mauck KF. Preoperative Testing Before Noncardiac Surgery: Guidelines and Recommendations. Am Fam Physician 2013;87:414-8.
- Kristensen SD, Knuuti J, Saraste A, Anker S, Botker HE, Hert SD, et al. 2014 ESC/ESA Guidelines on non-cardiac surgery: cardiovascular assessment and management: The Joint Task Force on non-cardiac surgery: cardiovascular assessment and management of the European Society of Cardiology (ESC) and the European Society of Anaesthesiology (ESA). Eur Heart J 2014;35:2383-431. [PubMed] [Free full text] doi:10.1093/eurheartj/ehu282
- Fleisher LA, Fleischmann KE, Auerbach AD, Barnason SA, Beckman JA, Bozkurt B, et al. 2014 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2014;130:2215-45. [PubMed] [Free full text] doi:10.1161/CIR.0000000000000105
- Fleisher LA, Beckman JA, Brown KA, Calkins H, Chaikof EL, Fleischmann KE, et al. 2007 ACC/AHA guideline on perioperative cardiovascular evaluation and management of patients undergoing noncardiac surgery: a report of the American College of Cardiology/American Heart Association Task Force on Practice Guidelines. Circulation 2007;116:418-99. [PubMed] [Free full text]
- Yunus M, Karim HM, Dey S. What is new in guidelines on preoperative tests and how to maximize benefit out of different guidelines? Archives Medical Review Journal. Forthcoming 2017;26:



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube