
Aamir Furqan1, Liaqat Ali2, Aatir Fayyaz3, Rana Altaf Ahmad4,5, Mirza Ahmad Raza Baig6, Syed Sohail Ahmad7
1Assistant Professor; 7Associate Professor; 4Professor & Head
Department of Cardiothoracic Anesthesia, Chaudhry Pervaiz Elahi Institute of Cardiology (CPEIC) Multan (Pakistan)
5Executive Director; 6Cardiac Perfusionist
Chaudhry Pervaiz Elahi Institute of Cardiology (CPEIC) Multan (Pakistan)
2Assistant Professor, Department of Anesthesiology, Multan Medical & Dental College, Multan (Pakistan).
3Assistant Professor, Children Hospital & Institute of Child Health, Multan (Pakistan)
Correspondence: Dr. Aamir Furqan, FCPS, Department of Cardiac Anesthesiology, Chaudhry Pervaiz Elahi Institute of Cardiology, Multan (Pakistan); Cell: +92-333-6203152; E-mail: draamir2009@hotmail.com
ABSTRACT
Objective: Pulmonary dysfunction is considered to be the most important complication after open heart surgery. Different maneuvers like intermittent or continuous positive pressure ventilation, low tidal volume ventilation and different vital capacity maneuvers have been used for reducing the incidence of pulmonary dysfunction after cardiac surgery. In this study we evaluated the effects of low tidal volume ventilation versus no-ventilation during cardiopulmonary bypass (CPB) in patients undergoing conventional CABG surgery.
Methodology: This randomized clinical trial was conducted in a tertiary care cardiac hospital. One hundred patients who were planned to undergo conventional CABG surgery were divided into two groups by using draw randomization procedure. In Group A patients (ventilation group) ventilation was continued at low tidal volume of 3 ml/kg, respiration rate of 12 breaths/min and PEEP of 5 cmH2O. In Group B patients (non-ventilation group) ventilation was arrested during CPB. For data analysis Statistical Package for Social Sciences (SPSS) V17 was used. Parametric variables were compared using unpaired t-test and non-parametric variables were compared using c2-test.
Results: The mean patient’s age in this study was 57.70 ± 8.57 years in ventilated group and 54.5 ± 8.33 years in non-ventilated group. PaO2/FiO2 ratio and alveolar-arterial oxygen tension gradient immediately after intubation was same in groups. But PaO2/FiO2 was significantly high in ventilated group after one hours of CPB and even after four hours of CPB (p < 0.001 and 0.002 respectively). Alveolar arterial oxygen tension (A-a O2) gradient after 1 hour and four hours of CPB was significantly low in Ventilated group (p < 0.001 and 0.001 respectively). Total Mechanical ventilation time was also significantly shorter in ventilated group 5.19 ± 1.96 hours versus 6.42 ± 2.60 hours in non-ventilated group (p 0.009). On 4th post-operative day, incidence of atelectasis was significantly low 20% in ventilated group versus 38% in non-ventilated group (p = 0.04).
Conclusion: Continuous low tidal volume ventilation is associated with better oxygenation after surgery and reduced risk of post-op pulmonary complications during cardiopulmonary bypass in patients undergoing conventional coronary artery bypass graft surgery.
Key words: Pulmonary dysfunction; Low tidal volume; Ventilation; Cardiopulmonary Bypass; Cardiopulmonary Arrest; Extracorporeal Circulation
Citation: Furqan A, Ali L, Fayyaz A, Ahmad RA, Baig MAR, Ahmad SS. Continuous low tidal volume ventilation during cardiopulmonary bypass reduces the risk of pulmonary dysfunction. Anaesth Pain & Intensive Care. 2016;20 Suppl 1:S37-S41
Received: 15 August 2016; Reviewed: September 2016; Accepted; 24 September 2016
INTRODUCTION
Cardiopulmonary bypass (CPB) is used by cardiac surgeons to work on non-beating heart. CPB is responsible for maintaining patient’s circulation, oxygenation, and temperature and provides a bloodless operative field to the surgeons by draining the blood from the right atrium and pumping it directly into the ascending aorta bypassing the lungs and the heart.1 This diversion from normal physiologic circulation may result in post-operative pulmonary dysfunction.2 Post-op pulmonary dysfunction is considered to be the most important complication after open heart surgery ranging from minor functional changes to the development of acute respiratory distress syndrome. The mortality rate is increased to 40-90% in patients who developed ARDS after the surgical procedure.3,4
Ventilation arrest after establishing CPB is practiced in many cardiac centers because lung oxygenation is no longer required after establishing CPB and lungs movements can interfere with surgical procedure. This ventilation arrest is associated with a high rate of retained bronchial sections, regional atelectasis, reduction in arterial O2 concentrations as a result of increase in arteriovenous shunt, decreased lung compliance, pulmonary edema and hence increased risk of nosocomial infections.5-7
Different maneuvers like intermittent or continuous positive pressure ventilation, low tidal volume ventilation and different vital capacity maneuvers have been shown to be beneficial in reducing the incidence of post-operative pulmonary dysfunction after cardiac surgery. 6,7,8-11 In this study we evaluated the effects of low tidal volume ventilation versus no-ventilation during CPB in patients undergoing conventional coronary artery bypass graft (CABG) surgery.
METHODOLOGY
This randomized clinical trial was conducted in a tertiary care cardiac hospital. The duration of this study was three months (01 March 2016 to 01 June 2016). One hundred patients who were planned to undergo conventional CABG surgery were divided into two groups by using draw randomization procedure. In Group A patients (ventilation group) ventilation was continued at low tidal volume of 3 ml/kg, respiration rate of 12 breaths/min and PEEP of 5 cmH2O. In Group B patients (non-ventilation group) ventilation was arrested during CPB. Patients who were planned to undergo off-pump surgery, and other valvular procedures, insulin dependent diabetes mellitus, reduced ejection fraction < 30%, obese patients and patients with pre-operative pulmonary dysfunction e.g. having forced vital capacity less than 40% of the predictive value were excluded from the study. Written informed consent was taken from every patient after briefing him/her about this research work. Ethical approval from department of academic affairs of the hospital was obtained.
Anesthesia was induced using standard hospital protocols. Fentanyl, midazolam and atracurium were used for anesthesia induction. Anesthesia was maintained using propofol, fentanyl and atracurium and isoflurane in all patients. Arterial and venous line cannulation was achieved in all patients before anesthesia induction. Invasive blood pressure and pulse oximetry was done in every patient. In all patients standard CPB was established using membrane oxygenator and roller pumps. Activated clotting time (ACT) was maintained above 480 sec during the CPB. Cardiac arrest was achieved using potassium enriched blood cardioplegic solution. After application of aortic cross-clamp, continuous ventilation with low tidal volume was started in Group A patients. While ventilation arrest was continued in Group B patients till the removal of cross-clamp. Moderate systemic cooling (temp =30-32 ºC) was achieved during surgery and patients were rewarmed to 37 ºC before weaning from CPB. Bypass time and cross-clamp time were noted. Sample for arterial blood gases were collected immediately after intubation, after one and four hours of CPB. Chest radiograph to rule out pulmonary complications e.g. pulmonary edema, atelectasis and pleural effusion was taken on 4th post-operative day. Extubation time, ICU stay and hospital stay time were also noted.
For data analysis Statistical Package for Social Sciences (SPSS) V17 was used. Parametric variables were compared using unpaired t-test and non-parametric variables were compared using c2-test.
RESULTS
The mean patient’s age in this study was 57.70 ± 8.57 years in ventilated group and 54.5 ± 8.33 years in non-ventilated group. There was no significant difference regarding smoking history and pre-operative ejection fraction between the groups. Bypass time and cross-clamp time were same between the groups (Table 1). PaO2/FiO2 ratio and alveolar-arterial oxygen tension gradient immediately after intubation was same in groups. But PaO2/FiO2 was significantly high in ventilated group after one hours of CPB and even after four hours of CPB (p < 0.001 and 0.002 respectively). Alveolar arterial oxygen tension (A-a O2) gradient after 1 hour of CPB was significantly low in ventilated group 21.45 ± 1.0 kPa versus 27.88 ± 1.98 kPa in non-ventilated group (p < 0.001). A-a O2 gradient after four hours of surgery was also higher in non-ventilated group 20.81 ± 1.94 kPa versus 19.37 ± 2.05 kPa (p = 0.001). Total mechanical ventilation time was significantly shorter in ventilated group 5.19 ± 1.96 hr versus 6.42 ± 2.60 hr in non-ventilated group (p = 0.009). There was no significant difference between the ICU stay and hospital stay period between the groups.
On 4th post-operative day, incidence of atelectasis was significantly low 20% in ventilated group versus 38% in non-ventilated group (p = 0.04). Although there was no significant difference regarding incidence of pleural effusion and pulmonary edema between groups (Figure 1).
Table 1: Comparison of demographic and operative variables
| Variables | Group A
(Ventilation Group) |
Group B
(Non-ventilation Group) |
P |
| Number of patients | 50 | 50 | |
| Age (Years) | 57.70 ± 8.57 | 54.5 ± 8.33 | 0.06 |
| Male Gender [n (%)] | 46 (92.0) | 45 (90.0) | 1.0 |
| Smoking History [n (%)] | 17 (34.0) | 20 (40.0) | 0.53 |
| Pre-op EF | 51.10 ± 9.38 | 50.30 ± 10.42 | 0.68 |
| Bypass Time (min) | 111.12 ± 25.99 | 110.98 ± 29.60 | 0.98 |
| X-clamp Time (min) | 64.52 ± 16.90 | 61.32 ± 17.10 | 0.34 |
EF= Ejection Fraction, X-clamp= cross clamp
Table 2: Comparison of clinical parameters
| Variables | Group A
(Ventilation Group) |
Group B
(Non-ventilation Group) |
P |
| PaO2/FiO2 Ratio after intubation | 335.90 ± 12.53 | 340.46 ± 19.95 | 0.17 |
| PaO2/FiO2 Ratio after 1 hour of CPB | 322.02 ± 12.27 | 294.36 ± 10.05 | < 0.001 |
| PaO2/FiO2 Ratio after hours of CPB | 298.38 ± 20.67 | 285.28 ± 21.48 | 0.002 |
| A-a O2 gradient after intubation (kPa) | 17.69 ± 0.92 | 17.58 ± 0.88 | 0.54 |
| A-a O2 gradient after 1 hour of CPB (kPa) | 21.45 ± 1.0 | 27.88 ± 1.98 | < 0.001 |
| A-a O2 gradient after 4 hour of CPB (kPa) | 19.37 ± 2.05 | 20.81 ± 1.94 | 0.001 |
| Ventilation time | 5.19 ± 1.96 | 6.42 ± 2.60 | 0.009 |
| ICU stay | 32.83 ± 10.90 | 35.04 ± 12.64 | 0.35 |
| Hospital stay | 7.28 ± 1.91 | 7.34 ± 3.32 | 0.91 |
CPB= CPB, ICU= Intensive care unit
| P-value 0.36 |
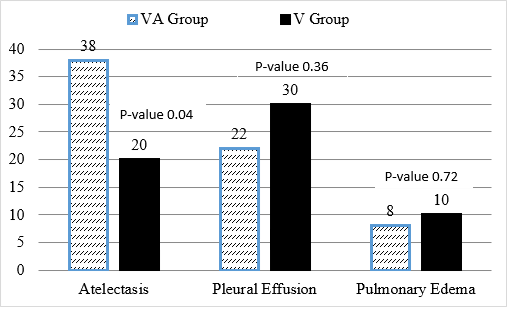
Figure 1: Comparison of postop chest complications seen on chest radiograph after 4 days of surgery
DISCUSSION
Despite many advancements in CPB techniques and improvements in post-op care in intensive care units, pulmonary dysfunction is still a well-known complication of CPB and is associated with increased risk of morbidity and mortality in this patient population.12 Systemic inflammatory response syndrome (SIRS) is considered to be the prime factor responsible for pulmonary dysfunction.4 SIRS is initiated immediately after establishing CPB resulting in leukocytes and complement system activation. Activated leukocytes are trapped in the interstitial lung tissue during their transit from pulmonary vasculature.13,14 Oxygen free radicals are also formed during CPB that also mediate pulmonary endothelial damage as well.15 Ischemia-reperfusion injury is also initiated after restoration of blood flow to the ischemic lungs after surgery. This ischemia-reperfusion injury along with systemic inflammatory response syndrome initiates a vicious cycle resulting in post CPB pulmonary dysfunction.11
Ventilation arrest during CPB has also been shown to be associated with the development of pulmonary atelectasis, increase in pulmonary arteriovenous shunts which results in reduced PaO2 and increased incidence of chest infections resulting in pulmonary dysfunction.6,7
To reduce the incidence of post-operative pulmonary dysfunction many modifications have been made in ventilation protocols during CPB, these include modifications in vital capacity maneuvers, continuous ventilation with low tidal volume and continuous positive airway pressure. 6,7,8-11,16
In this study, we used low tidal volume continuous ventilation in one group and in other group conventional ventilation method e.g. ventilator arrest was maintained during CPB. We found significantly better results in ventilation group. Post-op PaO2/FiO2 ratio was significantly high in ventilation group as compared to non-ventilation group. A-a O2 gradient after one and four hours of surgery was also significantly low in ventilation group as compared to non-ventilation group. We also found a reduced incidence of pulmonary atelectasis in ventilation group as compared to non-ventilation group.
Ahmed M et al. concluded that low tidal volume ventilation is associated with better PaO2/FiO2 ratio and A-a O2 gradient in the immediate post-op period i.e. after one hour of surgery. But in their study there was no significant difference in PaO2/FiO2 ratio and A-a O2 gradient after four hours of surgery.11 In our study, PaO2/FiO2 ratio was significantly high even after four hours of surgery in ventilation group. Similarly A-a O2 gradient after four hours was low in ventilation group as compared to the non-ventilation group. Ahmed M et al. did not found any significant difference regarding the incidence of pulmonary atelectasis, edema and pleural effusion between the groups. But in our study, the incidence of pulmonary atelectasis was significantly high in non-ventilated group as compared to the ventilated group. Our study partially supported the results of this study.
Dasgupta et al concluded that low tidal volume ventilation during CPB is associated with better post-op oxygenation and pulmonary functions as compared to no-ventilation or continuous positive pressure ventilation. They found shorter extubation time and ICU stay time in low tidal volume group.17 In our study, we also found shorter extubation time in ventilation group. In our study, ICU stay time was no significantly different between the groups. Our study supported the results of this study. Alavi et al. also found better oxygen saturation and decreased alveolar arterial oxygen gradient in low tidal volume group.10 Many other studies found significant results by using continuous low tidal volume ventilation during CPB.18-20
Continuous low tidal volume ventilation during CPB has shown to be associated with reduced serum chemokine concentrations and less release of metalloproteinases during surgery.21,22 Fernando et al. found that continuous low tidal volume ventilation is associated with reduced inflammatory response thereby reducing post-op pulmonary complications.23
CONCLUSION
Continuous low tidal volume ventilation is associated with better oxygenation after surgery and reduced risk of post-op pulmonary complications during cardiopulmonary bypass in patients undergoing conventional coronary artery bypass graft surgery.
Conflict of interest: None declared by the authors
Author contribution: AF: Concept; Manuscript writing. LA: Study design; Manuscript writing. AF: Statistical analysis. RAA: Proof reading; Final approval. MARB: Data collection. SSA: Data collection; Data analysis
REFERENCES
- Durukan AB, Gurbuz HA, Ucar HI, Yorgancioglu C, Salman N, Unal EU. Ventilation during cardiopulmonary bypass did not attenuate inflammatory response or affect postoperative outcomes. Cardiovasc J Afr. 2013;24(6):224. [PubMed] [Free Full Text] doi: 10.5830/CVJA-2013-041
- Rea H, Harris E, Seelye E, Whitlock R, Withy S. The effects of cardiopulmonary bypass upon pulmonary gas exchange. J Thorac Cardiovasc Surg. 1978;75(1):104-20. [PubMed] [Free Full Text] DOI: http://dx.doi.org/10.1016/S0003-4975(99)01196-0
- Messent M, Sullivan K, Keogh B, Morgan C, Evans T. Adult respiratory distress syndrome following cardiopulmonary bypass: incidence and prediction. Anaesthesia. 1992;47(3):267-8. [PubMed] [Free Full Text] DOI: 10.1111/j.1365-2044.1992.tb02134.x
- Asimakopoulos G, Smith PL, Ratnatunga CP, Taylor KM. Lung injury and acute respiratory distress syndrome after cardiopulmonary bypass. The Ann Thorac Surg. 1999;68(3):1107-15. [PubMed] [Free Full Text] DOI: http://dx.doi.org/10.1016/S0003-4975(99)00781-X
- Friedman M, Sellke FW, Wang SY, Weintraub RM, Johnson RG. Parameters of pulmonary injury after total or partial cardiopulmonary bypass. Circulation. 1994;90(5 Pt 2):II262-8. [PubMed]
- Magnusson L, Zemgulis V, Tenling A, Wernlund J, Tyden H, Thelin S, et al. Use of a Vital Capacity Maneuver to Prevent Atelectasis after Cardiopulmonary Bypass An Experimental Study. J Am Soc Anesthesiol. 1998;88(1):134-42. [PubMed]
- Loeckinger A, Kleinsasser A, Lindner KH, Margreiter J, Keller C, Hoermann C. Continuous positive airway pressure at 10 cm H2O during cardiopulmonary bypass improves postoperative gas exchange. Anesth Analg. 2000;91(3):522-7. [PubMed] doi: 10.1213/00000539-200009000-00004
- Ng CS, Wan S, Yim AP, Arifi AA. Pulmonary dysfunction after cardiac surgery. CHEST J. 2002;121(4):1269-77. [PubMed] [Free Full Text]
- Badenes R, Lozano A, Belda FJ. Postoperative pulmonary dysfunction and mechanical ventilation in cardiac surgery. Crit care res pract. 2015;1-8. [PubMed]doi.10.1155/2015/420513
- Alavi M, Pakrooh B, Mirmesdagh Y, Bakhshandeh H, Babaee T, Hosseini S, et al. The effects of positive airway pressure ventilation during cardiopulmonary bypass on pulmonary function following open heart surgery. Res Cardiovasc Med. 2013;2(2):79. [PubMed] doi: 10.5812/cardiovascmed.8129
- Salama AM, Eldegwy MH, Othman H, Abdelaziz AS. Low tidal volume lung ventilation during cardiopulmonary bypass decreases the potential of postoperative lung injury. Ain-Shams J Anaesthesiol. 2014;7(2):232. [free full text]
- Apostolakis E, Filos KS, Koletsis E, Dougenis D. Lung dysfunction following cardiopulmonary bypass. J Card Surg. 2010;25(1):47-55. [PubMed] [Free Full Text] DOI: 10.1111/j.1540-8191.2009.00823.x
- Gu Y, Boonstra P, Graaff R, Rijnsburger A, Mungroop H, Van Oeveren W. Pressure drop, shear stress, and activation of leukocytes during cardiopulmonary bypass: a comparison between hollow fiber and flat sheet membrane oxygenators. Artif Organs. 2000;24(1):43-8. [PubMed][Free full text] DOI: 10.1046/j.1525-1594.2000.06351.x
- Tennenberg SD, Clardy CW, Bailey WW, Solomkin JS. Complement activation and lung permeability during cardiopulmonary bypass. Ann Thorac Surg. 1990;50(4):597-601. [PubMed] [Free Full Text]
- Ascione R, Lloyd CT, Underwood MJ, Lotto AA, Pitsis AA, Angelini GD. Inflammatory response after coronary revascularization with or without cardiopulmonary bypass. Ann Thorac Surg. 2000;69(4):1198-204. [PubMed] [Free Full Text]
- Meade MO, Cook DJ, Guyatt GH, Slutsky AS, Arabi YM, Cooper DJ, et al. Ventilation strategy using low tidal volumes, recruitment maneuvers, and high positive end-expiratory pressure for acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. Jama. 2008;299(6):637-45. [PubMed][free full text ] doi: 10.1001/jama.299.6.637.
- Dasgupta CS, Kar SK, Ganguly T, Goswami A. Comparison of low ventilation, no ventilation and continuous positive pressure Ventilation as pulmonary protection strategy during cardiopulmonary bypass. 2015;3(1):1-5. [PubMed] [Free Full Text]
- Davoudi M, Farhanchi A, Moradi A, Bakhshaei MH, Safarpour G. The Effect of Low Tidal Volume Ventilation during Cardiopulmonary Bypass on Postoperative Pulmonary Function. J Tehran Uni Heart Center. 2010;5(3):128-31. [PubMed] [Free Full Text]
- Gür AK, Özcan S, Kurt T, Eker E, Odabasi D, Destan B, et al. The Effects of Low Tidal Volume and Ventilation on the Lungs in the Postoperative Period during Cardio Pulmonary Bypass in the Heart Surgery. IJCR. 2014;2(2):56-60. [PubMed]
- Gu W-J, Wang F, Liu J-C. Effect of lung-protective ventilation with lower tidal volumes on clinical outcomes among patients undergoing surgery: a meta-analysis of randomized controlled trials. Canadian Med Assoc J. 2015;187(3):E101-E9. [PubMed] [Free Full Text] doi: 10.1503/cmaj.141005
- Beer L, Szerafin T, Mitterbauer A, Debreceni T, Maros T, Dworschak M, et al. Low tidal volume ventilation during cardiopulmonary bypass reduces postoperative chemokine serum concentrations. Thorac and Cardiovasc Surg. 2014;62(08):677-82. [PubMed][Free Full Text] doi: 10.1055/s-0034-1387824.
- Beer L, Warszawska JM, Schenk P, Debreceni T, Dworschak M, Roth GA, et al. Intraoperative ventilation strategy during cardiopulmonary bypass attenuates the release of matrix metalloproteinases and improves oxygenation. J Surg Res. 2015;195(1):294-302. [PubMed][Free Full Text] doi: 10.1016/j.jss.2014.12.022.
- Ferrando C, Soro M, Belda FJ. Protection strategies during cardiopulmonary bypass: ventilation, anesthetics and oxygen. Curr Opin Anesthesiol. 2015;28(1):73-80. [PubMed]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube