
Tomoki Nishiyama, MD, PhD
Department of Anesthesiology, Shinagawa Shishokai Hospital, 1-29-7, Kita-Shinagawa, Shinagawa-ku, Tokyo, 140-0001, (Japan)
Correspondence: Tomoki Nishiyama, MD, PhD, Department of Anesthesiology, Shinagawa Shishokai Hospital, 1-29-7, Kita-Shinagawa, Shinagawa-ku, Tokyo, 140-0001, (Japan); Tel: +81-3-5871-0700; E-mail: nishit-tky@umin.ac.jp
ABSTRACT
Background and aim: Nicardipine and diltiazem, used to decrease blood pressure, have different actions on hemodynamics and hormonal response during inhalational anesthesia. However, there are no studies to compare these effects of nicardipine and diltiazem in propofol-fentanyl-nitrous oxide anesthesia. Therefore, we performed this study to compare the effects of nicardipine and diltiazem on hemodynamics, plasma concentrations of catecholamines and renin-angiotensin-aldosterone activity in propofol-fentanyl-nitrous oxide anesthesia.
Methodology:
Twenty patients scheduled for resection of brain tumors were divided into two groups. Anesthesia was induced with propofol and fentanyl, and maintained with propofol, fentanyl and 67% nitrous oxide and 23% oxygen. During surgery, nicardipine 1 mg or diltiazem 10 mg was administered in one minute. Blood pressure, heart rate, plasma concentrations of epinephrine, norepinephrine, angiotensin I and II, and aldosterone, and plasma renin activity were measured until 30 minutes after administration of nicardipine or diltiazem.
Results:
Blood pressure decreased significantly in both groups (P < 0.05). Heart rate did not change in both groups. Plasma concentrations of epinephrine, norepinephrine, angiotensin I and II, and aldosterone, as well as renin activity did not change in both groups. There were no differences between the two groups in blood pressure, heart rate, plasma concentrations of catecholamine, angiotensin and aldosterone, and renin activity.
Conclusion: During propofol-fentanyl-nitrous oxide anesthesia, there is no difference in the effects between nicardipine and diltiazem on hemodynamics, and plasma concentrations of catecholamines, angiotensin, and aldosterone, and renin activity.
Key words: Propofol; Fentanyl; Nitrous oxide; Catecholamines; Rennin-Angiotensin-Aldosterone; Anesthesia, General
Citation: Nishiyama T. Effects of nicardipine versus diltiazem on catecholamine secretion and renin-angiotensin-aldosterone system during propofol-fentanyl-nitrous oxide anesthesia. Anaesth Pain & Intensive Care 2016;20(1):21-25.
INTRODUCTION
Both nicardipine and diltiazem are calcium antagonists and are used to decrease blood pressure rapidly during general anesthesia; but nicardipine increases,1 while diltiazem decreases2 heart rate. We have already shown that nicardipine and diltiazem administered during general anesthesia had different effects on blood pressure, heart rate, and plasma concentrations of catecholamine and renin-angiotensin-aldosterone in sevoflurane3 and isoflurane4 anesthesia. However, there are no studies to compare the effects of nicardipine and diltiazem of hemodynamics and hormonal changes in intravenous anesthesia.
The present study was performed to compare hemodynamics and plasma concentrations of catecholamine, angiotensin, and aldosterone, and renin activity between nicardipine and diltiazem in propofol-fentanyl-nitrous oxide anesthesia.
METHODOLOGY
The study design was the same as our previous studies.3,4 This study is a non-blind randomized controlled study. After the approval of the Ethical Committee of the hospital and written informed consent from patients, 20 patients, aged 40 to 70 years with ASA physical status I or II, who would undergo resection of brain tumor, were randomly divided into two groups by an envelope method. Those who had cardiac, liver, renal, hormonal, or any metabolic disease (diabetes mellitus, hyper- or hypothyroidism etc.), obesity (body mass index > 30), allergy to diltiazem or nicardipine, or who had drug abuse, were excluded.
No premedication was allowed. Anesthesia was induced with propofol 2 mg/kg and fentanyl 4 µg/kg. Endotracheal intubation was facilitated with vecuronium 0.2 mg/kg. Anesthesia was maintained with propofol 6 mg/kg/h, intermittent fentanyl and 67% nitrous oxide in oxygen. Radial artery was cannulated to measure blood pressure. Lactated Ringers solution was infused to keep urine volume more than 1 ml/kg/h. Mannitol 20% 300 ml was infused at craniotomy. Ventilation was adapted to keep end-tidal carbon dioxide tension between 30 and 35 mmHg.
After microsurgical procedure started and when hemodynamics were stable at ±5% variation for 30 minutes, nicardipine 1 mg or diltiazem 10 mg was administered in one minute. Blood pressure and heart rate were measured at 0, 1, 3, 5, 10, 20, and 30 min, and plasma concentrations of epinephrine, norepinephrine, angiotensin I, angiotensin II, aldosterone, and renin activity were measured at 0, 5, 10, 20, and 30 min, for 30 min after administration of nicardipine or diltiazem.
Plasma concentrations of epinephrine and norepinephrine were measured with high-performance liquid chromatography (HPLC). Plasma concentrations of
angiotensin I and II, and aldosterone, and plasma rennin activity were measured with radioimmunoassay. During 30 min periods of measurements no fentanyl was administered.
Statistical analysis: Data were shown as mean ± standard deviation or number of the patients. Statistical analysis was performed with the chi-square test and factorial analysis of variance (ANOVA) for demographic data, and repeated measures ANOVA for measured parameters followed by Student-Neuman-Keuls test as a post hoc analysis. A p-value < 0.05 was considered to be statistically significant. Power analysis was performed to detect the intra- and inter- group differences of measured parameters with power of 0.90 using the G PowerTM software (University Mannheim, Germany).
RESULTS
By power analysis, 18 patients were necessary, therefore, 20 patients were enrolled. Demographic data and dose of fentanyl used were not different between the two groups (Table 1).
Table 1: Demographic data of the patients
| Parameter | Nicardipine | Diltiazem |
| Age (years) | 56 ± 8 | 56 ± 11 |
| Gender (male/female) | 7/3 | 8/2 |
| Body weight (kg) | 58 ± 10 | 59 ± 6 |
| Height (cm) | 163 ± 8 | 161 ± 6 |
| Duration of surgery (min) | 325 ± 47 | 287 ± 64 |
| Interval between start of surgery and start of the study (min) | 103 ± 15 | 97 ± 18 |
| Total fentanyl dosage at the start of the study (µg) | 328 ± 35 | 353 ± 42 |
Mean ± standard deviation or number of the patients
Blood pressure decreased significantly compared to the value before administration of nicardipine or diltiazem in one minute in both groups and the peak decrease was at 3 minutes in the diltiazem group and at 5 minutes in the nicardpine group (Figure 1-1). Heart rate did not change in both groups (Figure 1-2). Plasma epinephrine (Figure 2-1) and norepinephrine (Figure 2-2) concentrations did not change significantly in both groups. Plasma renin activity (Figure 3-1), angiotensin I (Figure 3-2) and II (Figure 3-3), and aldosterone (Figure 3-4) concentrations did not change significantly in both groups. There were no differences between the two groups in blood pressure, heart rate, plasma concentrations of catecholamine, angiotensin, and aldosterone, and renin activity.
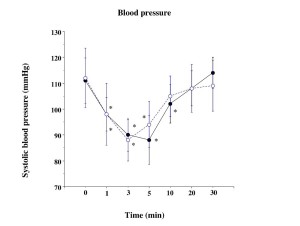
Figure: 1-1
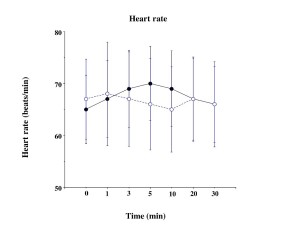
Figure 1: Blood pressure (1-1) and heart rate (1-2)
Mean ± standard deviation; closed circle, nicardipine group; open circle, diltiazem group; *: P < 0.05 vs. nicardipine group; +: P < 0.05 vs. the value at time 0.
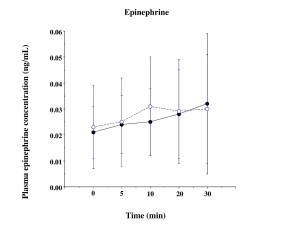
Figure 2-1
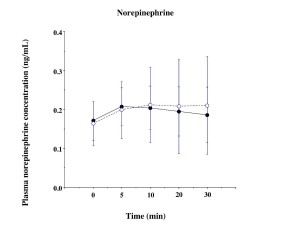
Figure 2-2
Figure 2: Plasma epinephrine (2-1) and norepinephrine (2-2) concentration
Mean ± standard deviation; closed circle, nicardipine group; open circle, diltiazem group; *: P < 0.05 vs. nicardipine group; +: P < 0.05 vs. the value at time 0
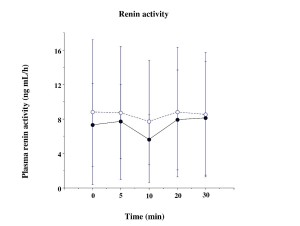
Figure 3-1
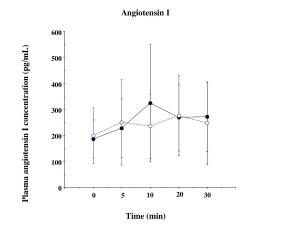
Figure 3-2
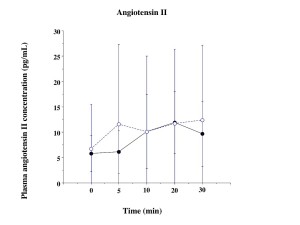
Figure 3-3
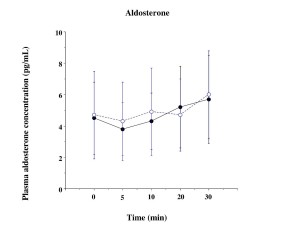
Figure 3-4
Figure 3: Plasma renin activity (3-1), angiotensin I (3-2) and II (3-3) , and aldosterone (3-4) concentrations
Mean ± standard deviation; closed circle, nicardipine group; open circle, diltiazem group
DISCUSSION
The results of our study showed that during propofol-fentanyl-nitrous oxide anesthesia, both nicardipine and diltiazem decreased blood pressure, but did not change heart rate, plasma concentrations of epinephrine, norepinephrine, rennin, angiotensin, and aldosterone. No differences were found between nicardipine and diltiazem in the above measurements.
There are some limitations of this study as shown in our previous study,4 such as this study was conducted at stable hemodynamic state and not at hypertensive state; dose of nicardipine and diltiazem, duration of measurements, and blindness of the study, were similar.
The peak decrease in blood pressure came faster and decrease lasted shorter with diltiazem than nicardipine in the present study. However, nicardipine has faster onset and shorter half-life than diltiazem.5,6 Therefore, the results of the present study might be modified by propofol, fentanyl and nitrous oxide, while we could not find any studies to discuss the reason of the discrepancy between our study and others.5,6
In our previous studies using the same study protocol as the present study, nicardipine increased heart rate and plasma concentrations of epinephrine and norepinephrine in both sevoflurane3 and isoflurane4 anesthesia. Diltiazem decreased heart rate in isoflurane anesthesia4, while did not change heart rate in sevoflurane anesthesia3. Diltiazem did not change plasma concentrations of epinephrine and norepinephrine in both sevoflurane3 and isoflurane4 anesthesia.
No changes of heart rate and plasma concentrations of epinephrine and norepinephrine were observed during propofol-fentanyl-nitrous oxide anesthesia in the present study. Takino et al7 reported that fentanyl inhibited norepinephrine release but not epinephrine at induction of anesthesia. However, Thomson et al8 showed that epinephrine did not change but norepinephrine increased by fentanyl induction. Nitrous oxide decreases epinephrine release and increases norepinephrine secretion.9 Propofol decreased plasma epinephrine concentrations at induction of anesthesia.10 Propofol, fentanyl and nitrous oxide might inhibit the increase of epinephrine and norepinephrine induced by nicardipine and diltiazem.
Nicardipine increases plasma renin activity,11 but did not change plasma aldosterone concentration.12 No changes of renin, angiotensin, and aldosterone concentrations in the present study might be due to the interaction between nicardipine and anesthetics used, while we could not find any studies of the effects of propofol, fentanyl, or nitrous oxide on renin-angiotensin-aldosterone system. Infusion of diltiazem did not affect renin-angiotensin-aldosterone system during droperidol-fentanyl anesthesia.13 Ikeda et al14 also showed no changes in renin secretion by infusion of diltiazem. These are consistent with our results in propofol-fentanyl-nitrous –oxide anesthesia.
CONCLUSION
In conclusion, both nicardipine and diltiazem decrease blood pressure during propofol-fentanyl-nitrous oxide anesthesia, but there is no statistically significant difference between the effects of the two drugs on heart rate, plasma epinephrine and norepinephrine concentrations, and renin-angiotensin-aldosterone system. Therefore, we can use either nicardipine or diltiazem with similar effects to decrease blood pressure in propofol-fentanyl-nitrous oxide anesthesia.
Acknowledgement: We used our department funds and have no conflict of interest.
Conflict of interest: None declared by the author.
REFERENCES
- Turlapaty P, Vary R, Kaplan JA. Nicardipine, a new intravenous calcium antagonist: a review of its pharmacology, pharmacokinetics, and perioperative applications. J Cardiothorac Anesth. 1989 Jun;3(3):344-55. [PubMed]
- Fujimoto T, Peter T, Mandel WJ. Electrophysiologic and hemodynamic action of diltiazem: disparate temporal effects shown by experimental dose-response studies. Am Heart J. 1981 Apr;101(4):403-7. [PubMed]
- Nishiyama T. Effects of nicardipine and diltiazem on catecholamine secretion and renin-angiotensin-aldosterone system during sevoflurane anesthesia. Analg Resusc Curr Res 2014 3:1 doi: 4172/2324-903X.1000110
- Nishiyama T. Effects of nicardipine versus diltiazem on catecholamine secretion and renin-angiotensin-aldosterone system during isoflurane anesthesia. Anaesth Pain & Intensive Care 2014;18(4):332-7. [Free full text]
- Hermann P, Rodger SD, Remones G, Thenot JP, London, DR, Morselli PL. Pharmacokinetics of diltiazem after intravenous and oral administration. Eur J Clin Pharmacol. 1983;24(3):349-52. [PubMed]
- Graham DJ, Dow RJ, Hall DJ, Alexander OF, Mroszczak EJ, Freedman D. The metabolism and pharmacokinetics of nicardipine hydrochloride in man. Br J Pharmacol. 1985;20 Suppl 1:23S-8S. [PubMed] [Free full text]
- Takino Y, Takahashi J, Yamaguchi O, Oh K. The effects of moderate-dose fentanyl-N2O anesthesia on urinary catecholamine excretion during upper-abdominal surgery. Masui. 1984 Oct;33(10):1095-8. [PubMed]
- Thomson IR, Hudson RJ, Rosenbloom, M, Torchia MG. Catecholamine responses to anesthetic induction with fentanyl and sufentanil. J Cardiothorac Anesth. 1988 Feb;2(1):18-22. [PubMed]
- Matsumoto T, Okuda Y, Dobashi Y, Yoshida S. Plasma catecholamine levels during air-oxygen-enflurane anesthesia compared with those during nitrous oxide-oxygen-enflurane anesthesia. Masui. 1992 Nov;41(11):1741-8. [PubMed]
- Mustola ST, Baer GA, Metsa-Ketela T, Laippala P. Haemodynamic and plasma catecholamine responses during total intravenous anaesthesia for laryngomicroscopy. Thiopentone compared with propofol. Anaesthesia 1995;50(2):1008-13.
- Clifton GG, Cook ME, McCarthy P, Bienvenu G, Walsh M, Turlapaty P, et al. Changes of plasma renin activity and atrial natriuretic factor during intravenous nicardipine treatment of severe hypertension. Int J Clin Pharmacol Ther Toxicol 1989;27(12):578-82.
- Baba T, Ishizaki T, Murabayashi S, Aoyagi K, Tamasawa N, Takebe K. Multiple oral dose of nicardipine, a calcium-entry blocker: effects on renal function, plasma renin activity, and aldosterone concentration in mild-to-moderate essential hypertension. Clin Pharmacol Ther. 1987 Aug;42(2):232-9. [PubMed]
- Kono K, Okutani R, Tsuda S, Ishida H, Nakamura H, Philbin DM. Effects of diltiazem on rennin-aldosterone and ACTH-adrenocortical function during upper abdominal surgery. J Clin Anesth. 1990 Nov-Dec;2(6):407-14.[PubMed]
- Ikeda F, Kono T, Oseko F, Imura H, Endo J. Effects of diltiazem hydrochloride on pressor and steroidogenic actions of angiotensins and norepinephrine in man. Endocrinol Jpn. 1980;27(6):779-84. [PubMed]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube