
Josef Holzki1
1 Department of Pediatrics, Centre Hospitaliere Universitaire de Liège, Chenée, (Belgium)
Former Head, Department of Pediatric Anesthesia & Surgical Intensive Care, Children´s Hospital, Cologne, (Germany)
Correspondence: Dr. med. Josef Holzki, Beienburger Str. 45, D-51503 Roesrath, (Germany); Tel: +49 2205 8983 546; Fax: +49 2205 8983 548; E-mail: josef.holzki@arcor.de
ABSTRACT
The anatomy of the pediatric larynx has been of great interest to the anesthesiologists and the ENT specialists as there has been a compulsion to use the endotracheal tube (ETT) with the largest possible internal diameter in an effort to minimize the resistance to air flow. The need to calculate the best possible size of ETT in infants and children without any harmful effects, lead to various studies, including autopsies, and radiodiagnostic studies.
Keywords: Pediatric; Larynx; Anatomy;
Citation: Holzki J. How could fundamental disagreements about the correct anatomy of the pediatric larynx develop during the last 15 years? Anaesth Pain & Intensive Care 2018;22(1):5-7
Received – 25 Feb 2018; Reviewed – 27 Feb 2018; Accepted – 5 Mar 2018
The anatomy of the pediatric larynx has been thoroughly investigated and described in the scientific literature since 1897 based on qualified experimental investigations.1 The evidence, that the entrance of the larynx (glottis) was considerably larger than the outlet (cricoid ring), the only circular, cartilaginous, rigid part of the larynx was confirmed in 1936.2 Eckenhoff combined the older findings with his observations during clinical laryngoscopy in 1951 and used for the first time the term “funnel shaped” for describing the lumen of the pediatric larynx.3 This was the scientific basis for sealing the upper airway safely at the level of the circular cricoid outlet with uncuffed tracheal tubes since then till the present time. Using properly selected uncuffed tracheal tubes have the immense advantage of not damaging the mucosa of the larynx when the head of the child is moving.
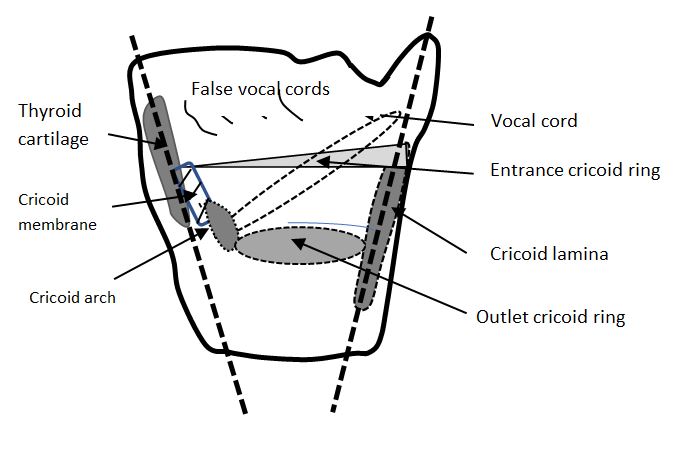
| Figure 1: A-P cross-section of infant larynx (autopsy specimen). The axis of thyroid cartilage, cricothyroid membrane and arch of cricoid forms an oblique line, leaning forward. The lamina of the cricoid ring leans backward. A cylindrical lumen of the larynx, described by CT-scans, must be an artifact4 |
The publication by Eckenhoff was confirmed by decades of practice all over the world and a number of convincing experimental studies since that time (summarized in reference 4), ending in the largest experimental study about the infant larynx in several hundred autopsy specimen by Fayoux et al. in 2006/08.5,6 The authors documented the pronounced distensibility of the structures above the entrance of the cricoid ring which could receive calibration rods and tracheal tubes with considerably larger diameters than could pass through the cricoid outlet. This fact was and is known to all specialists of airway diagnostics (pediatric ENT-surgeons and airway endoscopists), but not to all pediatric anesthesiologists (see below).
In 2009, Dalal et al.7 photographed the glottic level of anesthetized and paralyzed children and found the opening of the glottis smaller than the one of the cricoid outlet. This could have been expected because the authors described the normal finding after muscular blockade of the glottis before intubation, when the flaccid vocal cords have to be lateralized by the beveled tip of tracheal tubes. This is everyday experience of all anesthesiologists. The authors of the article7 did not perceive the distensibility of the laryngeal structures above the cricoid ring and missed the funnel shape of the A-P section of the pediatric larynx as is documented in Figure 1, and in greater detail in a recent, comprehensive review article.4 The photographic and planimetric study7 cannot provide convincing arguments for a cylindrical lumen of the pediatric larynx!
Several studies used magnetic resonance imaging (MRI)8 or CT scans9 to describe the lumen of the pediatric larynx in sedated or anesthetized children and found even more conflicting results, namely a narrower subglottic space than the cricoid outlet, a well-known result in sedated or paralyzed children. But the most surprising finding in these studies was the assertion that an oval shaped cricoid outlet always existed, particularly in infants.9 These findings could not be confirmed in autopsy studies nor in laryngeal surgery nor airway endoscopy.4 A surprising flaw of these radiologic studies was a false reference8 and the omission of an extremely important paper.9
The basic errors in MRI and CT scan investigations of the pediatric larynx can be attributed to the invisibility of the cartilaginous structures and therefore the inability to determine the vertical axis nor the precise plane of cross sections of the lumen of the larynx correctly. Missing the accurate axis and/or the correct plane of the lumen of the larynx, circular planes are depicted as oval structures.
To discuss the conflicting opinions about the anatomy of the pediatric airway in greater detail would disrupt the size of this editorial. But the discussion can be followed in above mentioned extensive review article.4 From this article, in which an attempt was made to analyze the most important articles about the anatomy of the pediatric larynx, an appropriate conclusion can be derived.
If a tracheal tube, advancing via the distensible glottis meets a resistance within the larynx, the resistance is not caused by the vocal cords but by the rigid cricoid ring. The active vocal cords within a surrounding of pliable muscles can never have a smaller lumen than the non-dilatable cricoid ring.
Conflict of interest: None declared by the author
REFERENCES
- Bayeux MR. Tubage du larynx dans le Croup. Auto-Extubation. La presse médicale 1897; 6: 29-33.
- Peter K. Handbuch der Anatomie des Kindes (Handbook of the anatomy of the child). Peter K, Wetzel G, Heiderich F edits. Springer, Berlin 1936; 525-562.
- Eckenhoff JE. Some anatomic considerations of the infant larynx influencing endotracheal anesthesia. Anesthesiology 1951; 12: 401-410. [PubMed] [Free full text]
- Holzki J, Brown KA, Carroll RG, Coté CJ. The anatomy of the pediatric airway: Has our knowledge changed in 120 years? A review of historic and recent investigations of the anatomy of the pediatric larynx. Pediatr Anesth 2018; 18: 13-22. doi: 10.1111/pan.13281. [PubMed] [Free full text]
- Fayoux P, Devisme L, Merrot O, Barciniak B. Determination of Endotracheal Tube Size in a Perinatal Population. Anesthesiology 2006; 104: 954-60. [PubMed] [Free full text]
- Fayoux P, Marciniak B, Devisme L et al. Prenatal and early postnatal morphogenesis and growth of human larygo-tracheal structures. J Anat 2008; 213: 86-92. [PubMed] [Free full text]
- Dalal PG, Murray D, Messner AH, Feng A, McAllister J, Molter D. Pediatric laryngeal dimensions: an age-based analysis. Anesth Analg 2009;108:1475–9. doi: 10.1213/ane.0b013e31819d1d99. [PubMed]
- Litman RS, Weissend EE, Shibata D, Westesson PL. Developmental changes of laryngeal dimensions in unparalized, sedated children. Anesthesiology 2003; 98: 41-5 . [PubMed] [Free full text]
- Wani TM, Rafiq M, Akhter N, AlGhamdi FS, Tobias JD. Upper airway in infants – a computed tomography-based analysis. Paediatr Anaesth. 2017 May;27(5):501-505. [PubMed] [Free full text]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube