
Raghavendra Kotal, Md. Yunus, Habib Md. Reazaul Karim, Manuj K. Saikia, P. Bhattachryya, M. Singh, Mrinal Mandal
Department of Anesthesiology & Critical Care, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences (NEIGRIHMS), Shillong, Meghalaya – 793018, (India)
Correspondence: Dr Md. Yunus, Sub Dean (Research) Additional Professor, Anesthesiology & Critical Care, North Eastern Indira Gandhi Regional Institute of Health and Medical Sciences (NEIGRIHMS), Shillong, Meghalaya – 793018, (India); Phone: +91-0364-2538009 (O); +91-0364-2538049 (R); Cell: 91-9436706438 & 91-9774334284; E-mail: drmdyunus@hotmail.com
ABSTRACT
Background and aim: Acute kidney injury (AKI) after cardiac surgery occurs in approximately 1/3rd of the cases that require cardiopulmonary bypass (CPB) and is associated with worsened short and long term consequences. Preoperative anemia and perioperative packed cell transfusion are two important modifiable risk factors for AKI and elucidating their relationship may help in devising preventive strategies. The present study aimed to study the relationship between preoperative anemia and perioperative packed red blood cell transfusion with development of postoperative acute kidney injury in patients who underwent cardiac surgeries under CPB.
Methodology: The present prospective cohort study was conducted after ethical committee approval and informed consent from 60 eligible anemic and non-anemic patients (30 each). They were further sub grouped based on the number of packed red cell (PRC) units transfused. Occurrence and frequency of AKI was determined from the estimated glomerular filtration rate as per RIFLE criteria. The data collected were analyzed using INSTAT software for statistical significance.
Results: Demographic parameters, type of surgery, preoperative and intraoperative parameters were comparable in both the groups (p > 0.05). Preoperative hemoglobin level during CPB were significantly different in the anemic and non-anemic groups (p < 0.001). 50% of anemic patient suffered AKI as compared to 16.67% of the non-anemic patients, with a RR of 3.0 and p 0.01. RIFLE-injury was found in 23.33% of the anemic group as compared to 10% in the non-anemic group with a RR 2.33, p > 0.05. AKI was higher in patients who received 3 units of packed red cells as compared to lesser units of transfusion with a RR of 2.66 and p 0.01.
Conclusion: Both anemia and increased red cell transfusion during cardiac surgeries with cardiopulmonary bypass appear to be risk factors for acute kidney injury.
Key words: Cardiac anesthesia; Cardiac surgeries; Anemia; Acute kidney injury; Cardiopulmonary bypass
Citation: Kotal R, Yunus M, Karim HMR, Saikia MK, Bhattachryya P, Singh M, Mandal M. Influence of packed red cell transfusion on risk of acute kidney injury after cardiopulmonary bypass in anemic and non-anemic patients. Anaesth Pain & Intensive Care 2016;20 Suppl 1:S42-S47
Received: Nov 2015. Reviewed: Dec 2015; Feb 2016. Corrected: Jan 2016; Mar 2016. Accepted: Mar 2016.
INTRODUCTION
Acute kidney injury (AKI) after cardiac surgery under cardiopulmonary bypass (CPB) is a common postoperative complication and a major and serious health issue. It is characterized by an abrupt deterioration in kidney function as evidenced by a reduction in the glomerular filtration rate. Because of the dilutional effects of the CPB pump priming, this deterioration may not be detected in the first 1 to 2 days using conventional monitoring by serum creatinine levels.1 Approximately 24 – 30% of the cases undergoing cardiac surgery develop AKI of a variable severity, and about 1% of these may be so severe enough to require hemodialysis with short and long term consequences and increased mortality.2,3 The incidence of AKI may also vary based on the definition used to define it. An incidence as high as 39% has been found in a study done by Brown et al as defined by Acute Kidney Injury Network definition.4
There are non-modifiable as well as modifiable risk factors for AKI in patients undergoing cardiac surgery with CPB.5-8 Modifiable risk factors are total duration of bypass, non-pulsatile flow, ischemia time (aortic cross-clamping time), hemodilution during bypass, non-maintenance of mean arterial pressure (MAP) > 55 to 60 mmHg, blood transfusion during CPB, anemia etc.
Anemic patients are likely to get more packed red cells (PRC) transfusion during perioperative period leading to more free iron load and are expected to have increased incidence of AKI (both AKI risk and injury). The current study was devised to evaluate the relationship between preoperative anemia and intraoperative and immediate postoperative PRC transfusion in patients undergoing cardiac surgeries under CPB with occurrences of postoperative AKI (both RIFLE – Risk & RIFLE-Injury) as defined by Acute Dialysis and Qualitative Initiative (ADQI).9
METHODOLOGY
This prospective observational cohort study was conducted after ethical committee approval and informed consent from the eligible patient or the patient’s legal guardians during the year 2012-14. Patients were divided into anemic and non-anemic groups depending on preoperative hemoglobin (Hb) level. Preoperative Hb concentration of less than 12.5 g/dL (which is the average threshold of the World Health Organization’s sex-based anemia definition of 12.0 g/dL in women and 13.0 g/dL in men) were considered as anemic in the present study.10 Sixty patients aged between 15 to 60 years of both sexes undergoing elective cardiac surgeries under CPB were included. The sample size was calculated using http://www.openepi.com/Menu/OE_Menu.htm online for a finite population size of 250 with known frequencies of the outcome of 33.33% and absolute error of 10%. This gave a sample size of 61 for 95% confidence level. Patients who required preoperative blood transfusion due to severe anemia having Hb less than 7 gm%, preoperative renal failure, having Hb of more than 16 gm%, who required intraoperative intra-aortic balloon counter pulsation, deep hypothermic circulatory arrest, more than 3 units of PRC transfusion and who died within 3 days of surgery were excluded.
All patients were evaluated in pre-anesthetic clinic for anesthetic plan and to keep premedication and other preoperative advices homogeneous. Perioperative care was given by the same team of cardiac surgeon, anesthesiologist, intensivist, perfusionist and nursing team. The heart was approached by median sternotomy in all patients. Invasive arterial blood pressure was monitored and blood pressure was targeted within ± 20% of baseline pre bypass period and during CPB 50-60 mmHg of MAP were maintained. During non-pulsatile CPB, a flow of 2.4 to 3.0 L / min / m2 body surface was maintained. Blood cardioplegia was used in all cases and blood temperature of approximately 32º C was maintained during bypass. Heparin and protamine were used on body weight basis in all patients. Serial arterial blood gas analysis showed the hematocrit (Hct). Hct during bypass was targeted to minimum of 21% while during non-bypass time minimum of 24% intraoperatively. Re-warming was done up to 37º C before coming out from bypass. Vasoactive drugs, e.g. dopamine or dobutamine and/or NTG and occasionally adrenaline, were used as needed while coming out of bypass and postoperatively to maintain minimum of 65-70 mmHg MAP and effective left ventricular contraction. Postoperatively patients were managed in Intensive Care Unit (ICU). Hct was targeted to 30% in postoperative period.
Both anemic and non-anemic patients were further sub grouped based on the number of PRC units transfused (zero, one, two or three) during intraoperative and postoperative 24 hour. Data were collected from the pre-anaesthetic record, immediate preoperative, intraoperative and postoperative period.
AKI was determined from estimated glomerular filtration rate (eGFR) as per risk, injury, failure, loss of function, end stage renal disease (RIFLE) criteria of ADQI group.9 eGFR was calculated using COCKCROFT –GAULT equation.11 Both AKI Risk (RIFLE-R) and AKI Injury (RIFLE-I) were evaluated. The incidence was calculated mathematically and expressed in percentage scale while Fisher’s exact test was used for statistical analysis. Quantitative data were further analysed by unpaired t test. The INSTAT software (Graphpad software, Inc, La Zolla, CA, USA) was used for statistical analysis and a p value of < 0.05 was considered as statistically significant.
RESULTS
Demographic parameters were comparable in two groups, with no statistically significant differences (p > 0.05). Out of 60 patients 29 (48.33%) were males. Female patients were higher in anemic group (66.67%). Preoperative hemodynamics, random blood sugar, blood urea and serum creatinine levels were also not different statistically. CPB time and ischemia times were also comparable in both the groups with no statistical significant difference (p > 0.05). Intraoperative urine output, postoperative use of ionotropes / vasopressor support, duration and time till extubation were also comparable without statistically significant differences (p > 0.05). (Table 1) The common surgical procedures performed were valve replacements, atrial and ventricular septal defect repair and coronary artery bypass surgery.
Table 1: Showing the demographic and different clinical and laboratory parametric data analyzed using unpaired t test
| Parameter | Anemic
n or mean (SD or %) |
Non anemic
N or mean (SD or %) |
p value (two tailed) |
| Demographic profile
Male Age (years) Weight (kg) Height (cm) BSA (m2) Preoperative HR (/min) SBP (mmHg) DBP (mmHg) Hb (gm/dl) S. Creatinine (mg/dl) B. urea (mg/dl)
Intraoperative CPB time (min) Aortic X-clam (min) Urine output (ml) Lowest Hct in CPB (%) Postoperative Ionotropic support (hours) Time for extubation (hours) |
10 (33.33) 37.7 (12.66) 48.03 (6.52) 158.8 (7.08) 1.56 (0.43)
70.95 (7.69) 113.15 (10.34) 72.30 (7.87) 11.19 (1.32) 1.07 (0.36) 26.03 (11.68)
108.2 (47.06) 82.86 (36.04) 1189.7 (173.93) 28.9 (7.23)
11.13 (10.50) 11.26 (5.93) |
19 (63.33) 38.30 (12.9) 50.80 (6.75) 160.70 (8.39) 1.53 (0.12)
79.82 (9.14) 119.12 (12.62) 80.35 (8.62) 14.60 (1.41) 1.12 (0.24) 25.40 (10.65)
112.40 (60.47) 81.73 (48.84) 1246.3 (211.49) 34.6 (5.34)
9.36 (8.03) 12.23 (5.24) |
0.038 0.856 0.111 0.347 0.714
0.692 0.549 0.608 0.0001 0.529 0.828
0.764 0.925 0.256 0.001
0.446 0.504 |
Legend: SD- standard deviation, N- total number, n- number, BSA- body surface area, ASA- American Society of Anesthesiologists, HR- heart rate, SBP- systolic blood pressure, DBP- diastolic blood pressure, Hb- hemoglobin, RBS- random blood sugar, CPB- cardio pulmonary bypass, X-clam- cross clamp
The mean ± SD preoperative Hb level in anemic group was 11.19 ± 1.32 gm% as compared to 14.60 ± 1.41 gm% in the non-anemic group and the difference was highly significant (p < 0.001). The lowest Hct level during CPB in the anemic group and non-anemic group were 28.9 ± 7.23 and 34.6 ± 5.34 respectively and the statistical difference was highly significant (p < 0.001). 25 out of 30 (83.33%) anemic patients required 49 (59.76%) units of PRC transfusion as compared to 20 out of 30 (66.67%) of non-anemic patients, who required 33 (41.24%) units of PRCs.
Table 2: Showing the incidence of AKI in relation to anaemia and analysed results of Fisher’s exact test.
| AKI (class) | Anaemic
n (%) |
Non anaemic
n (%) |
RR | 95% CI | Two tailed p value |
| RIFLE (Risk)
RIFLE (Injury) |
15 (50)
7 (23.33) |
5 (16.67)
3 (10) |
3.00
2.33 |
1.24 – 7.20
0.66 – 8.18 |
0.012
0.299 |
Legend: RR- Relative risk, AKI- Acute Kidney Injury, RIFLE- Risk, Injury, Failure, Loss of function and End stage renal disease, CI- confidence interval
There was a threefold risk (p 0.01) of developing AKI (Risk) in anemic patients as compared to non-anemic patients. However, although the anemic patients were found to have more AKI-injury as compared to the non-anemic, the difference was not statistically significant. (Table 2) Incidence of AKI was higher in patients who received 3 units of PRCs as compared to no transfusion and less than 3 units of PRC transfusions (Table 3).
Table 3: Showing the incidence of AKI in relation to number of PRC units transfused and analyzed results of Fisher’s exact test
| AKI (class) | 3 PRC units
n/N (%) |
< 3 PRC units
n/N (%) |
RR | 95% CI | Two tailed p value |
| Anemic (N=30)
RIFLE (Risk) RIFLE (Injury) Non anemic (N=30) RIFLE (Risk) RIFLE (Injury) All (N=60) RIFLE (Risk) RIFLE (Injury) |
6/8 (75) 3/8 (37.5)
2/4 (50) 2/4 (50)
8/12 (66.67) 5/12 (41.67) |
9/22 (40.9) 4/22 (18.18)
3/26 (11.53) 1/26 (3.85)
12/48 (25) 5/48 (10.42) |
1.83 2.06
4.33 13.0
2.66 4.00 |
0.96 – 3.48 0.58 – 7.26
1.01 – 18.42 1.5 – 112.4
1.41 – 5.02 1.37 – 11.61 |
0.214 0.344
0.118 0.039
0.013 0.020 |
Legend: RR- Relative risk, AKI- Acute Kidney Injury, PRC- Packed Red Blood Cells, RIFLE- Risk, Injury, Failure, Loss of function and End stage renal disease, CI- confidence interval, n – number, N- total number
The incidence of AKI also increased along with the increase in the number of PRC units transfused (Figure 1).
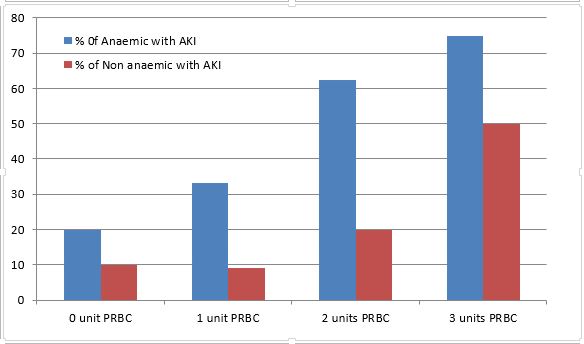
Figure 1: Showing the trend of AKI with regard to the number of PRC units transfused in both anemic and non-anemic group in % scale for each category
DISCUSSION
AKI in cardiac surgery is a major issue due to the fact that with minimal increase in creatinine postoperatively can have an impact on 30 days mortality,12 while further increase in creatinine level has an effect on late mortality of >5 years.12 In addition, it results in prolonged duration of ICU and hospital stay, as well as increased cost of treatment.13 Among the modifiable risk factors in AKI in cardiac surgery, anemia and perioperative PRC transfusions are important.12 The CPB, PRC transfusion and anemia14 are independent risk factors for AKI and the interplay between them substantially increases the risk if all of them are present at the same time in a patient all together.
The findings of the present prospective cohort study reconfirm the findings of a few retrospective studies. In a study by Kulier et al15 involving cardiac surgical patients with anemia (Hb < 13 gm%) found increased renal complication. De Santo et al16 and Karkouti et al17 also found increased incidence of acute renal insufficiency in anemic patients postoperatively who underwent cardiac surgeries.
In a retrospective study conducted by Karkouti et al18 have shown a statistically significant increase in risk of AKI following PRCs transfusion in cardiac surgery. They also found that AKI rates increased in direct proportion to the amount of erythrocytes transfused, and this increase was more pronounced in anemic patients. In the present prospective cohort study also it was noted that the incidence of AKI increases progressively in patients who received 3 units of PRC as compared to no transfusion or 1 unit and 2 unit transfusion in both the anemic and non-anemic groups, and it was also pronounced in anemic group as compared to non-anemic group.
The harmful effects of transfusion of blood including those acting on kidneys were reiterated by J. Murphy et al19 and Rao et al20 A study by Michael Haase et al21 demonstrated that avoiding transfusion when hemoglobin > 8 gm% can decrease AKI in cardiac surgical conditions. On the other hand, anemia in cardiac patients is associated with postoperative non-cardiac complications.16 These leads us to a dicey situation when it comes to decision making regarding perioperative PRC transfusion and target Hct. However, the present study is unable to comment on this and further studies with control will be required.
LIMITATIONS
Although the present study had an advantage of being prospective, it also had limitations as it is a single center with relatively small sample size and power and lacking multivariate analysis. Also, the possibility of known and unknown confounders on the result could not be ruled out as the participants were not randomized.
CONCLUSION
Both anemia and packed red cell transfusion during cardiac surgeries with cardiopulmonary bypass appear as risks for acute kidney injury, the incidence of AKI (RIFLE-R) being significantly higher. The incidence of acute kidney injury increases with increasing number of packed red cell units transfused both in anemic and non-anemic patients, but is more pronounced in anemic group. However, for the formulation of a plan on preoperative treatment of anemia to reduce acute kidney injury will require large prospective study with controls.
Conflict of interest: None
Authors’ contribution: RK: conduction of study works, statistical analysis, literature search and manuscript writing
MY: Concept, conduction of study works, literature search, manuscript editing & reviewing
HMRK: statistical analysis, literature search and manuscript writing & editing
MKS: Concept, conduction of study works
PB: Concept, manuscript editing and interpretation
MS: Concept and manuscript editing
MM: conduction of study and data collection
REFERENCES
- Mao H, Katz N, Ariyanon W, Blanca-Martos L, Adýbelli Z, Giuliani A, et al.Cardiac Surgery-Associated Acute Kidney Injury.Cardiorenal Med. 2013;3(3):178-99. [PubMed][Free full Text] DOI: 1159/000353134
- Rosner M H, Okusa M D. Acute kidney injury associated with cardiac surgery.Clin J Am Soc Nephrol. 2006 Jan;1(1):19 –32. [PubMed][Free Full Text] DOI: 10.2215/CJN.00240605
- Karkouti K, Wijeysundera D N, Yau T M, Callum J L, Cheng D C, Crowther M, et al. Acute Kidney Injury After Cardiac Surgery: Focus on Modifiable Risk Factors.Circulation. 2009;119(4):495-502. [PubMed][Free Full Text] doi: 10.1161/CIRCULATIONAHA.108.786913
- Brown JR, Kramer RS, Coca SG, Parikh CR.Duration of acute kidney injury impacts long-term survival after cardiac surgery.Ann Thorac Surg 2010;90(4):1142-8. [PubMed][Free Full Text] doi: 10.1016/j.athoracsur.2010.04.039
- Thakar CV, Liangos O, Yared JP, Nelson D, Piedmonte MR, Hariachar S, et al.ARF after open-heart surgery: Influence of gender and race.Am J Kidney Dis.(3) 2003;41:742-51. [PubMed]
- Chertow GM, Lazarus JM, Christiansen CL, Cook EF, Hammermeister KE, Grover F, Daley J. Preoperative renal risk stratification.Circulation. 1997;95(4):878-84. [PubMed][Free Full Text]
- Mangos GJ, Brown MA, Chan WY, Horton D, Trew P, Whitworth JA. Acute renal failure following cardiac surgery: incidence, outcomes and risk factors.Aust N Z J Med. 1995;25(4):284-9. [PubMed]
- Zanardo G, Michielon P, Paccagnella A, Rosi P, Caló M, Salandin V, et al. Acute renal failure in the patient undergoing cardiac operation. Prevalence, mortality rate, and main risk factors.J Thorac Cardiovasc Surg. 1994;107(6):1489-95. [PubMed]
- Bellomo R, Ronco C, Kellum JA, Mehta RL, Palevsky P, ADQI workgroup. Acute renal failure – definition, outcome measures, animal models, fluid therapy and information technology needs: the Second International Consensus Conference of the Acute Dialysis Quality Initiative (ADQI) Group.Crit Care. 2004;8(4):204–12. [PubMed] doi: 10.1186/cc2872
- Haemoglobin concentrations for the diagnosis of anaemia and assessment of severity. Vitamin and Mineral Nutrition Information System. Geneva, World Health Organization, 2011 (WHO/NMH/NHD/MNM/11.1) available at http://www.who.int/vmnis/indicators/haemoglobin.
- Cockroft DW, Gault MN. Prediction of creatinine clearance from serum creatinine.Nephron. 1976; 16(1): 31-41. [PubMed]
- Lassnigg A, Schmidlin D, Mouhieddine M, Bachmann LM, Druml W, Bauer P, Hiesmayr M. Minimal Changes of Serum Creatinine Predict Prognosis in Patients after Cardiothoracic Surgery: A Prospective Cohort Study.J Am Soc Nephrol. 2004;(6)15:1597–1605. [PubMed][Free Full Text]
- Dasta JF, Kane-Gill SL, Durtschi AJ, Pathak DS, Kellum JA. Costs and outcomes of acute kidney injury (AKI) following cardiac Surgery.Nephrol Dial Transplant. 2008; 23(6): 1970–4[PubMed][Free Full Text] doi: 10.1093/ndt/gfm908.
- Karkouti K, Wijeysundera DN, Yau TM, Callum JL, Cheng DC, Crowther M, et al. Acute kidney injury after cardiac surgery: focus on modifiable risk factors.Circulation. 2009; 119(4): 495–502. [PubMed][Free Full Text] doi: 10.1161/CIRCULATIONAHA.108.786913.
- Kulier A, Levin J, Moser R, Rumpold-Seitlinger G, Tudor IC, Snyder-Ramos SA, et al. Impact of preoperative anaemia on outcome in patients undergoing coronary artery bypass graft surgery.Circulation. 2007;116(5):471– 9. [PubMed][Free Full Text] DOI: 10.1161/CIRCULATIONAHA.106.653501
- De Santo L, Romano G, Della Corte A, de Simone V, Grimaldi F, Cotrufo M, et al.Preoperative anaemia in patients undergoing coronary artery bypass grafting predicts acute kidney injury.J Thorac Cardiovasc Surg. 2009;138(4):965-70. [PubMed][Free Full Text]
- Karkouti K, Wijeysundera DN, Beattie WS,Reducing Bleeding in Cardiac Surgery (RBC) Investigators. Risk Associated With Preoperative Anaemia in Cardiac Surgery: A Multicenter Cohort.Circulation. 2008;117(4):478-84. [PubMed][Free Full Text] doi: 10.1161/CIRCULATIONAHA.107.718353.
- Karkouti K, Wijeysundera DN, Yau TM, McCluskey SA, Chan CT, Wong PY, Beattie WS. Influence of Erythrocyte Transfusion on the Risk of Acute Kidney Injury after Cardiac Surgery Differs in Anaemic and Nonanaemic Patients.Anesthesiology. 2011;115(3):523–30. [PubMed] doi: 10.1097/ALN.0b013e318229a7e8.
- Murphy GJ, Reeves BC, Rogers CA, Rizvi SI, Culliford L, Angelini GD. Increased mortality, postoperative morbidity, and cost after red blood cell transfusion in patients having cardiac surgery. Circulation. 2007;116(22): 2544–52. [PubMed][Free Full Text] DOI: 10.1161/CIRCULATIONAHA.107.698977
- Rao SV, Jollis JG, Harrington RA, Granger CB, Newby LK, Armstrong, PW, et al. Relationship of blood transfusion and clinical outcomes in patients with acute coronary syndromes.JAMA. 2004;292(13):1555-62. [PubMed][Free Full Text] doi:10.1001/jama.292.13.1555
- Haase M, Bellomo R, Story D, Letis A, Klemz K, Matalanis G, et al. Effect of mean arterial pressure, haemoglobin and blood transfusion during cardiopulmonary bypass on post-operative acute kidney injury.Nephrol Dial Transplant. 2012;27(1):153–60. [PubMed] [Free Full Text] doi: 10.1093/ndt/gfr275.



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube