
MedhatHannallah, MD, FFARCS1, Yonette Exeter, CRNP2, Lauren Scher, MS3,
Ghofran Habib, MD4, George Hwang,MD5, Ling Cai, PhD, MA6
1Professor, 5Instructor, 4Research Intern
Department of Anesthesia, Georgetown University Hospital, Washington, DC, USA.
2Nurse Practitioner, Department of Medicine, Division of Gastroenterology, Georgetown University Hospital, Washington, DC, (USA)
6Biostatistician, 3Medical Student
Georgetown University School of Medicine, Washington, DC, USA.
Correspondence: MedhatHannallah, MD, FFARCS, Department of Anesthesia, Georgetown University Hospital, 3800 Reservoir Road, SW, Washington DC, 20007 (USA); Phone: 202-444-6680; E-mail: hannallm@gunet.georgetown.edu
ABSTRACT
Background:This study was designed to determine the degree of correlation between two obstructive sleep apnea (OSA) questionnaires, the validated ‘STOP-Bang’ questionnaire and‘Flemons’ Modified Neck Circumference (MNC)’ questionnaire which had been used at our hospital for many years.
Methodology:With IRB approval and written informed patient consents, 197 adult outpatients presenting for gastroenterological procedures were randomlyscreened for OSA risk using both the STOP-Bang and the MNC questionnaires. Spearman’s rank correlation coefficient was used to measure the statistical dependence of the scores calculated from the two questionnaires.
Results:The Spearman’s correlation between the STOP-Bang questionnaire score and the MNC questionnaire score was 0.82 (p < 0.001).
Conclusions:There is a strong correlation between the STOP-Bang and the MNC questionnaires as demonstrated in this study.Our successful experience with the MNC questionnaire justify conduction of a randomized controlled trial to test the validity of the MNC questionnaire.
Keywords:Sleep Apnea, Obstructive;Apnea; Screening;Questionnaires.
Citation:Hannallah M, Exeter Y, Scher L, Habib G, Hwang G, Cai L. Comparison of “the STOP-Bang” and “the Modified Neck Circumference” obstructive sleep apnea screening questionnaires. Anaesth Pain & Intensive Care 2015;18(2):153-55
INTRODUCTION
Patients with obstructive sleep apnea (OSA) are at risk of developing perioperative respiratory complications.1 Definitive diagnosis of OSA requires undergoing sleep studies. In the absence of a definitive diagnosis, several questionnaires have been developed to screen patients in an attempt to identify those who are at high risk of having OSA.2
For several years the Modified Neck Circumference (MNC) questionnaire, which was developed by Flemons3 (Box 1), was used to screen preoperative patients for OSA risk at MedStar Georgetown University Hospital (MGUH). It is simple to use and is felt to be reliably sensitive and specific in identifying patients at high risk of having OSA.
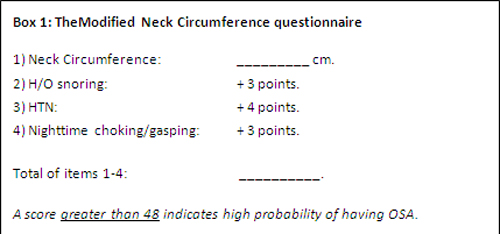
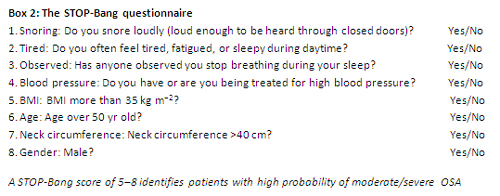
Its sensitivity and specificity, however, have only been validated on a limited scale. With the introduction of MedConnect electronic medical records system, MGUH adopted the STOP-Bang questionnaire4 to screen preoperative patients for OSA risk. The STOP-Bang questionnaire (Box 2) is the most widely used OSA questionnaire. It has been validated by large prospective clinical trials. While highly sensitive in prediction of OSA risk, its specificity is not as strong. While the specificity improved by using a higher score, we found that upon conversion to the STOP-Bang questionnaire, the diagnosis of OSA risk at our hospital increased significantly compared to when the MNC questionnaire was used.
Over-diagnosing OSA risk in the surgical patient has significant implications since it affects the choice of anesthesia, monitoring requirements, and discharge criteria. Having experienced both questionnaires, we feel that the MNC questionnaire deserves to be validated prospectively. As a preliminary step, this study was designed to determine the degree of correlation between the two questionnaires in measuring OSA risk.
METHODOLOGY
With IRB approval and written informed patient consent, 197 random adult outpatients presenting for elective gastrointestinal procedures were screened for OSA risk using both the STOP-Bang and the MNC questionnaires. Since the snoring question is asked differently in the two questionnaires, patients were asked about snoring twice: 1) Do you snore in your sleep? (As asked in the MNC questionnaire). 2) Do you snore loud enough to be heard through closed doors? (As asked in the STOP-Bang questionnaire).
Spearman’s rank correlation coefficient was used to measure the statistical dependence of the scores calculated from the two questionnaires.
RESULTS
The Spearman’s correlation between the STOP-Bang questionnaire score and the MNC questionnaire score is 0.82 (p < 0.001). Figure 1 shows the scatterplot of both sets of scores.
Figure 1: Scatterplot of the stop bang questionnaire score and the modified neck circumference questionnaire score.
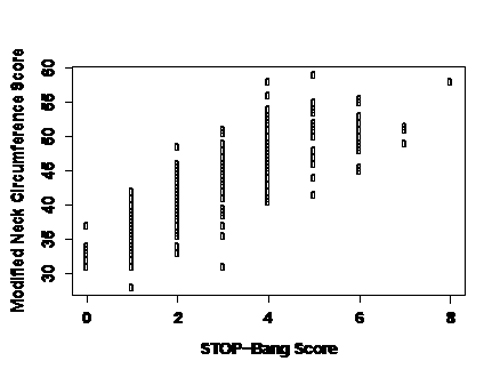
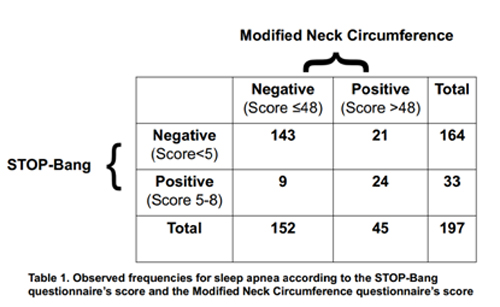
Table 1 shows the contingency table of classification of whether a patient is high risk of having OSA according to the two questionnaires: STOP-Bang score (positive if 5-8) and MNC score (positive if >48). For the MNC questionnaire, the positive percent agreement relative to the STOP-Bang questionnaire is 0.73 (95% CI = 0.54, 0.87); the negative percent agreement relative to the STOP-Bang questionnaire is 0.87 (95% CI = 0.81, 0.92).
Thirty three patients had a STOP-Bang score of 5-8, signifying high risk of having OSA. If the simple “Do you snore in your sleep?’ question was asked instead of “Do you snore loud enough to be heard through closed doors?” 52 patients would have had a STOP-Bang score of 5-8 instead.
DISCUSSION
The STOP-Bang questionnaire is widely used to screen preoperative patients for obstructive sleep apnea (OSA). Its sensitivity and specificity in predicting the probability of OSA has been validated by large prospective and randomized trials. At a score of 3 or more it has high sensitivity but poor specificity. Although the specificity improves at a score of 5-8, certain aspects of the STOP-Bang questionnaire could compromise its accuracy. One is the fact that it gives the same point value to factors that may have different clinical significance. For example, a hypertensive male over the age of 50 will have the same STOP-Bang score as a middle aged female who has a BMI >35 kg m−2, a neck circumference >40 cm and who snores loudly. Clinically, these 2 patients are likely to have different OSA risks. Secondly, the STOP-Bang questionnaire gives the same point value to patients within a wide range of a risk condition. As an example, a patient with a neck circumference of 40 cm will get 0 points, a patient with a neck circumference of 41 cm will get 1 point, so will a patient with a neck circumference of 55 cm. Intuitively, the OSA risk in the first 2 patients should be similar, while that between the 2nd and 3rd patients should be different.
The MNC questionnaire emphasizes the value of neck circumference, the larger the neck circumference the higher the OSA risk. Hypertension, snoring and night chocking, conditions known to be associated with OSA risk, add numeric values to that of the neck circumference. It is not very clear on what basis Flemons assigned these numeric values. In addition, the MNC questionnaire has not been validated by a large prospective trial. Nonetheless, based on our successful clinical experience with that questionnaire, we feel that a prospective large validation trial may prove its reliability in predicting patients with OSA.
CONCLUSION
This study demonstrated strong correlation between the STOP-Bang and the Modified Neck Circumference questionnaires which justifies the conduction of an independent prospective trial to test the validity of the Modified Neck Circumferencequestionnaire.
This study also demonstrates that the way, in which the question about snoring is phrased in the two questionnaires,has important effect on the final obstructive sleep apnearisk score.
REFERENCES
- Chung SA, Yuan H, Chung F. A systemic review of obstructive sleep apnea and its implications for anesthesiologists. AnesthAnalg 2008;107:1543-63.
[PubMed]doi: 10.1213/ane.0b013e318187c83a. - Abrishami A, Khajehdehi A, Chung F. A systematic review of screening questionnaires for obstructive sleep apnea.Can J Anaesth 2010;57(5):423-38.
[PubMed]doi: 10.1007/s12630-010-9280-x. - Felmons W. Obstructive sleep apnea. N Engl J Med 2002;347:498-504.
[PubMed][Free full text] DOI: 10.1056/NEJMcp012849 - Chung F, Subramanyam R, Liao P, Sasaki E, Shapiro C, Sun Y. High STOP-Bang score indicates a high probability of obstructive sleep apnoea.Br J Anaesth 2012;108(5):768-75.
[PubMed][Free full text]doi: 10.1093/bja/aes022.



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube