
Mohammad Hamid, MBBS, Diplomate American Board1, Mohammad Irfan Akhtar, MBBS, FCPS2
1Associate Professor; 2Assistant Professor
Department of Anesthesia, Aga Khan University, Karachi (Pakistan)
Correspondence: Dr Mohammad Hamid, Associate Professor, Department of Anesthesia, Aga Khan University, PW II, Stadium Road, Karachi, 74800 (Pakistan); Tel: +923486 4639; E-mail: mohammad.hamid@aku.edu
ABSTRACT
Intraoperative use of transesophageal echocardiography (TEE) for monitoring and diagnostic purposes has increased over the years in cardiac surgical patients and anaesthesiologists have taken a lead to develop expertise in performing this examination. TEE has proved to be helpful in the management of non-cardiac surgical and Intensive care unit patients particularly those patients who are haemodynamically unstable. It provides important information about ventricular and valvular anatomy and its function. Certain structures which are difficult to visualize by transthoracic echocardiography can be demonstrated easily by TEE. Several guidelines have been established for performing comprehensive TEE examination and cardiologists and anaesthesiologists follow these guidelines to identify any cardiovascular abnormality.
TEE use is limited to very few centres in Pakistan, mainly due to the equipment cost and lack of expertise. In addition, there are no established TEE training institutes. The main purpose of this article is to provide basic information about transesophageal echocardiography machine, TEE probe and how to obtain standard images by probe manipulation.
Key words: Transesophageal Echocardiography; Intraoperative; Guidelines; Ultrasound;
Echocardiography, Doppler; Doppler; Ultrasonography; Diagnosis; Diagnostic Techniques and Procedures
Citation: Hamid M, Akhtar MI. Introduction to basic transesophageal echocardiography (TEE) and standard views. Anaesth Pain & Intensive Care. 2016;20 Suppl 1:S91-S96
Received: 23 May 2016; Reviewed: 30 May 2016; Corrected: 28 June 2016; Accepted: 10 July 2016
INTRODUCTION
Transesophageal echocardiography (TEE) has become an essential component of cardiac anaesthesia and its value in cardiac surgery(1) is well established. In addition, it is increasingly being used for cardiac assessment and monitoring in intensive care(2) and non-cardiac surgeries(3, 4). TEE has been used to optimize perioperative care in patients with high risk for cardiac event and for quick assessment of cardiac function and fluid status in haemodynamically unstable patients. Intraoperative use of TEE was introduced in 1980 and comprehensive guidelines for intraoperative examination were published in 1999 by American Society of Echocardiography and Society of Cardiovascular Anesthesiologists(5) (ASE/SCA). A 2-D echocardiography is the most common mode used for examination along with Doppler assessment. A 3-D examination is also evolving and gaining popularity particularly during valvular repairs(6). Guidelines for 3-D echocardiography examination have also been developed(7). ACC/AHA guidelines discourage the routine use of TEE but recommended that it can be used in emergency situations where corrective therapy for haemodynamic instability failed in non-cardiac surgery patients (Class IIa recommendation)(8).
TEE provides important information about ventricular and valvular anatomy and function. Certain structures which are difficult to visualize by transthoracic echocardiography can be demonstrated easily by TEE. Main advantage of TEE is that it can be introduced even during the surgery on thoracic and abdominal region. Other advantages of TEE include the presence of transducer close to posterior structures and high resolution images due to absence of intervening lung or bones.
Echocardiography uses high frequency sound waves (also called ultrasound). As we know that sound is a form of energy that travels in waves. When a sound wave strikes a solid or fluid filled structure, some of the waves reflected back to the transducer and these reflected sound waves are called echoes. A sound wave can travel easily through gaseous structure but travel fastest through solids. Sound waves obey the law of reflection, refraction, diffraction and attenuation. Sound waves are sent through a device at the end of echo probe called transducer. A 2-D image is obtained by sweeping the ultrasound beam.
ECHO MACHINE & IMAGE OPTIMIZATION
Same machine is used for Transthoracic and Transesophageal Echocardiography. Knowledge about the echocardiography machine is an essential component of TEE examination. Several adjustments are needed to improve the quality of image and better examination. Machine has a monitor and several knobs and sliders on front panel which helps in optimization of image quality. Different knobs and their functions are explained below.
The depth should be set just beyond the structure of interest. Higher depth setting leads to reduction in size of image and also slows the frame rate because system has to wait longer for signals to be received. Once the structure of interest is visible and centred, do not increase the depth. Image gain increases the sensitivity (amplitude) of the system to the returning signals, similar to volume control in audio system. If sets too high, the image will appear bright and tissues like MV appears thickened. Too low gain will show only pericardium. It should be adjusted in such a manner that the blood appears nearly black and cardiac tissues as grey.
Time gain compensation (TGC) are several slider type panels which allow differential adjustment of gain. These should be used to eliminate artefacts and optimize the image. TGC should be used frequently. Normally TGC controls are set lower for near field and higher for the far field. Focus appears as arrow head on left side of image and should be adjusted to the level of structure of interest. If focus point is too far away from the structure of interest, the image resolution will not be adequate. Higher frequencies are used when structure is close to the transducer (Atria, AV) while lower frequencies are helpful when structure is far from transducer (Deep transgastric view).
Color gain increases or amplifies the signals generated by the returning echoes. Set color gain by increasing the color gain control until speckles of color appear outside the blood pools and then decrease the gain one to two settings until the speckles go away. Too high gain will overestimate the regurgitant jet. Sector size controls the angle of sector displayed on the monitor. This angle ranges from 15-90 degree. The most important effect of the sector size is on the frame rate. The wider the sector size, the lower the frame rate and the temporal resolution. Sector size should be kept small for fast moving objects.
Safety and precautions for TEE examination
Review the history and previous transthoracic examination before TEE examination. Insert the probe after intubation and use a bite block. Never use force when inserting the probe and always direct the probe centrally towards the back of pharynx after lifting the mandible. Use of TEE is contraindicated in patients with swallowing problems and esophageal diseases. When probe is not in use e.g. during cardiopulmonary bypass period, then either freeze the image or turn off the power. Do not insert the probe after the patient is heparinised.
TEE Probe and its Manipulation
TEE probe is basically a gastroscope with a small transducer mounted at the tip. Probe has two knobs at the handle. Larger control wheel is used for ante flexion and retro flexion while smaller wheel is used for left or rightward flexion of the tip of TEE probe. One electronic switch at the handle, scan the heart in various axial views. It ranges from 0 degree to 180 degree.
Echo probe functions on the principle of piezoelectric effect. The word originates from the Greek word “Piezein” which denotes “to press”. TEE probe contains several piezoelectric crystals (Quartz, Barium titanate, and tourmaline), which vibrate when voltage is applied. These vibrations produce sound waves which propagates in particular direction. These waves can be directed as a beam and returning signals again change the shape of crystals which emit electrical signals. These echoes are converted into the cardiac images on the monitor.
Movement of TEE probe
Quality of image can be improved by using a larger control wheel on the handle which provides angulation (Ante flexion or retro flexion) while smaller knob is used for tilting the probe laterally (Left or right). Whole probe can also be turned clockwise and ante clockwise (called turning right or left). Rotation of whole Image plane is possible by controlling the axis rotation between the range of 0 -180 degrees. It is called rotating forward if the angle moved from 0 degrees towards 180 degrees.
STANDARD VIEWS (Figure 1)
ECHO is a two dimensional (cross section) representative of anatomical structure which exists in three dimensions in space. A 2D image obtained in a transverse plane at 0° is perpendicular to the shaft of transducer while at 90° it lies in the vertical plane and runs parallel to the shaft of probe.
Short axis means the image is perpendicular to anatomical structure and long axis is parallel to structure of interest. Apex of the image is close to the probe while arc of the image sector shows more distal structures. Each structure must be examined in multiple planes if possible.
ASE/SCA task force has developed guidelines of intraoperative echo examination and recommends 20 standard images. These guidelines were revised in 2014 and 8 more standard views are added(9). Reeves et al. have suggested only 11 views for basic TEE examination during perioperative period and in the intensive care unit patients(10).
Consent is taken from all the patients before examination and for the procedural sedation propofol is commonly used(11). Study begins by inserting ECHO probe to mid esophagus (ME) which is about 35cm from incisors. It is suggested to push TEE probe into stomach after mid esophageal examination and finally pulled out in upper esophagus.
MIDESOPHAGEAL (ME) VIEWS
In the mid esophagus position, the transducer is just behind the left atrium. Keep the angle at 0° degree and move the probe up and down to obtain Four chamber view. Structures seen are left atrium (LA), left atrial appendage (LAA), right atrium (RA), RV, LV (Septal & Lateral wall), mitral valve (MV) and tricuspid valve (TV). After obtaining four chamber view rotate the axis from 0° to 60-70 degree and you will be able to see LA, LV and MV. This view (Mitral Commissure view) is mainly used for assessment of MV pathology. Further 90° rotation (Range 80-100) will provide Two chamber view and shows the LA, LAA, MV and anterior & inferior walls of LV. At this position if we turn the probe towards left side pulmonary veins (left sided) becomes visible. Use color flow to confirm this finding.
From four chamber view create an angle of 135° (Long axis (LAX) view, Range 120-160°) and you will be able to visualize LA, LV, LVOT, Aortic valve, MV and ascending aorta. Two cusps of aortic valve will be visible in this view. From four chamber view withdraw the probe slightly and rotate 40° (AV short axis view, range 30 – 60) to see Mercedes Benz sign (Figure 1) of aortic valve. Right coronary cusp (RCC) is facing towards RV and LCC at right of screen. Non coronary cusp, Interatrial septum and RV outflow tract are also visible.
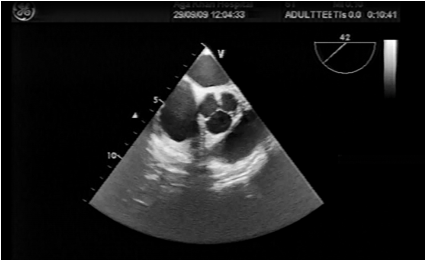
Image 1: AV short axis view showing Aortic valve in closed position with three aortic cusps in the middle
From AV short axis view rotate further 80 degrees (RV inflow – outflow view) to see RA, TV, RV, RV outflow tract, pulmonary Valve and main Pulmonary artery. This view is very helpful in tetralogy of Fallot repair. Turn the probe right and rotate at about 110° (Bicaval view, Range 80 – 110° from AV SAX) and watch SVC, IVC, RA, LA, interatrial septum, Eustachian valve (Figure 2). This view is used to confirm the position of the tip of central venous pressure (CVP) line. Right pulmonary vein can also be visualized in this view by turning the probe to right side.
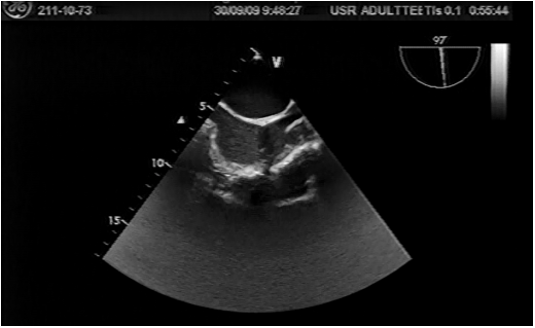
Image 2. Bicaval view showing SVC on right side and IVC on left side
AV long axis view is obtained by rotating from AV SAX view to 120 -160°. You will be able to see Proximal ascending aorta, LV outflow, MV, AV, Lower most RCC and adjacent to anterior MV leaflet is non coronary cusp. Withdraw TEE probe slightly from AV SAX view and rotate about 40° (Ascending aorta short axis view) to see proximal ascending aorta, Main pulmonary artery, right pulmonary artery and SVC.
Further rotation to around 130° will give you Long axis view of Ascending called Ascending aorta long axis view. Aorta along with Right pulmonary artery (short axis) will be visualized.
Transgastric view (TG)
From the mid esophagus position pushed down the probe, so that the tip of the TEE probe is in the stomach (40-45 cm from incisor). Now anteflex the tip of TEE probe to assess ventricle from base to apex.
In this view (TG basal short axis view (0°)) the basal portion of the ventricle and MV should be visible. This view is helpful in detection of basal LV ischaemia and assessment MV pathology. TG Mid SAX view (0° range 0-15) is obtained by advancing the probe slightly and then anteflexion at the tip. Posteromedial papillary muscle can be appreciated at 1° O’clock and anterolateral muscle at 5° O’clock position. This view is useful for monitoring global LV function. Ejection fraction estimation can be done with the help of M-Mode in this view. This view is most important in detecting myocardial ischemia in different coronary artery territory.
From the mid TG view rotation of axis to 90° will show the Anterior (bottom) and inferior walls of left ventricle. This view is called TG two chamber view. By turning the whole probe clockwise will show you the right atrium and tricuspid valve. This image is called TG right ventricular inflow view.
Now advance the probe deep into the stomach then sharply anteflex and at the same time withdraw slowly to see Deep TG long axis view (0° about 45 -50 cm from incisor). This will show all four chambers, AV and LVOT. This view is basically used for doppler (CWD) examination to estimate velocities across AV. Finally, TG long axis view is visualized by rotating 120° from mid SAX view. Left ventricle in long axis and LVOT are clearly seen in this view.
Upper esophageal (UE) view (20-25 cm from incisor)
For visualization of great vessels reduce the screen depth to 6 cm and withdraw TEE probe gradually to ME four chamber view. Now turn the probe anticlockwise to find descending thoracic aorta SAX view at 0° and descending thoracic aorta LAX view at 90°.
Withdraw the probe further until distal aortic arch is seen then follow the arch by turning the probe towards right side. This is upper esophageal aortic arch LAX view at 0°. When transducer rotates to 90° UE aortic arch SAX view is seen. Origin of left subclavian artery is also seen.
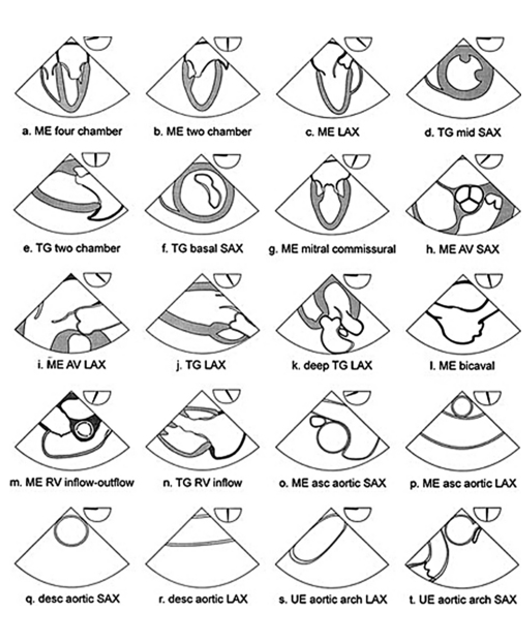
Figure 1: American society of echocardiography and Society of cardiovascular anesthesiologist recommended 20 cross sectional views for comprehensive TEE examination. ME= mid esophagus, LAX= long axis, SAX= short axis, TG= transgastric, AV= aortic valve, RV= right ventricle, asc = ascending, des= descending, UE= upper esophageal.
Left ventricle wall motion abnormalities: (Figure 3)
Left ventricle wall motion abnormalities can be detected by using 16 segments model as suggested by SCA/ASE. It consists of six basal segments, six segments at mid papillary level and four segments at apical level. Four chambers view, Two chambers view, TG basal SAX view, TG mid SAX view can provide information about all 16 segments. Involved coronary artery (Stenosed or Blocked) can be identified by looking at the regional wall motion abnormalities in these segments. The qualitative grading of wall motion is Normal (>30% thickening), Mild hypokinetic (10 – 30% thickening), severely hypokinetic (<10% thickening), Akinetic (No thickening) and dyskinetic (Moves paradoxically).
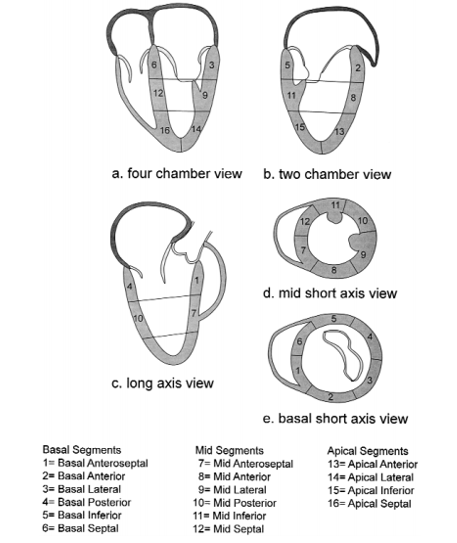
Figure 2: Sixteen segment model of the left ventricle.
DOPPLER EXAMINATION
It is a method of detecting the direction and velocity of moving blood within the heart and vessels. Doppler principle is used to understand the movement of blood and tissues in the body. Pressure gradients are derived by using Doppler analysis of blood flow. Doppler examination includes:
Pulsed wave Doppler (PWD)
Same transducer crystal is used for transmission and reception. It allows sampling of blood flow velocities from a specific intracardiac depth. PWD can measure only limited range of velocities. Flow velocity through the mitral valve can be easily detected by PWD.
Continuous wave Doppler (CWD)
Two crystals transducers are used, one continuously transmits and other continuously receives and processed the signals. Very high velocities like aortic stenosis can be measured. Blood flow along the entire beam is observed.
Color flow Doppler (CFD)
Different colors are used to designate the direction of blood flow. Red color is seen when blood flowing towards the probe while the blue color denotes the flow away from the probe. Mosaic pattern represent turbulent flow, usually seen when there is valvular stenosis or regurgitation.
INTRAOPERATIVE APPLICATION OF TEE IN ADULT CARDIAC SURGERY
TEE application in the intraoperative period is very important in the assessment of the biventricular function, cardiac fluid status, valvular repair accuracy, para-valvular leak, residual septal defect and intra-cardiac air. It plays an important complementary role with PAC in the successful management of high-risk cardiac surgical patients.
BASIC PERIOPERATIVE TEE EXAMINATION FOR NON CARDIAC SURGERY
Out of 20 cross sectional views used for comprehensive examination, seven can be utilized for basic TEE examination for non-cardiac surgery. These includes ME 4 chamber, ME two chamber, ME long axis, Transgastric mid SAX, ME RV inflow-outflow, Descending aortic SAX and upper esophageal aortic arch LAX view. This approach of perioperative TEE is proposed to improve time efficiency and diagnostic yield.
CONCLUSION
Improved outcomes have been seen after the introduction of Transesophageal echocardiography in cardiac surgery, particularly in the valve surgery. It provides valuable information about the anatomy and function of different chambers of heart and valves. Blood flow and velocity across the valves and in large vessels can also be identified. Certain structures which are difficult to visualize by transthoracic echocardiography can be demonstrated easily by TEE. It is important to know the various knobs on TEE machine and probe for better visualization of heart structures. Guidelines for comprehensive intraoperative TEE examination are also available for anaesthesiologists. These guidelines provide information about the TEE machine, probe insertion technique and how to manipulate probe to identify a particular structure. Doppler is also one of the important component of TEE examination which helps to detect the direction and velocity of moving blood within the heart and vessel.
Acknowledgement: We acknowledge the permission from Anesth Analg (Reference #5) for allowing us to use Figure 1 and 2 in this article
Conflict of interest: No conflict of interest declared by the authors
Authors’ contribution: KS & MH: Concept, Design, Literature search, Manuscript preparation & review
REFERENCES
- Klein AA, Snell A, Nashef SA, et al. The impact of intra-operative transoesophageal echocardiography on cardiac surgical practice. Anaesthesia 2009;64:947-952 [PubMed] [Free full text] doi: 10.1111/j.1365-2044.2009.05991.x.
- Maxwell C, Konoske R, Mark J. Emerging Concepts in Transesophageal Echocardiography. F1000Res. 2016:1-10. [PubMed] [Free full text] doi: 10.12688/f1000research.7169.1.
- Rebel A, Klimkina O, Hassan ZU. Transesophageal echocardiography for the noncardiac surgical patient. Int Surg 2012;97:43-55 [PubMed] [Free full text] doi: 10.9738/CC61.1.
- Guarracino F, Baldassarri R. Transesophageal echocardiography in the OR and ICU. Minerva Anestesiol 2009;75:518-529 [PubMed] [Free full text]
- Shanewise JS, Cheung AT, Aronson S, et al. ASE/SCA guidelines for performing a comprehensive intraoperative multiplane transesophageal echocardiography examination: recommendations of the American Society of Echocardiography Council for Intraoperative Echocardiography and the Society of Cardiovascular Anesthesiologists Task Force for Certification in Perioperative Transesophageal Echocardiography. Anesth Analg 1999;89:870-884 [PubMed]
- Mahmood F, Jeganathan J, Saraf R, Shahul S, Swaminathan M, Mackensen GB, et al. A Practical Approach to an Intraoperative Three-Dimensional Transesophageal Echocardiography Examination.J Cardiothorac Vasc Anesth 2016;30:470-490 [PubMed] doi: 10.1053/j.jvca.2015.10.014.
- Lang RM, Badano LP, Tsang W, Adams DH, Agricola E, Buck T, et al. EAE/ASE recommendations for image acquisition and display using three-dimensional echocardiography. J Am Soc Echocardiogr 2012;25(1):3-46 [PubMed] doi: 10.1016/j.echo.2011.11.010.
- Shillcutt SK, Markin NW, Montzingo CR, Brakke TR. Use of rapid “rescue” perioperative echocardiography to improve outcomes after hemodynamic instability in noncardiac surgical patients. J Cardiothorac Vasc Anesth 2012;26:362-370 [PubMed]
doi: 10.1053/j.jvca.2011.09.029.
- Hahn RT, Abraham T, Adams MS, Bruce CJ,Glas KE, Lang RM, et al. Guidelines for performing a comprehensive transesophageal echocardiographic examination: recommendations from the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr 2013;26(9):921-64 [PubMed] doi: 10.1016/j.echo.2013.07.009
- Reeves ST, Finley AC, Skubas NJ, et al. Basic perioperative transesophageal echocardiography examination: a consensus statement of the American Society of Echocardiography and the Society of Cardiovascular Anesthesiologists. J Am Soc Echocardiogr 2013;26(5):443-456 [PubMed] doi: 10.1016/j.echo.2013.07.009.
- Akaishi M, Asanuma T, Izumi C, Iwanaga S, Kawai H, Daimon M, et al. Guidelines for conducting transesophageal echocardiography (TEE): Task force for guidelines for conducting TEE: J Echocardiogr. 2016;14(2):47-8 [PubMed] doi: 10.1007/s12574-016-0281-9



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube