
Indira Kumari1, Ravindra Kumar Gehlot2, Rajendra Verma3,
Aditi Narang4, Virendra Verma5, Pooja Suwalka6
1Professor; 2Assistant Professor; 4Resident
R.N.T. Medical College, Udaipur, Rajasthan, (India)
3Senior Resident, Pacific Institute of Medical Sciences, Udaipur, Rajasthan, (India)
Correspondence: Dr. Ravindra Kumar Gehlot, Quarter No. 3, Dilshad Bhawan, 69, Chetak Circle, Udaipur (Rajasthan)- 313001(India); Mobile: +91 9468694902; E-mail: dr.rgehlot.2010@gmail.com
ABSTRACT
Objective: To compare the effect of adding two different doses of dexmedetomidine to ropivacaine, on onset and duration of analgesia for supraclavicular brachial plexus block in patients scheduled for upper limb orthopedic surgery.
Methodology: This prospective randomized double blind comparative study was conducted at our institution. After ethical committee approval and informed patient consents, 50 patients of ASA I, II and aged 21-60 years, who were scheduled for elective upper limb surgery and were enrolled in the study and randomly divided into two equal groups. They received either 30 ml of 0.75% ropivacaine plus dexmedetomidine (1 µg/kg) diluted with normal saline up to 5 ml (total volume = 35 ml) in Group 1 or 30 ml of 0.75% ropivacaine plus dexmedetomidine (2 µg/kg) diluted with normal saline up to 5 ml (total volume = 35 ml) in Group 2. The onset and duration of sensory and motor block, duration of analgesia, hemodynamic parameters, sedation score, VAS and side effects were recorded.
Results: Onset time of sensory and motor block were earlier in Group 2 than in Group 1 (p < 0.001). Duration of sensory and motor block and duration of analgesia were longer in Group 2 than in Group 1 (p < 0.001). There was no significant difference in the incidence of hypotension and bradycardia between both the groups (p > 0.05). There was a statistically significant reduction in number of rescue analgesic doses and total dose consumption in 24 hours in Group 2 than in Group 1.
Quantitative data are represented as arithmetic mean and standard deviation and analyzed using Student’s t test or ANOVA as per need. Qualitative data are represented as number (proportion or percentage) and analyzed using Chi square test. The levels of significance and α-error were kept 95% and 5% respectively for all statistical analyses. P values < 0.05 were considered significant.
Conclusion: Dexmedetomidine 2 µg/kg provided longer duration of intraoperative sensory and motor analgesia and prolonged postoperative analgesia in comparison to dexmedetomidine 1 µg/kg when added to inj ropivacaine 0.75%, for supraclavicular brachial plexus block without any appreciable side effects.
Key words: Ropivacaine; Dexmedetomidine; Supraclavicular brachial plexus block; Analgesia, Postoperative
Citation: Kumari I, Gehlot RK, Verma R, Narang A, Verma V, Suwalka P. Comparison of two different doses of dexmedetomidine added to ropivacaine in patients posted for upper limb surgery under supraclavicular brachial plexus block. Anaesth Pain & Intensive Care 2017;21(2):__
Received: 21 October 2016, Reviewed: 6 Dec 2016, Corrected: 12 Dec 2016, Accepted: 12 Jan 2017
INTRODUCTION
Brachial plexus block is a widely employed regional nerve block technique for upper limb surgeries as an alternative to general anesthesia. Supraclavicular brachial plexus block is ideal for operations involving the arm and the forearm, from the lower humerus down to the hand.1 Main advantages are no need of controlled ventilation and less cardiovascular disturbance, but with superior intraoperative pain control, attenuation of the surgical stress response, minimal systemic impairment, lower incidence of postoperative nausea and vomiting, excellent localized postoperative analgesia, a decreased hospital discharge time and cost.2,3 Ropivacaine, a relatively new long acting local anesthetic with fast onset, long duration and minimal toxic profile. Bupivacaine, with its wide and unpredictable latency of nerve block and enhanced neuro and cardiovascular toxicity4,5 needed replacement with a drug of better anesthetic and safety profile. Various adjuvants have been used along with local anesthetic agents to improve the characteristics and surgical duration of supraclavicular block. Some α-2 adrenoceptor agonists (clonidine and dexmedetomidine) have been previously used efficaciously and safely as an adjuvant to local anesthetic agents in regional nerve blocks.6,7
Dexmedetomidine has more sedative potential and provides optimal intraoperative and postoperative patient comfort. In our search we were unable to locate any study with dexmedetomidine in two different doses added to ropivacaine in supraclavicular block. Our objective was to compare the clinical effect of two different doses of dexmedetomidine (1 µg/kg and 2 µg/kg) as an adjuvant to ropivacaine 0.75% in supraclavicular brachial plexus block in upper extremity surgery and see its effect on block characteristics and the duration of postoperative analgesia.
METHODOLOGY
After Institutional Ethical Committee (IEC) approval, this prospective, comparative study was conducted at the department of anesthesiology and department of orthopedic surgery from July 2014 to December 2015 at M.B. Hospital attached to RNT Medical College, Udaipur (Rajasthan). After informed written consent from patients, the study was conducted on 50 patients of ASA Grade I and II of either gender, aged 21 to 60 years, who underwent various elective orthopedic surgeries on the upper limb e.g., open reduction of fracture humerus with K wire fixation, plating or screw, fracture of radius/ulna and fracture of olecranon etc. under supraclavicular brachial plexus block.
Following were excluded: patients on adrenoceptor agonist or antagonist therapy, patients with coagulopathy, those with known hypersensitivity to ropivacaine / dexmedetomidine, history of significant systemic disease, history of alcohol or drug abuse, patchy or inadequate anesthesia requiring conversion to general anesthesia or when additional opioid or sedation was administered, pregnant or lactating women, patient refusal and subsequent pneumothorax.
Fifty patients were randomly divided using sealed envelope techniques into two groups of 25 each. Group 1 (n=25) received 0.75% ropivacaine 30 ml plus dexmedetomidine 1 µg/kg diluted with normal saline up to 5 ml (total volume = 35 ml)
Group 2 (n=25) received 0.75% ropivacaine 30 ml plus dexmedetomidine 2 µg/kg body weight diluted with normal saline up to 5 ml (total volume = 35 ml)
The anesthetic solution was prepared by an anesthesiologist who was not involved in the study and the anesthesiologist who performed the block was blinded to the treatment group.
On arrival to the operating room, the patients were examined to confirm the findings of pre-anesthetic checkup. An IV line was secured using a 20 G cannula in the unaffected limb and intravenous fluid was started at the rate of 10 ml/kg. Standard monitoring was applied using multipara monitors for heart rate, non-invasive blood pressure (NIBP), pulse oximetry for peripheral oxygen saturation (SpO2)and continuous ECG monitoring for recording arrhythmias and ST segment. Baseline vitals were recorded. Inj. midazolam 0.02 mg/kg was given five minutes before supraclavicular block.
The patients were administered brachial plexus block via supraclavicular route using the subclavian perivascular approach in supine position with arm adducted. Under aseptic precautions, the injection site was identified to be 1 cm behind the midpoint of clavicle (where the pulsation of the subclavian artery was felt) and infiltrated with 1 ml of 2% lignocaine subcutaneously. A nerve stimulator, INMED. Model NSML-100® and 5 cm needle, were used to locate the brachial plexus. The intensity of the stimulating current, was initially set to deliver 1 mA, and was gradually decreased to 0.5 mA after the appropriate distal motor response (thumb abduction for radial nerve, thumb adduction for ulnar nerve, thumb opposition for median nerve and flexion of the elbow for musculocutaneous nerve) was observed. The drug was injected via a connecting line of 30 cm attached to locator needle by another anesthesiologist assistant to prevent needle movement. During injection of the drug solution, negative aspiration was done after every 5 ml to avoid intravascular injection. Plexus block was considered successful when all four nerve territories (ulnar, radial, median and musculocutaneous) were effectively blocked for both sensory and motor components.
Sensory block was assessed using a 3-point scale8, [0= normal sensation, 1= loss of sensation to pin prick (analgesia), 2= loss of sensation of touch (anesthesia)] for a pin prick with 24 G hypodermic needle.
Motor block was assessed using Modified Bromage Scale (Grade 0= Normal motor function with full extension and flexion of the elbow, wrist and fingers, Grade 1= Decreased motor strength with ability to move fingers only and Grade 2= Complete motor block with inability to move the fingers.
The following were also defined
| Onset time for sensory block- | time interval between the end of local anesthetic administration and complete sensory block (score 2 for all nerves) |
| Duration of sensory block- | time interval between the complete sensory block and complete resolution of anesthesia on all the nerves (Grade 0) |
| Onset time for motor block- | time interval between total local anesthetic administration and complete motor block (grade 2) |
| Duration of motor block- | time interval from complete motor block to complete recovery of motor function of hand and forearm (grade 0) |
| Duration of analgesia- | The time between end of drug administration in the brachial block and first rescue analgesic dose administered. |
Perioperative sedation was rated by using the 4 point sedation score7 (0=awake, 1= drowsy, 2= sleeping but arousable on verbal command, 3= sleeping and arousable only on tactile stimulation).
Heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), oxygen saturation (SpO2) and sedation were recorded at 0, 5, 10, 15, 30, 45, 60, 90 and 120 min intraoperatively. Postoperative vital signs, e.g. SpO2, VAS score, sedation score, were monitored 2 hourly for the first 8 hours, then 4 hourly till 24 hours. Postoperative intensity of pain was measured using a 10 point Visual Analogue Scale (VAS). If VAS was more than 3, inj tramadol 2 mg/kg was administered as infusion as per routine protocol of our institute. All patients were observed for any discomfort, nausea, vomiting, dryness of mouth, pain, bradycardia/tachycardia, hypotension and complications like pneumothorax, hematoma, local anesthesia toxicity, post block neuropathy and complications of block using nerve stimulator like arterial puncture, intraneural injection and nerve injury in the intra- and postoperative periods.
Statistical Analysis: Sample size was calculated on the basis of the study done by Kohli S et al.6 The data were entered and statistically analyzed using MS Excel, Epi Info 6 and SPSS. Quantitative data are represented as arithmetic mean and standard deviation and analyzed using Student t test or ANOVA as per need. Qualitative data are represented as numbers (proportion or percentage) and analyzed using Chi square test. The levels of significance and α-error were kept 95% and 5% respectively, for all statistical analyses. P values < 0.05 were considered significant.
RESULTS
Brachial plexus block was performed in 50 patients; out of these two were excluded (one in Group 1 and one in Group 2) due to incomplete block effect. A total of 48 patients were included in the study. There was no statistically significant difference between the demographic data (age, sex, weight, duration of surgery) and baseline vital signs (HR, SBP, DBP, SpO2) in both the groups .
Table 1: Demographic data and baseline vitals of patients in two groups
| Group 1 | Group 2 | P value | |
| Age (years) | 39.42 ± 14.67 | 38.83 ± 14.01 | 0.89 |
| Sex | 14/10 | 17/7 | 0.365 |
| Weight (kg) | 59.75 ± 8.02 | 59.92 ± 7.51 | 0.941 |
| Duration of surgery (min) | 74.00 ± 5.60 | 73.29 ± 5.53 | 0.661 |
| aseline PR (per min) | 75.08 ± 6.75 | 79.00 ± 6.54 | 0.051 |
| Baseline SBP (mm Hg) | 121.50 ± 5.25 | 122.83 ± 6.98 | 0.458 |
| Baseline DBP (mm Hg) | 70.00 ± 5.69 | 69.25 ± 6.51 | 0.673 |
| Baseline SpO2 (%) | 98.91 ± 0.71 | 98.62 ± 0.82 | 0.198 |
The onset of sensory and motor block was earlier and duration of analgesia and sensory motor block was longer in Group 2 as compared to Group 1 (statistically highly significant, p < 0.001)
Table 2: Comparison of onset and duration of sensory-motor block in two groups.
| Group 1 | Group 2 | P value | |
| Onset of sensory block (min) | 3.88 ± 0.68 | 2.29 ± 0.75 | < 0.001 |
| Onset of motor block (min) | 7.38 ± 0.97 | 5.42 ± 1.21 | < 0.001 |
| Duration of sensory block (min) | 733.96 ± 29.00 | 952.50 ± 29.15 | < 0.001 |
| Duration of motor block (min) | 797.29 ± 28.63 | 1004.17 ± 37.41 | < 0.001 |
| Duration of analgesia (min) | 870.83 ± 32.22 | 1070.62 ± 43.84 | < 0.001 |
Postoperative distribution of patients according to VAS > 3 shows that in Group 1 out of 24 patients, 14 (58.33%) patients required two doses, nine patients (37.5%) required single dose and one patient (4.17%) did not require any rescue analgesic. In Group 2, only one (4.17%) patient required two doses, 18 (75%) patients required single dose and five (20.83%) patients did not require any rescue analgesic in 24 hour period. Total rescue analgesic consumption was significantly less in Group 2 (20 doses) as compared to Group 1 (37 doses) (p=0.024).
Table 3: No. of patients requiring rescue analgesia within 24 hrs
| Group 1 | Group 2 | P value | |
| No. of patients | 23 (95.83%) | 19 (79.17%) | 0.537 |
| 0 dose | 1 (4.17%) | 5 (20.83%) | 0.102 |
| 1 dose | 9 (37.5%) | 18 (75%) | 0.080 |
| 2 dose | 14 (58.33%) | 1 (4.17%) | 0.000 |
| Total no. of dose | 37 | 20 | 0.024 |
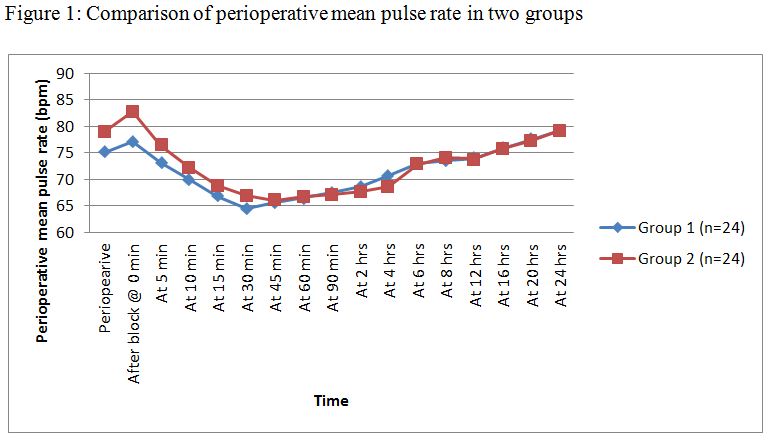
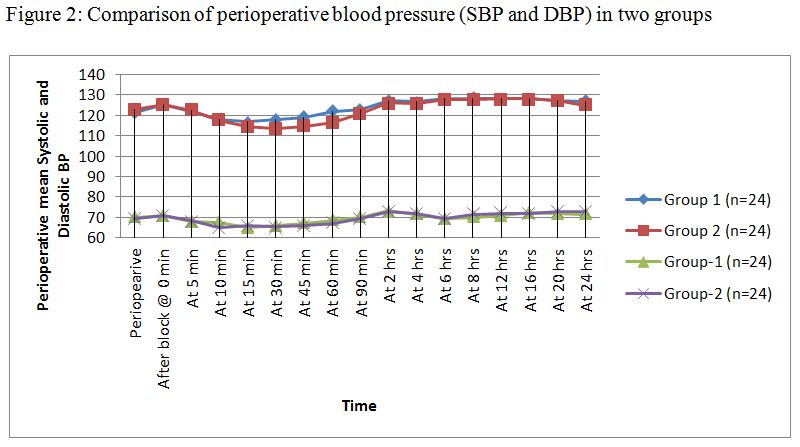
Incidence of side effects were comparable (p > 0.05) in both the groups. Three patients (12.50%) had bradycardia in Group 1 and 5 patients (20.83%) in Group 2. They were treated with inj. atropine 0.6 mg. One patient (4.17%) had hypotension in Group 1 and 2 patients (8.33%) in Group 2. They were treated with incremental doses of inj. mephentermine 6 mg bolus and crystalloid infusion. No other adverse effect was observed in the study. There was no significant fall in mean pulse rate and blood pressure in both groups perioperatively and hemodynamic parameters were comparable perioperatively
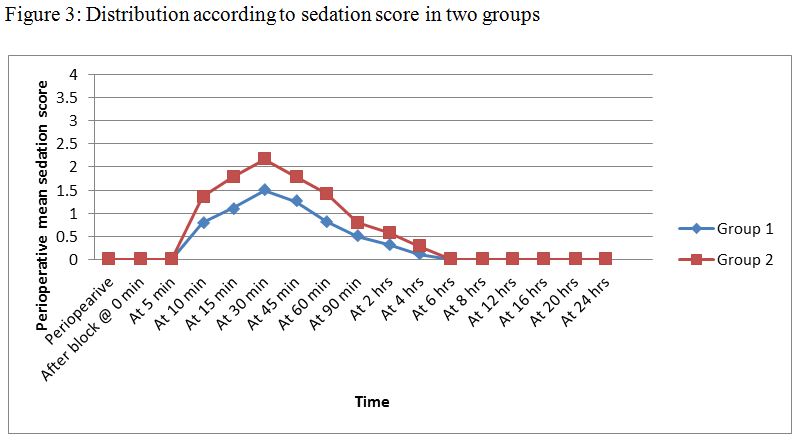
Sedation scores were higher and quality of operative conditions was better in Group 2 than in Group 1 and found statistically non-significant.
DISCUSSION
Results of this prospective randomized, double blinded comparative study demonstrate that adding 2 µg/kg dexmedetomidine to 0.75% ropivacaine hastened the onset of sensory and motor block and prolonged the duration of postoperative analgesia in supraclavicular brachial plexus block. Hemodynamic parameters remained stable throughout the study period with both the doses but higher dose caused more sedation.With the use of dexmedetomidine as adjuvant to ropivacaine causes faster onset of action of local anesthetics, rapid establishment of both sensory and motor blockade, prolonged duration of analgesia into the postoperative period and stable cardiovascular parameters makes these agents very effective adjuvants in regional anesthesia. Both of these drugs have been widely used by several researchers for brachial plexus block in various doses with various local anesthetic agents.7,9 Both drugs were found effective for this purpose.Our study showed that onset of sensory and motor block was earlier in Group 2 than in Group 1. This difference was statistically significant (p < 0.001). We were unable to locate any previous studies comparing two different doses of dexmedetomidine with 30 ml of 0.75% ropivacaine. In our study higher dose of dexmedetomidine resulted in earlier onset of sensory block, but the results of motor block were comparable to other studies.10,11Duration of sensory and motor block were statistically different between the two groups and duration was more prolonged in Group 2 as compared to Group 1 (p < 0.001). These results were comparable with other studies.12-15Duration of analgesia was prolonged in Group 2 as compared to Group 1. The difference was statistically significant (p < 0.001). There was decrease in mean VAS scores in Group 2 till 8 hours without statistically significant difference but at 12 to 20 hours there was significant difference in VAS scores, where Group 2 had lower scores as compared to Group 1.There was significant difference in number of patients requiring two doses of rescue analgesic (p = 0.000). Results show that higher dose of dexmedetomidine prolongs the duration of analgesia significantly and also consumption of rescue analgesic is reduced. These results were comparable with other studies.13-15In our study higher dose of dexmedetomidine produced higher sedation scores but patients were arousable by gentle tactile stimulation. Completely successful block was achieved in 88% of patients in both the groups. These results were comparable with other studies.16,17Results suggested that only slight decrease in heart rate was observed which reaffirms the established effects of α-2 adrenoceptor in central nervous system. They inhibit the release of norepinephrine, terminating the propagation of pain signals and their post synaptic activation, inhibition of sympathetic activity, thereby decreasing HR and BP.18Changes in mean PR and blood pressure (SBP & DBP) were within 20% from baseline during first 24 hr after block in both groups this shows hemodynamic stability, with maximum fall of mean PR 14% at 30 min in Group 1 and 16.45% at 45 min in Group 2. There was no significant difference in incidence of bradycardia and hypotension in both groups (p > 0.05). These results were consistent with various other studies.15,19In our study we observed fall in saturation in both groups but this was easily managed by administering oxygen via ventimask at 4-5 L/min and there was no significant episodes of hypoxemia like some earlier studies.19No complications related to brachial plexus block using nerve stimulator was observed in our study. Even though we used higher dose of ropivacaine, we did not find any local anesthetic toxicity in any of the patients. In several studies, maximum dose of ropivacaine up to 5 mg/kg was reported to be safe without any toxic effect. Also Geiger and colleagues reported safe use of 225 mg (0.75%) of ropivacaine to produce satisfactory sensory and motor blockade with stable hemodynamic profile and no sign of cardiovascular or neural toxicity.Keeping the results of our study in view, we recommend that dexmedetomidine in a dose of 2 µg/kg can safely and effectively be used as an adjuvant to brachial plexus block for upper limb surgeries.
CONCLUSION
Higher dose of dexmedetomidine (2 µg/kg) with 30 ml of 0.75% ropivacaine in brachial plexus block resulted in earlier onset, prolonged duration of sensorimotor blockade and provided a longer pain free postoperative period without significant hemodynamic alterations, when compared to lower dose of dexmedetomidine (1 µg/kg) with 30 ml of 0.75% ropivacaine.
Conflict of interest: Nil declared by the authors
Authors’ Contribution:IK: ConceptRKG: Conduction of study and manuscript editingRV: Data collection and analysesAN, VV: Conduction of the studyPS: Manuscript editing
REFERENCES
- Moore DC, Bridenbaugh LD. Eather KF. Block of the upper extremity. Arch Surg. 1965 Jan;90:68-72. [PubMed]
- Liu SS, Strodtbeck WM, Richman JM. Wu CL. A comparison of regional versus general anesthesia for ambulatory anesthesia: a meta-analysis of randomized controlled trials. Anesth Analg. 2005 Dec;101(6):1634-42. [PubMed]
- Borgeat A, Ekatodramis G, Schenker CA. Postoperative nausea and vomiting in regional anesthesia: a review. Anesthesiology. 2003 Feb;98(2):530-47. [PubMed] [Free full text]
- Bertini L, Tagariello V, Mancini S, Ciaschi A, Posteraro CM, Benedetto P, et al.. 0.75% and 0.5% ropivacaine for axillary brachial plexus block: a clinical comparison with 0.5% bupivacaine, Reg Anaesth Pain Med. 1999 Nov-Dec;24(6):514-518. [PubMed]
- Capogna G, Celleno D, Laudano D, Giunta F. Alkalinization of local anaesthetic.Which block, which local anesthetic? Reg Anaesth. 1995 Sep-Oct; 20(5):369-77. [PubMed]
- Kohli S, Kaur M, Sahoo S, Vajifdar H, Kohli P. Brachial plexus block: Comparison of two different doses of clonidine added to bupivacaine. J Anaesthesiol Clin Pharmacol. 2013 Oct;29(4):491-5. doi: 10.4103/0970-9185.119147. [PubMed] [Free full text]
- Hutschala D, Mascher H, Schemetter L, Kimscha W, Eichler HG. Clonidine added to bupivacaine enhances and prolongs analgesia after brachial plexus block via a local mechanism in healthy volunteers. European J Anaesth 2004;21(3):198-204.
- Agarwal S, Aggarwal R, Gupta P. Dexmedetomidine prolongs the effect of bupivacaine in supraclavicular brachial plexus block. J Anaesthesiol Clin Pharmacol. 2014 Jan;30(1):36-40. doi: 10.4103/0970-9185.125701 [PubMed] [Free full text]
- Esmaoglu A, Yegenoglu F, Akin A, Turk CY. Dexmedetomidine added to levobupivaciane prolongs axillary brachial plexus block. Anaesth Analg. 2010 Dec; 111(6):1548-51. doi: 10.1213/ANE.0b013e3181fa3095 [PubMed]
- Swami SS, Keniya VM, Ladi SD, Rao R. Comparision of dexmedetomidine and clonidine (α2 agonist drugs) as an adjuvant to local anaesthesia in supraclavicular brachial plexus block: A randomised double-blind prospective study. Indian J Anaesth. 2012 May;56(3):243-9. doi: 10.4103/0019-5049.98767. [PubMed] [Free full text]
- Tripathi D, Shah K, Shah C, Shah S, Das E. Supraclavicular Brachail Plexus Block for Upper Limb Orthopaedic Surgery: A Randomized Double Blinded Comparison Between Ropivacaine and Bupivacaine. The Internet Journal of Anesthesiology 2012; 30. [PubMed] [Free full text]
- Das A, Majumdar S, Halder S, Chattopadhyay S, Pal S, Kundu R et al. Efficacy of dexmedetomidine as adjuvant in ropivacaine-induced
supraclavicular brachial plexus block: A prospective, double-blinded and randomized
controlled study. Saudi J Anaesth. 2014 Nov;8(Suppl 1):S72-77. [Free full text] - Ammar AS, Mahmoud KM, Ultrasound-guided single injection infraclavicular brachial plexus block using bupivacaine alone or combined with dexmedetomidine for pain control in upper limb surgery:a prospective randomized controlled trial. Saudi J Anaesth. 2012 Apr;6(2):109-14. [PubMed] [Free full text]
- Dar FA, Najar MR, Jan N. Dexmedetomidine added to ropivacaine prolongs axillary brachial plexus block. Int J Biomed Adv Res. 2013;4:719-22. [Free full text]
- Zhang Y, Wang CS, Shi JH, Sun B, Liu SJ, Li P et al. Perineural administration of dexmedetomidine in combination with ropivacaine prolongs axillary brachial plexus block. Int J Clin Exp Med. 2014 Mar 15;7(3):680-685. [PubMed] [Free full text]
- Memmis D, Turan A, Karamanlioglu B, Pamucku Z, Kurt I. Adding dexmedetomidie to lidocaine for intravenous regional anesthesia. Anesth Analg. 2004 Mar;98(3):835-40. [PubMed]
- Abosedira MA. Adding Clonidine or Dexmedetomidine to Lidocaine During Bier’s Block: A Comparative Study. J Med Sci. 2008 Nov 1;8(7):660-4. [Free full text]
- Kuthiala G, Chaudhary G. Ropivacaine: A review of its pharmacology & clinical use. Ind J Anaesth. 2011 Mar;55(2):104-10. doi: 10.4103/0019-5049.79875. [PubMed] [Free full text]
- Kwon Y, Huwang SM, Lee JJ, Kim JH. The effect of dexmedetomidine as an adjuvant to ropivacaine on the bispectral index for supraclavicular brachial plexus block. Korean J Anaesthesiol. 2015 Feb;68(1):32-36. doi: 10.4097/kjae.2015.68.1.32 [PubMed] [Free full text]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube