
Nishith Govil, MBBS, MD1, Shalini Dadu, MBBS, MD2, Virender P Singh, MBBS, MS3, Vinay Rai, MBBS, MD3, Parag Kumar, MBBS, MD1
1Assistant Professor, 2Associate Professor
Department of Anesthesiology, Shri Guru Ram Rai Institute of Medical & Health Science
(SGRRIH&MS), Patel Nagar, Dehradun (india)
Professor, Department Of Otolaryngology, Shri Guru Ram Rai Institute of Medical & Health Science, (SGRRIH&MS), Patel Nagar, Dehradun (india)
Correspondence: Dr Nishith Govil, House No. 707, Street 4, Lane 5, Rajendra Nagar, Dehradun-Pin 248001, Uttarakhand (India); Cell: +91-8126101759; E-mail: nishithgovil@rediffmail.com
ABSTRACT
Objectives: Sympatholytic properties of dexmedetomidine have many advantages to use in general anesthesia especially in pediatric age group undergoing cochlear implant surgeries. This study is designed to compare the effects of bolus dose of dexmedetomidine followed by infusion with placebo in cochlear implant surgeries for quality of hypotensive anesthesia with hemodynamic stability and incidence of complications in pediatric age group particularly emergence delirium with sevoflurane.
Methodology: 60 pediatric patient of ASA grade I or II with congenital or acquired deafness of age ranging from 2 to 8 years scheduled for cochlear implant surgery were included in this study.
Group D were administered dexmedetomidine 0.5 μg/kg in 100 ml 0.9% NaCI over 10 min followed by infusion of dexmedetomidine at 0.5 μg/kg/h and Group P was given placebo only i.e. 0.9% NaCl 100 ml over 10 min followed by infusion at 2 ml/h. Heart rate (HR) and mean arterial pressure (MAP) at different time interval, intraoperative fentanyl and propofol consumption, surgeons’ satisfaction score and complications, particularly incidences of emergence delirium were recorded.
Statistical analysis: Mean with standard deviation of various parameters of both groups was compared using student’s t test were analyzed.
Results: statistical significant lowering of MAP, HR, opioid consumption and rate of complications were lower in dexmedetomidine group compared to placebo group.
Conclusion: Intraoperative administration of dexmedetomidine provides better surgical field and subsequently higher surgeon’s satisfaction score leading to reduced surgery time with better recovery profile.
Keywords: Dexmedetomidine; Cochlear implant; Pediatric patients; Dexmedetomidine
Citation: Govil N, Dadu S, Singh VP, Rai V, Kumar P. Dexmedetomidine improves surgical field in cochlear implant surgery: a randomized, double-blind, placebo-controlled trial. Anaesth Pain & Intensive Care 2017;21(2):147-153
Reviewed: 26 Jan, 16 Feb 2017,
Corrected: 17 Feb 2017
Accepted: 8 Mar 2017
INTRODUCTION
Dexmedetomidine is an active isomer of medetomidine and an agonist at α2 –adrenoceptors that causes sedation without respiratory depression leading to its increasing use in critical care for sedation and in minor surgical procedures as a sole anesthetic agent.1 It has many uses as adjuvant in anesthesia in adults though there are few studies to substantiate its role in pediatric age group. One review concludes that dexmedetomidine provides perioperative analgesia thus decreasing opioid requirement, reduced pain scores and postoperative nausea and vomiting (PONV).2,3 Dexmedetomidine is also used to decrease stress response to laryngoscopy, lowers intra ocular pressure and as an agent for controlled hypotension in FESS surgeries. 4,5 In a large number of studies dexmedetomidine has been used successfully to prevent emergence delirium and postoperative shivering in children.6,7 A 2013 meta-analysis of various trials done proved that pharmacokinetics and dose effects of dexmedetomidine are similar in pediatric age group as seen in adults.8
Recently large numbers of cochlear implantations are done in pediatric age group due to better outcomes, as well as availability of newer anesthetic adjuvants and hemodynamic monitoring. The anesthesia management in cochlear implantation requires a balanced approach so as to provide a stable intraoperative hemodynamics and fewer postoperative complications like sedation, emergence delirium and postoperative pain.9 Good results in this surgery are obtained by providing bloodless surgical field with controlled hypotension.10
This study was designed to compare the effects of adding a bolus dose of dexmedetomidine followed by infusion, with placebo for hypotensive anesthesia in pediatric age group undergoing cochlear implant surgery. Perioperatively, we compared the amount of fentanyl consumption and the incidence of emergence delirium and other complications.
METHODOLOGY
60 pediatric patient of physical status ASA classes I or II (with hemoglobin 8- 10 gm%) with congenital deafness, ages 2 to 8 years, scheduled for cochlear implant surgery over a period of 1 year were included in this prospective, randomized, double blind study after taking due approval from the ethical committee of our institution.
Informed and explained consent about the method of anesthesia was taken from the parents, preoperative assessment was done and children were screened for any exclusion criteria. Children with cardiac anomalies, sinus bradycardia and atrioventricular block, QTc interval > 440 ms, severe milestone delay, seizure disorders, neuromuscular disorder, hepatic impairment and on drugs for any chronic ailment, were excluded from the study.
After keeping NPO for 6 hours patients were given 0.5 mg/kg oral midazolam preoperatively before taking to the induction room where patients were attached to electrocardiogram, non-invasive blood pressure and pulse oximetry with a multichannel monitor (Datex-Ohmeda, Cardiocap/5, GE healthcare, Helsinki, Finland). Separate intravenous lines were secured for giving maintenance fluid and test drug after induction with 4-8 % v/w of sevoflurane in 100% oxygen, fentanyl 3 μg/kg and intubation was facilitated with rocuronium 0.6 mg/kg. Anesthesia was maintained with oxygen and nitrous oxide mixture with sevoflurane concentration adjusted to keep mean arterial pressure (MAP) and heart rate (HR) within the range of 20% of baseline. Further doses of rocuronium were not given till fascial nerve was identified by surgeon after which rocuronium 0.1 mg/kg was given for muscle relaxation. Hypothermia was avoided by heated air blanket and warm RL at 10 ml/kg/hr as maintenance fluid. Just before completion of surgery paracetamol rectal suppository 20 mg/kg and IV ondansetron 0.1 mg/kg were given. Muscle relaxation was reversed with neostigmine/ glycopyrrolate and sevoflurane was stopped at completion of surgery with patient extubated in a deeper plane of anesthesia. In the post anesthesia care unit (PACU) children were monitored for any pain using objective pain scores (OPS) (Table 1), sedation or agitation using Pediatric Anesthesia Emergence Delirium (PAED) scoring system (Table 2).
Table 1: Objective pain score 11 for postoperative assessment of pain in children
| Parameter | Score | |
| Systolic blood pressure | < 20% of baseline | 0 |
| 20-30 % of baseline | 1 | |
| 30% of baseline | 2 | |
| Crying | Not crying | 0 |
| Crying but responds to age-appropriate nurturing | 1 | |
| Does not respond to nurturing | 2 | |
| Movements | No movement relaxed | 0 |
| Restless ( moving constantly) | 1 | |
| Thrashing (moving wildly) | 2 | |
| Agitation | Asleep or calm | 0 |
| Can be comforted to lessen the agitation (mild) | 1 | |
| Cannot be comforted (hysterical) | 2 | |
| Complain of pain | Asleep or states no pain | 0 |
| Cannot localize | 1 | |
| Localizes pain | 2 | |
Table 2: Pediatric Anesthesia Emergence Delirium (PAED scale) 12
| Clinical status | Not at all | Just a little | Quite a bit | Very much | Extremely |
| The child makes eye contact with the care giver | 4 | 3 | 2 | 1 | 0 |
| The child’s actions are purposeful | 4 | 3 | 2 | 1 | 0 |
| The child is aware of his/her surroundings | 4 | 3 | 2 | 1 | 0 |
| The child is restless | 0 | 1 | 2 | 3 | 4 |
| The child is inconsolable | 0 | 1 | 2 | 3 | 4 |
Dexmedetomidine infusion was prepared by a nursing assistant (not involved in the study) in a concentration of 4 μg/ml in a 50 ml syringe and another nursing assistant who was not aware of the content of the syringe started the infusion with a syringe pump (SP102, Larsen and toubro Ltd). 60 children were randomly assigned equally into two groups- Group D and Group P using a computer generated randomization sequence for the study. Demographic profile of patient with regard to age, sex, weight and ASA grade were recorded. After intubation, Group D participants were administered dexmedetomidine (Dextomid, Neon Laboratories) 0.5 μg/kg diluted in 100 ml 0.9% NaCI over 10 min followed by infusion of dexmedetomidine at 0.5 μg/kg/hr. Group P was given normal saline as placebo 100 ml over 10 min followed by infusion at 2 ml hr. The surgeon assessing the quality of surgical field and the anesthetist recording the hemodynamic variables and other measurement of the participants were blinded to the study.
Glycopyrrolate at 10 μg/kg was given if heart rate fell below 60/min and IV mephenteramine 0.5 mg was given if MAP went below 50 mmHg or < 30% of baseline. Fentanyl 0.5 μg/kg and propofol 2 mg/kg both were given if HR and MAP rose above 30% of baseline. Infusion of test drug was stopped 15-20 min prior to the conclusion of surgery. IV fentanyl 0.25 µg/kg was given OPS > 4 and IV ondansetron 0.1 mg/kg were used for any episode of nausea and vomiting in PACU.
Baseline HR and MAP, immediately after intubation (before starting bolus of study drug), 5 min after starting of bolus dose and thereafter at different time interval till patients were discharged from PACU. Intraoperatively fentanyl consumption, total duration of surgery and surgeons satisfaction score based on surgical site bleeding every 15 min after start of surgery was recorded. In the PACU modified Aldrete score, OPS and PAED score immediately on arrival, 30, 60, 90 and 120 min after extubation were recorded. Any episodes of shivering, total amount of rescue analgesia, PONV, hypotension, bradycardia or any other complication were recorded.
Statistical analysis: All the data was expressed as arithmetic mean ± SD, ranges, numbers and percentages as appropriate at various time intervals. Statistical analysis was performed for 2 groups utilizing Statistical Program for Social Science Data version 23 (letter no SGRR/MC/PO/LiB/2015/-11164; License code e27995dcb17243a98de5). Comparisons between the hemodynamic variables, duration of surgery and fentanyl consumption were made between the two groups using student’s t-test. Comparison of Aldrete score, OPS and PAED score were made with Mann-Whitney U test; Chi-square test was used to compare Surgeons Satisfaction Score based on bleeding at the surgical site. Fisher’s exact test was used to compare any episode of complication like bradycardia, hypotension, shivering and PONV. To compare variables at different time intervals from baseline within the group, repeated measures ANOVA was used. Significant difference is considered when value of p < 0.05. The main measured variable was intraoperative Surgeons Satisfaction Score which should be 2 to 3 with SD close to 1.1, the sample size was determined to be 30 patients per group at an α error margin of 0.05, β value of 0.95, and 10% dropout rate to be able to reject the null hypothesis.
RESULTS
All the enrolled 6o patients completed the study. The demographic profile of two groups was similar in age, sex, weight, baseline HR and MAP (p > 0.05) (Table 3). With regards to HR statistical difference existed between Group D and Group P at all time intervals (p < 0.05) till the time of extubation (Figure 1) and in PACU. Significant fall in HR is seen in Group D at 15, 20, 25, 30, 60, 75, 90 min after induction from baseline and 10, 30, 60 min after extubation. MAP was significantly lower in Group D than in Group P at 15, 20, 25, 30, 45, 60, 75, 90 and 105 min after induction from baseline and at 30 min after extubation (Figure 2). Consumption of fentanyl and propofol was significantly high in Group P compared to Group D (Table 3) while Surgeons Satisfaction Score and surgical field remain significantly better in Group D compared to Group P at 15, 30, 60, 75 min after start of surgery while OPS remain significantly low in Group D at 30 and 60 min after extubation while incidence of postoperative delirium was significantly more in Group P (Table 4). Incidence of postoperative complications were very low in dexmedetomidine group (Table 5).
Table 3: Comparison of demographic profile and baseline variables expressed as mean ± standard deviation.
| Variable | Group D
(n=30) |
Group P
(n=30) |
p-value |
| Age (in years) | 3.18 ± 0.72 | 3.22 ± 0.86 | 0.55 |
| Sex (M:F) | 16:14 | 15:15 | 0.76 |
| Weight (kg) | 12.96 ± 1.88 | 13.39 ± 1.68 | 0.95 |
| Peri-operative fentanyl consumption | 40.81 ± 7.34 | 58.12 ± 7.27 | 0.02 |
| Intraoperative propofol consumption | 24.68 ± 6.34 | 42.24 ± 6.22 | 0.01 |
| Baseline heart rate (beats/min) | 121.5 ± 3.38 | 120.94 ± 3.99 | 0.65 |
| Baseline mean arterial pressure (mmHg) | 75.88 ± 2.87
|
76.44 ± 1.75 | 0.35 |
| Duration of surgery | 112 ± 0.27 | 130 ± 4.95 | 0.00 |
Group D, Dexmedetomidine group; Group P, placebo group. Data is expressed as Mean ± SD. P values calculated using Student’s t-test and p<0.05 is shown in bold.
Table 4: Comparison of surgical score (SS), objective pain score (OPS), emergence agitation score (EAS) and Aldrete Score (AS) at various times interval.
| Parameter | Group D
(n=30) |
Group P
(n=30) |
p-value |
| SS at 15 min | 1.25 ± 0.45 | 1.94 ± 0.25 | 0.00 |
| SS at 30 min | 1.62 ± 0.50 | 2.06 ± 0.57 | 0.02 |
| SS at 45 min | 1.72 ± 0.34 | 2.87 ± 0.34 | 0.30 |
| SS at 60 min | 2.10 ± 0.42 | 3.26 ± 0.44 | 0.01 |
| SS at 75 min | 1.31 ± 0.61 | 2.87 ± 0.50 | 0.03 |
| SS at 90 min | 1.84 ± 0.57 | 1.87 ± 0.52 | 0.50 |
| SS at 105 min | 1.26 ± 0.51 | 1.25 ± 0.45 | 0.63 |
| OPS on arrival | 4.2 ± 0.7 | 7.9 ± 0.3 | 0.01 |
| OPS at 30 min | 2.0 ± 0.3 | 5.4 ± 0.8 | 0.03 |
| OPS at 60 min | 2.4 ± 0.6 | 4.9 ± 0.6 | 0.01 |
| OPS at 90 min | 6.2 ± 0.9 | 6.7 ± 0.9 | 0.78 |
| OPS at 120 min | 2.4 ± 0.6 | 2.1 ± 0.6 | 0.54 |
| PAED on arrival | 7.1 ± 0.3 | 13.4 ± 0.7 | 0.00 |
| PAED at 30 min | 10.6 ± 0.4 | 16.6 ± 0.8 | 0.01 |
| PAED at 60 min | 8 ± 0.2 | 14.8 ± 0.4 | 0.00 |
| PAED at 90 min | 13.9 ± 0.4 | 14.6 ± 0.2 | 0.56 |
| PAED at 120 min | 5.0 ± 0.5 | 8.3 ± 0.6 | 0.66 |
Group D, Dexmedetomidine group; Group P, placebo group. Data is expressed as Mean ± SD. P values calculated using Mann Whitany U test and p<0.05 is shown in bold.
Table 5: Incidence of complications [n]
| Complication | Group D | Group P |
| Shivering | 2 | 6 |
| PONV | 1 | 8 |
| Hypotension | 1 | 1 |
| Bradycardia | 5 | 2 |
| Emergence agitation (PAED Score >16) | 1 | 12 |
| Dry mouth | 5 | 2 |
Values are expressed as number of patients. Bradycardia (HR<60) episodes occur intraoperatively
Figure 1: Comparison of heart rate (HR) at various time intervals
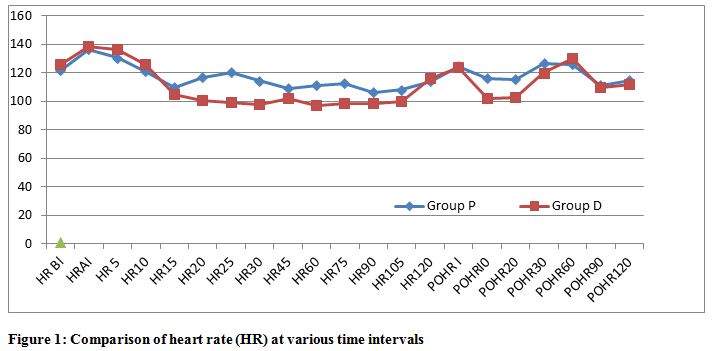
Significant difference (P value <0.05) is observed at HR15, HR20, HR25, HR30, HR60, HR75, POSTOPERATIVELY AT PO10, PO30. Significant difference is observed if P value is <0.05 (Student’s t test). HR BI= heart rate before induction, HR AI= heart rate after induction, POHR 10 = 10 mins after extubation
Figure 2: Shown here comparison of mean arterial pressure (MAP) at various time intervals
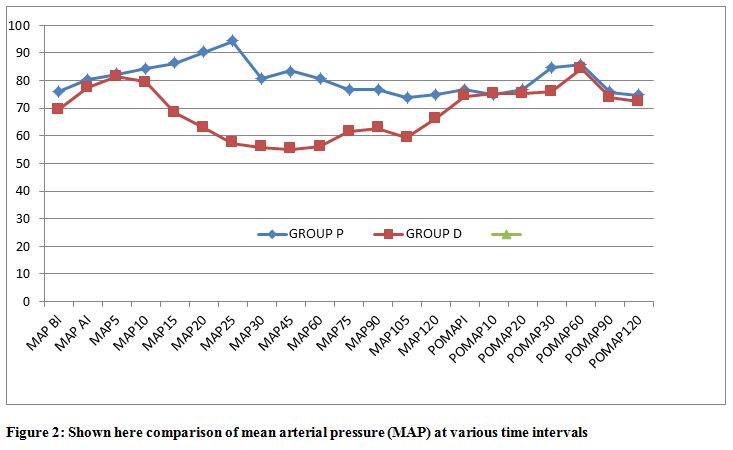
Significant difference (p <0.05) is observed after starting of test drug at MAP15, MAP20, MAP25, MAP30, MAP45, MAP60, MAP75, MAP90, MAP105 AND Postoperatively (PO) at PO30 using Student’s t test. MAP BI= mean arterial pressure before induction, MAP AI= mean arterial pressure after induction
DISCUSSION
In many studies dexmedetomidine is given for sedative, amnestic, and analgesic properties in a bolus dose of < 0.5 μg/kg in pediatric patient to avoid bradycardia giving further infusion dose with titrated response with a maximum dose of 2 μg/kg/hr. At these doses in children Dexmedetomidine acts as an effective sedative and analgesic agent without any significant hemodynamic effects. 13, 14
Bloodless surgical field in surgery is dependent mainly on two factors surgical technique and patient profile with regards to coagulation and hemodynamic parameters namely HR and MAP. Dexmedetomidine has been used successfully as an agent for providing controlled hypotension and bloodless surgical field in endoscopic sinus surgeries, middle ear and spine surgeries.15 Bloodless surgical field is achieved by dexmedetomidine due to lowering in MAP that has been compared to various other agents used for controlled hypotension.16 However, peripheral vasoconstriction due to postsynaptic α2b receptors leads to transient hypertension which is usually observed after starting higher loading doses i.e. > 1 μg/kg.17 In our study no episode of hypertension (MAP > 30% of baseline) is seen in either of the group. However, in 5 patients of Group D significant bradycardia i.e. (HR < 30% of baseline or < 60 bpm) develops after 15-20 min of giving the bolus test drug which when treated with glycopyrrolate 10 μg/kg IV, immediately led to raising of MAP and HR. Such episodes of bradycardia may be due to decrease in sympathetic outflow or due to reflex slowing of HR secondary to transient increase in MAP after the bolus dose of dexmedetomidine. Mason et al.18 reported 3 cases where anticholinergics used for dexmedetomidine induced bradycardia led to exaggerate hypertensive response. According to them and Buck ML19, bradycardia induced by dexmedetomidine should not be treated with anticholinergics, unless bradycardia induced by dexmedetomidine is coincident with hypotension, which is unresponsive to fluids.
Significant fall in MAP from baseline is seen in all time intervals in Group D as compared to Group P which may be the reason for the optimal surgical condition with significant low bleeding scores seen in Group D as compared to Group P. Fentanyl and propofol consumption used for maintenance is significantly high in Group P which has been substantiated in a similar study by El Saied et al. who concluded that recovery time was significantly shorter with dexmedetomidine group with reduced requirement of fentanyl in PACU.20
Shams T21 conducted a study to compare dexmedetomidine and esmolol in functional endoscopic sinus surgery to provide bloodless surgical field. They found that both dexmedetomidine and esmolol provides equal surgeons satisfaction score but dexmedetomidine have additional benefit in terms of postoperative analgesia with opioid sparing effect. In our study in pediatric age group dexmedetomidine also provided added benefits of reducing emergence agitation, postoperative shivering and nausea vomiting. In PACU, patients achieved modified Aldrete score of >=9 in Group D compared to placebo Group early and consequently have shorter stay in PACU. The mechanism of action of dexmedetomidine for analgesia was studied in detail by various authors who found that interaction of dexmedetomidine with α2A and α2C receptor in the spinal cord led to modulation of pain in the descending noradrenergic pathways and affect release of endogenous opioids.22
Emergence delirium is a distressing problem seen in pediatric patient after receiving sevoflurane anesthesia that delays recovery from PACU. Various theories have been postulated for emergence delirium with pain as one of the main causative factor and therefore IV fentanyl is the preferred drug to decrease agitation.23 Alternative nonpharmacological and pharmacological methods including dexmedetomidine have been used successfully to prevent emergence delirium in various studies.24 In our study also 12 patients in placebo group showed incidences of agitation after arrival in PACU with average onset time of agitation being between 10 to 15 min. Use of fentanyl, considerably reduces severity and score of agitation but invariably adds to nausea and vomiting.
Other common adverse events of dexmedetomidine are bradycardia and dry mouth. Bradycardia is due to increase sinus node recovery times and AV nodal effective refractory periods25 especially when co administering drugs causing bradycardia or doing maneuvers causing vagal stimulation like intubation. Easly26 reported the efficacy of dexmedetomidine in reducing postoperative shivering in children by reducing the threshold for shivering. In our study also shivering was less in children receiving dexmedetomidine. No other incidence of hypoxia or any respiratory complication was observed with dexmedetomidine in PACU which was consistent with its safety profile in the study by Koroglu A.27
LIMITATIONS
The limitation of our study was that the monitoring of quality of the surgical field visualization was done with a subjective scoring system and we depended upon the assessment by the operating surgeon for this. Further, we did not use laser Doppler flowmetry to evaluate blood supply to the implant site, that would have added to the authenticity of the observation in a measurable method.
CONCLUSION
The main findings of our study are: intraoperative dexmedetomidine provides controlled hypotension, better surgical field and higher surgeon’s satisfaction score leading to reduced surgery time. Dexmedetomidine significantly reduces consumption of propofol and fentanyl to achieve hemodynamic stability. Compared to placebo, dexmedetomidine provides better recovery profile and lower incidence of postoperative complications like emergence agitation, postoperative pain and nausea/vomiting.
Conflict of interest: No conflict of interest declared. This research was carried out without any externa; source of funding.
Authors’ Contribution: NG-Conduction of study work; SD-Conceptualized idea of the study; VPS-Conduction of clinical cases; VR-Manuscript edition; PK-Statistical analysis.
REFERENCES
- Afonso J, Reis F. Dexmedetomidine: current role in anesthesia and intensive care. Rev Bras Anestesiol. 2012 Jan-Feb; 62(1):118-33. doi: 10.1016/S0034-7094(12)70110-1. [PubMed]
- Gurbet A, Basagan-Mogol E, Turker G, Ugun F, Kaya FN, Ozcan B. Intraoperative infusion of dexmedetomidine reduces perioperative analgesic requirements. Can J Anaesth. 2006 Jul;53(7):646–52. [PubMed]
- Patel A, Davidson M, Tran MC, Quraishi H, Schoenberg C, Sant M, et al. Dexmedetomidine infusion for analgesia and prevention of emergence agitation in children with obstructive sleep apnea syndrome undergoing tonsillectomy and adenoidectomy. Anesth Analg. 2010 Oct;111(4):1004–10. doi: 10.1213/ANE.0b013e3181ee82fa[PubMed]
- Banga PK, Singh DK, Dadu S, Singh M. A comparative evaluation of the effect of intravenous dexmedetomidine and clonidine on intraocular pressure after suxamethonium and intubation. Saudi J Anaesth. 2015;9:179-83. [Free full text]
- Richa F, Yazigi A, Sleilaty G, Yazbeck P.. Comparison between dexmedetomidine and remifentanil for controlled hypotension during tympanoplasty. Eur J Anaesthesiol. 2008 May;25(5):369-74. doi: 10.1017/S0265021508003761 [PubMed]
- Isik B, Arslan M, Tunga AD, Kurtipek O. Dexmedetomidine decreases emergence agitation in pediatric patients after sevoflurane anesthesia without surgery. Paediatr Anaesth. 2006 Jul;16(7):748–53. [PubMed]
- Liu ZX, Xu FY, Liang X, Zhou M, Wu L, Wu Jr, et al. Efficacy of dexmedetomidine on postoperative shivering: a meta-analysis of clinical trials.Can J Anaesth.2015 Jul; 62(7):816-29. doi: 10.1007/s12630-015-0368-1[PubMed] [Free full text]
- Schnabel A, Reichl SU, Poepping DM, Kranke P, Pogatzki-Zahn EM, Zahn PK. Efficacy and safety of intraoperative dexmedetomidine for acute postoperative pain in children: a meta-analysis of randomized controlled trials. Paediatr Anaesth. 2013 Feb; 23(2):170–9. doi: 10.1111/pan.12030. [PubMed]
- Bajwa SJ, Kulshrestha A. The cochlear implantation surgery: A review of anesthetic considerations and implications. Int J Health Allied Sci. 2013;2:225-9. [Free full text]
- Amin SM, Lemay MGE. Optimizing surgical field during cochlear implant surgery in children: Dexmedetomidine versus esmolol. Egypt J Anaesth 2016; 32:255-61.
- Hannallah RS, Broadman LM, Belman AB, Abramowitz MD, Epstein BS. Comparison of caudal and ilioinguinal/iliohypogastric nerve blocks for control of post-orchiopexy pain in pediatric ambulatory surgery. Anesthesiology. 1987 Jun;66(6): 832-834. [PubMed] [Free full text]
- Sikich N, Lerman J. Development and psychometric evaluation of the paediatric anesthesia emergence delirium scale. Anesthesiology. 2004 May;100(5):1138–45. [PubMed] [Free full text]
- Hall JE, Uhrich TD, Barney JA, Arain SR, Ebert TJ. Sedative, amnestic, and analgesic properties of small-dose dexmedetomidine infusions. Anesth Analg. 2000 Mar;90(3):699-705. [PubMed]
- Schnabel A, Meyer-Friebem CH, Reichl SU, Zahn PK, Pogatzki-Zahn EM. Is intraoperative dexmedetomidine a new option for postoperative pain treatment? A meta-analysis of randomized controlled trials. Pain. 2013 Jul;154(7):1140-9. doi: 10.1016/j.pain.2013.03.029[PubMed]
- Akkaya A, Tekelioglu UY, Demirhan A, Bilgi M, Yildiz I, Apuhan T, Kocoglu H. Comparison of the effects of magnesium sulphate and dexmedetomidine on surgical vision quality in endoscopic sinus surgery: randomized clinical study. Rev Bras Anestesiol 2014; 64: 406–412. [Free full text]
- Le Bot A, Michelet D, Hilly J, Maesani M, Dilly MP, Brasher C, et al. Efficacy of intraoperative dexmedetomidine compared with placebo for surgery in adults: a meta-analysis of published studies. Minerva Anestesiol. 2015 Oct;81(10):1105–17. [PubMed]
- Mason KP, Zurakowski D, Zgleszewski S, Prescilla R, Fontaine PJ, Dinardo JA. Incidence and predictors of hypertension during high-dose dexmedetomidine sedation for pediatric MRI. Paediatr Anaesth. 2010 Jun;20(6):516– 523. [PubMed]
- Mason KP, Zgleszewski S, Forman RE, Stark C, DiNardo JA. An exaggerated hypertensive response to glycopyrrolate therapy for bradycardia associated with high-dose dexmedetomidine. Anesth Analg. 2009 Mar;108(3):906–08. [PubMed]
- Buck Dexmedetomidine use in pediatric intensive care and procedural sedation. J Pediatr Pharmacol Ther. 2010 Jan;15(1):17–29. [PubMed] [Free full text]
- El Saied MH, Mohamed NN, Amin MI. Dexmedetomidine versus fentanyl in anesthesia of cochlear implantation in pediatric patients. Egypt J Anaesth.2016; 32:55-59
- Shams T, EL Bahnasawe NS, Abu-Samra M, El Mesry R. Induced hypotension for functional endoscopic sinus surgery: a comparative study of dexmedetomidine versus esmolol. Saudi J Anaesth. 2013 Apr;7(2):175-80. doi: 10.4103/1658-354X [PubMed] [Free full text]
- Fairbanks CA, Stone LS, Kitto KF, Nguyen HO, Posthumus IJ, Wilcox GL. Alpha(2c)-Adrenergic receptors mediate spinal analgesia and adrenergic-opioid synergy. J Pharmacol Exp Ther. 2002 Jan;300(1):282-90. [PubMed] [Free full text]
- Dahmani S, Stany I, Brasher C, Lejeune C, Bruneau B, Wood C, et al.. Pharmacological prevention of sevoflurane- and desflurane-related emergence agitation in children: a meta-analysis of published studies. Br J Anaesth. 2010 Feb;104(2):216-223. doi: 10.1093/bja/aep376[PubMed] [Free full text]
- Pickard A, Davies P, Birnie K, Beringer R. Systematic review and meta-analysis of the effect of intraoperative α₂-adrenergic agonists on postoperative behavior in children. Br J Anaesth. 2014 Jun;112(6):982-90. doi: 10.1093/bja/aeu093 [PubMed] [Free full text]
- Hammer GB, Drover DR, Cao H, Jackson E, Williams GD, Ramamoorthy C, et al. The effects of dexmedetomidine on cardiac electrophysiology in children. Anesth Analg. 2008 Jan;106(1):79-83. doi: 10.1213/01.ane.0000297421.92857.4e [PubMed]
- Easley RB, Brady KM, Tobias JD. Dexmedetomidine for the treatment of post-anesthetic shivering in children. Pediatr Anesth 2007; 16:748-753.
- Koroglu A, Teksan H, Sagir O, Youcel A, Toprak HI, Ersoy OM. A comparison of the sedative, hemodynamic and respiratory effects of dexmedetomidine and propofol in children undergoing magnetic resonance imaging. Anesth Analg. 2006 Jul;103(1):63-67. [PubMed]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube