
Cindy Lin, MD1, Nicole Elsey, MD1,2, Marco Corridore, MD1,2, Jon Grischkan, MD3, William E. Shiels II, DO4, Joseph D. Tobias, MD1,2,5
1Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, Columbus, Ohio
2Department of Anesthesiology & Pain Medicine, The Ohio State University
College of Medicine, Columbus, Ohio
3Department of Otolaryngology and Head & Neck Surgery, Nationwide Children’s
Hospital and The Ohio State University, Columbus, Ohio
4Department of Radiology, Nationwide Children’s Hospital, Columbus, Ohio
5Department of Pediatrics, The Ohio State University College of Medicine,
Columbus, Ohio
Correspondence: Joseph D. Tobias, MD, Chairman, Department of Anesthesiology & Pain Medicine, Nationwide Children’s Hospital, 700 Children’s Drive
Columbus, Ohio 43205 (USA); Phone: (614) 722-4200; FAX: (614) 722-4203; E-mail: Joseph.Tobias@Nationwidechildrens.org
ABSTRACT
Branchial cleft anomalies are common congenital head and neck lesions in the pediatric population. Their close proximity to laryngeal structures may lead to airway complications during the diagnosis and management of the lesion. We present an unusual cause of airway compromise secondary to dye extravasation during an interventional radiology procedure for evaluation of a branchial cleft sinus. The diagnosis and treatment of branchial cleft anomalies are reviewed and options presented for the management of airway compromise related to interventions for these anomalies.
Key words: Branchial Arch Syndrome; Branchial Clefts; Branchial Cleft Anomalies; Airway Obstruction; Airway Management
Citation: Lin C, Elsey N, Corridore M, Grischkan J, Shiels WE, Tobias JD. Dye extravasation during radiography for branchial cleft sinus compromising airway in an infant. Anaesth Pain & Intensive Care 2015;19(2):192-95
INTRODUCTION
Branchial cleft anomalies account for approximately 20% of congenital head and neck lesions in infants and children. As they generally lie in the vicinity of laryngeal structures, complications during procedures intended to image the anatomy can lead to airway compromise. We present a report of a 10-month-old child who experienced airway compromise following extravasation of dye during a radiodiagnostic procedure to define the anatomy of a branchial cleft remnant. The diagnosis and treatment of branchial cleft anomalies are reviewed and options presented for the management of airway compromise related to interventions for these anomalies.
CASE REPORT
IRB approval is not required for single patient case reports at Nationwide Children’s Hospital. Our patient was a healthy 10-month-old infant who was subjected to guided contrast injection by interventional radiology for a suspected branchial cleft sinus with diagnostic head and neck magnetic resonance imaging (MRI). The infant was held nil per os for 6 hours and transported to the interventional radiology suite where routine American Society of Anesthesiologists monitors were placed. Anesthesia was induced with sevoflurane in oxygen and nitrous oxide followed by uncomplicated orotracheal intubation with a 3.5 mm cuffed endotracheal tube (ETT). The cuff was inflated to minimize air leak around the ETT. Non-ionic water soluble contrast medium (Optiray 320, Mallinckrodt, Inc, Hazelwood, MO) was then injected into the sinus tract in the neck under fluoroscopy and the patient was transferred to MRI. Guidewire cannulation of the tract was performed by the interventional radiology team to determine if there was a pharyngeal connection, indicating a true branchial fistula. Upon completion of the head and neck MRI, the radiologist reading the scan informed the team that there was extravasated contrast material in the submandibular space, parapharyngeal, and pre-vertebral soft tissues (Figures 1& 2).
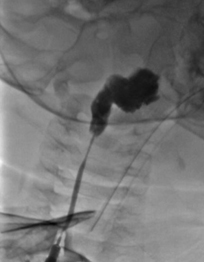
Figure 1: Fluoroscopic imaging demonstrating the sinus tract of the branchial cleft cyst and extravasation of dye
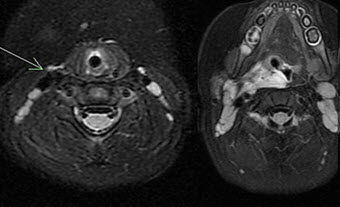
Figure 2: MRI of the neck and oropharynx demonstrating dye in the brachial cleft (arrow). There is also extravasation of contrast material into the submandibular space, parapharyngeal, and prevertebral soft tissue which displacement of the normal tissues
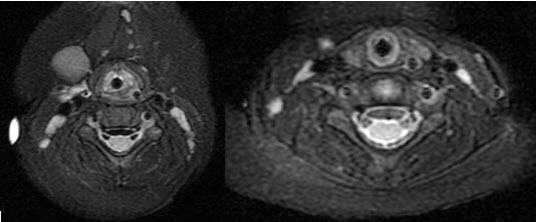
Figure 3: MRI of the neck demonstrating dye around the trachea with mass effect upon the airway which is stented open with the endotracheal tube

Figure 4: A radiograph obtained the next morning. The catheter seen within the brachial cleft sinus. There has been interval reabsorption of the contract material.
The contrast was surrounding the area, causing a mass effect upon the airway. It was reported that the airway was stented open with the ETT (Figure 3). Given these findings and concern for airway patency, the ETT was left in place and the patient was admitted to the Pediatric ICU with continuous sedation. Dexamethasone was administered to minimize airway swelling. A series of radiographs of the neck were obtained to evaluate the reabsorption of the dye. By the next morning, there was no residual dye noted in the neck (Figure 4). The patient was transported to the operating room and a direct laryngoscopy and bronchoscopy was performed to evaluate airway patency. The airway was patent with no residual posterior or lateral pharyngeal wall swelling obstructing the lumen. The patient’s trachea was extubated at that time under direct vision by the pediatric otorhinolaryngologist. The patient was transported back to the Pediatric ICU. There were no further airway concerns. The remainder of his hospital course was unremarkable and he was discharged home on day 3.
DISCUSSION
We present a report of an infant who developed iatrogenic airway compromise from the extravasation of radio-opaque contrast material during the injection of a branchial cleft sinus. Branchial cleft anomalies are common congenital head and neck masses in the pediatric population, accounting for approximately 20% of all congenital head and neck masses.1,2 They are the result of an incomplete obliteration of the pharyngeal clefts and pouches of the branchial apparatus during embryogenesis, presenting as a cyst, sinus, or fistula on the lateral side of the neck.Branchial cleft sinuses and fistulas often present with an external draining pit in the lateral neck during the first decade of life. These commonly present as a painless slow-growing neck mass, which becomes apparent during adolescence.
The diagnosis of branchial cleft anomalies can generally be accomplished primarily by medical history and physical examination alone.2 Definitive treatment involves complete surgical excision to minimize the chance of recurrence.3 Diagnostic imaging (sonography, computed tomography (CT) imaging, magnetic resonance imaging (MRI) and fistulography) can be used to aid surgical planning. Fluoroscopic fistulography using a water-soluble contrast dye to delineate the tract of the fistula or sinus is sometimes performed prior to surgical excision. After confirming the presence of a tract, patients undergo CT or MR imaging to define the extent of the lesion and its relationship to the surrounding structures.
The choice of contrast agent plays a crucial role in the pathogenesis of tissue damage following extravasation injury. A variety of contrast agents are approved for intravascular use with variation in their osmolality. Contrast medium extravasated into the surrounding tissue causes local inflammation and tissue injury that reaches its peak within 24-48 hours of extravasation. The severity of tissue injury is associated with both the osmolality and cytotoxicity of the contrast agent. Toxicity decreases as contrast osmolality approaches serum osmolality (285 mOsm/kg). Non-ionic low-osmolality contrast media (LOCM) are usually better tolerated and have a lower risk of serious adverse complications than ionic high-osmolality contrast media.4,5 Extravasation of LOCM from the site of injection into surrounding tissues most commonly present with mild symptoms such as tissue swelling and skin erythema, but rarely may cause tissue necrosis and severe skin ulceration.6,7
Although we could not find previous reports of dye extravasation as occurred in our patient, it is logical that such issues may occur with the injection of dye into a fistula tract and its extravasation into the soft tissues of the neck surrounding the airway. In our patient, a non-ionic LOCM with an osmolality of 702 mOsm/kg was used. Despite its low osmolality, a mass effect occurred related to the contrast and the surrounding tissue injury which subsequently resulted in iatrogenic airway compromise. Imaging demonstrated extravasation of the contrast material into the submandibular space, parapharyngeal and prevertebral soft tissues, causing mass effect upon the airway. The mass effect was likely exacerbated by the high osmolality of the dye with the transudation of fluid into these spaces.
As was the case in our patient, the diagnostic imaging of a branchial cleft anomaly in the pediatric patients often requires general anesthesia to minimize anxiety, control pain, and prevent movement. In many cases, this imaging is performed by contrast injection in the interventional radiology suite after the induction of general anesthesia. Given the type and duration of the procedure, these cases are frequently accomplished with spontaneous ventilation and a laryngeal mask airway (LMA). Given the proximity of branchial cleft lesions to laryngeal structures and the possibility of airway complications during these procedures, we would recommend consideration of performing such cases with an endotracheal tube in place. As illustrated by our patient, the ETT will stent the airway open until there is resolution of the mass effect.
Treatment of airway compromise in this scenario should include leaving the ETT in place to maintain patency of the airway. Patients with airway compromise should be monitored in the ICU under continuous sedation and with an appropriate pain control regimen. The patient should be given a course of intravenous corticosteroids to mitigate airway edema. Attempts at aspiration of extravasated dye have not been consistently shown to reduce complications associated with extravasation and may increase the risk of more trauma and infection.8 Serial radiographic imaging should be obtained to monitor the progression of dye absorption. Given that contrast extravasation may cause tissue necrosis and possible injury to the airway, we would also recommend direct laryngoscopy and bronchoscopy by the otorhinolaryngologist to visually inspect the airway prior to tracheal extubation.
Most importantly, effective communication is essential between all healthcare providers involved in the care including the radiologist, otorhinolaryngologist, and anesthesiologist regarding findings on imaging modalities. This case presents a near miss that could have resulted into a “can’t intubate – can’t ventilate” scenario, had the radiologist not alerted the anesthesia provider and surgeon to the dye extravasation. Although contrast extravasation is uncommon, its potential airway complications may lead to a change in practice including the use of an ETT over an LMA for these procedures.
REFERENCES
- Waldhausen, JH. Branchial cleft and arch anomalies in children. Semin Pediatr Surg 2006;15:64-69.
[PubMed] - Goff CJ, Allred C, Glade RS. Current management of congenital branchial cleft cysts, sinuses, and fistulae. Curr Opin Otolaryngol Head Neck Surg 2012;20:533-539
[PubMed] doi: 10.1097/MOO.0b013e32835873fb. - Glosser JW, Pires CA, Feinberg SE. Branchial cleft or cervical lymphoepithelial cysts: etiology and management. J Am Dent Assoc 2003;134:81-86.
[PubMed] - Cohan RH, Leder RA, Bolick D, Herzberg AJ, Hedlund LW, Wheeler CT, et al. Extravascular extravasation of radiographic contrast media. Effects of conventional and low-osmolar agents in the rat thigh. Invest Radiol 1990;25:504-510.
[PubMed] - Rubin JD, Cohan RH. Iodinated radiographic contrast media: comparison of low-osmolar with conventional ionic agents. Curr Opin Radiol 1991;3:637-645.
[PubMed] - Wang CL, Cohan RH, Ellis JH, Adusumilli S, Dunnick NR. Frequency, management, and outcome of extravasation of nonionic iodinated contrast medium in 69,657 intravenous injections. Radiology 2007;243:80-87.
[PubMed][Free full text] - Tonolini M, Campari A, Bianco R. Extravasation of radiographic contrast media: prevention, diagnosis, and treatment. Curr Probl Diagn Radiol 2012;41(2):52-55.
[PubMed] doi: 10.1067/j.cpradiol.2011.07.004. - Bellin MF, Jakobsen JA, Tomassin I, Thomsen HS, Morcos SK, Thomsen HS, et al. Contrast medium extravasation injury: guidelines for prevention and management. Eur Radiol 2002;12:2807-2812.
[PubMed]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube