
Aamer Mahmood Malak1, Asad Shameem2, Chaudhary Amjad Ali1, Muhammad Arslan Qureshi1
1Consultant Anesthesiologist, Combined Military Hospital, Multan Cantt 60000 (Pakistan)
2 Consultant Anesthesiologist, PNS Hafeez, E-8, Islamabad-44000 (Pakistan)
Correspondence: Brig Dr Aamer Mahmood Malak, House No. 250, Street No 13 Chaklala Scheme 3, Rawalpindi-46000 (Pakistan); Phone: +92 333 5208339; E-mail: aamer@doctor.com
ABSTRACT
Objective: Postoperative nausea and vomiting (PONV) is the most common postoperative complication among patients undergoing laparoscopic procedures, because of the formation of pneumoperitonium during laparoscopic procedures. A number of antiemetic drugs have been used to prevent PONV after laparoscopic cholecystectomy. In this study, we evaluated the safety and efficacy of ondansetron, cyclizine and prochlorperazine in preventing PONV in patients undergoing laparoscopic cholecystectomy (LC).
Methodology: In this randomized single blinded controlled trial, we included 195 patients who underwent elective laparoscopic cholecystectomy having ASA status I or II. Selected patients were randomly divided into three equal groups of participants: Group O patients were given ondansetron (4 mg) for the prevention of PONV, Group C patients received cyclizine (50 mg), and Group P patients were given prochlorperazine (10 mg). All groups received their PONV drugs in identical 50 ml syringes. General anesthesia was given to all patients. Metoclopramide was used as a rescue antiemetic drug in all patients. Incidence of PONV within 24 hours, need of rescue anti-emetics and adverse effects e.g. headache, dizziness and sedation within 6 hours after surgery were the focused study outcomes. Comparative analysis was done by Chi-square test or Fischer’s exact test as needed. ANOVA test was used to compare quantitative variables between the three groups. P < 0.05 was considered to be significant.
Results: There was no significant difference in age, gender, ASA status, and BMI of study participants between three groups. The incidence of nausea was 5 (7.7%) in ondansetron group, 3 (4.6%) in cyclizine group and 5 (7.7%) in prochlorperazine group of patients. Vomiting occurred in 6 patients (9.2%) in Group O, 7 patients (10.8%) in Group C and 3 patients (4.6%) in Group P (p-value 0.67). Rescue anti-emetics were required in 5 patients (7.7%) in Group P, in 4 patients (6.2%) in Group C and in 7 patients (10.8%) in Group O (p-value 0.72). The number of adverse effects, such as headache, dizziness and sedation, were high in Group P as compared to the Group C and Group O but this difference was statistically insignificant (p-value 0.79, 0.63 & 0.91 respectively).
Conclusion: Ondansetron, cyclizine and prochlorperazine are equally effective in reducing the incidence of PONV after laparoscopic cholecystectomy with acceptable safety profile.
Key words: Ondansetron; Cyclizine; Prochlorperazine; Postoperative nausea and vomiting
Citation: Malak AM, Shameem A, Ali CA, Qureshi MA. Comparison of ondansetron, cyclizine and prochlorperazine for PONV prophylaxis in laparoscopic cholecystectomy. Anaesth Pain & Intensive Care 2017;21(4):453-457
Received: 16 Aug 2017; Reviewed: 20 Aug, 6, 8 Dec 2017; Corrected: 17 Sep, 01 Dec 2017,; Accepted: 6 Dec 2017
INTRODUCTION
Postoperative nausea and vomiting (PONV) are the second most common presenting complaints of surgical patients after pain.1,2 The incidence of these two varies from 30% to 50% and can be as high as upto 80% in high-risk patients.3 PONV is most common among patients who underwent laparoscopic procedures, because of the formation of pneumoperitonium during laparoscopic procedures.4 The most commonly reported consequences of PONV in laparoscopic patients include; bleeding from surgical sites, rupture of skin stitches, alkalemia, aspiration pneumonia and dehydration.5,6 All these complications may lead to additional burden on health care facility resources and increase in length of hospital stay.
Despite many advancements in anesthesia induction techniques, the incidence of PONV is still high. A number of antiemetic drugs have been used to prevent PONV after laparoscopic cholecystectomy (LC).7 Ondansetron, cyclizine and prochlorperazine are three commonly used drugs for the prevention of PONV. These drugs all act by different mechanisms; ondansetron is a serotonin receptor antagonist (SRA), cyclizine is a histamine H1 receptor antagonist and prochlorperazine perhaps exerts its effects by acting on dopamine receptors. All the three drugs are well-proven drugs in prevention of PONV.8-10 However, literature has mixed evidence in finding the safest and the most effective drug. In this study, we evaluated the safety and efficacy of ondansetron, cyclizine and prochlorperazine in preventing the PONV in patients undergoing LC.
METHODOLOGY
In this randomized single blinded controlled trial, we included 195 patients, ASA status I or II, who underwent LC, of 20 to 60 years and of any gender. This sample size was calculated by taking the average incidence of nausea in 81% patients receiving ondansetron and 56% in patients receiving prochlorperazine,11 by taking α 5% and 1-β 80%, sample size was 61 patients in each group. So we included 65 patients in each group in this study. The study was approved by ethical review committee of our hospital. Patients with ASA status III or IV, those who underwent emergency LC, patients having history of peptic ulcer disease, reflex esophagitis, already taking anti-emetic drugs, pregnant female patients and having allergy to any of these drugs were excluded. All patients were first informed about study protocol before they signed a written informed consent. The setting of this study was department of surgery of our hospital and the duration was 01 March to 25 December 2016.
Patients were admitted one day before surgery. A consultant anesthesiologist who was unaware of study protocols did the pre-anesthesia evaluation of study patients. Patients were kept NPO for at least 6 hours before anesthesia induction. After taking the patient to operating room (OR), intravenous (IV) access was achieved by inserting a 16-20 Gauge IV cannula. Pulse oximetry, ECG and non-invasive blood pressure monitoring was done in all patients during and after induction of anesthesia. Lactated ringer and Gelofusine™ solution was used for fluid replacement during surgery. In all patients anesthesia induction was done by giving 2 mg/kg of 1% propofol and 0.04 mg/kg of midazolam along with 100% oxygen. In all patients, endotracheal tube (size ranging from 7.5 to 8.5 mm) was inserted using an appropriate sized laryngoscope blade to achieve tracheal intubation after adequate relaxation with atracurium bromide (0.03-0.5 mg/kg).
A staff nurse outside the OR, who was blinded to the patient selection, prepared study drugs in a 50 ml syringe. All the three drugs were prepared in similar syringes to prevent biasedness in the study. We made three groups of participants; Group O patients were given ondansetron (4 mg) for the prevention of PONV, Group C patients received cyclizine (50 mg), and Group P patients were given prochlorperazine (10 mg). Anesthesia was maintained by inhalational anesthetics, i.e. isoflurane 1.2%, and atracurium bromide (0.08-0.1 mg/kg) was given if needed after 40-45 min of anesthesia induction.
After completion of LC, anesthesia was reverted by giving neostigmine and glycopyrrolate. Gentle suctioning of secretions through endotracheal tube (ETT) was done before removing the ETT to clear the airway.
Senior anesthesiologists, who were unaware of the group assigned to these patients, noted incidence of PONV within 24 hours after surgery. Diagnosis of PONV was made on verbal communication with patient by asking either he/she have experienced any of these. The following definitions were used to define nausea and vomiting; an unpleasant feeling accompanying the urge to vomit was taken as nausea and the forceful ejection of gastric contents was noted as vomiting. Requirement of additional antiemetic drugs to prevent PONV was also noted. Metoclopramide was used as a rescue antiemetic drug in all patients if additional need of antiemetic drug was needed in any patient. Adverse effects of these drugs such as headache, dizziness and restlessness were noted within first 6 hours of surgery.
SPSS v23 was used for analysis of study data. Comparison of PONV, need of rescue antiemetic and adverse effects between Group O, P and C was Chi-square test or Fischer’s exact test if needed. ANOVA test was used to compare quantitative variables between the three groups. P-value < 0.05 was considered to be was significant.
RESULTS
In this study, there was no significant difference in age, gender, ASA status, and BMI of study participants between all of the three groups. The mean duration of surgery and duration of general anesthesia was also not statistically significant between the groups (p-value 0.11 and 0.13 respectively) (Table 1).
Incidence of nausea and vomiting was little higher in ondansetron and prochlorperazine group of patients as compared to cyclizine group. Incidence of nausea in ondansetron group was 5 (7.7%), 3 (4.6%) in cyclizine group and 5 (7.7%) in prochlorperazine group of patients. Vomiting occurred in 6 (9.2%) patients in Group O, 7 (10.8%) patients in Group C and 3 (4.6%) patients in Group P. This difference in the incidence of PONV between study groups was statistically not significant (p-value 0.67) (Figure 1).
Table 1: Demographic data and study variables
| Variable | Group O
(N=65) |
Group C
(N=65) |
Group P
(N=65) |
p-value |
| Age (y) | 47.2 ± 7.6 | 47.7 ± 8.9 | 46.4 ± 9.6 | 0.70 |
| Female/Male Gender (n) | 52/13 | 45/20 | 46/19 | 0.30 |
| ASA I/II (n) | 50/15 | 56/9 | 52/13 | 0.39 |
| BMI | 26.2 ± 3.8 | 26.3 ± 4.3 | 25.6 ± 3.9 | 0.67 |
| Anesthesia duration (min) | 104.6 ± 6.6 | 106.8 ± 7.5 | 105.4 ± 5.7 | 0.13 |
| Surgery duration (min) | 84.8 ± 6.6 | 83.2 ± 6.5 | 85.4 ± 5.6 | 0.11 |
Data given as mean ± standard deviation
Rescue anti-emetic was required in 5 (7.7%) patient in Group P, in 4.0 (6.2%) patients in Group C and in 7 (10.8%) patients in Group O. Number of adverse effect such as headache, dizziness and sedation were higher in Group P as compared to the Group C and Group O but with statistically insignificant difference (Table 2).
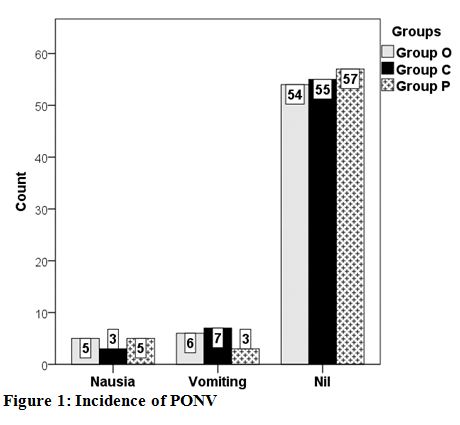
Figure 1: Incidence of PONV
Table 2: Comparative frequency of adverse effects
| Adverse effect | Group O
(N=65) |
Group C
(N=65) |
Group P
(N=65) |
p-value |
| Headache | 3 (4.6) | 3 (4.6) | 5 (7.7) | 0.79 |
| Dizziness | 2 (3.1) | 4 (6.2) | 5 (7.7) | 0.63 |
| Sedation | 3 (4.6) | 2 (3.1) | 4 (6.2) | 0.91 |
| Need of rescue anti-emetics | 7 (10.8) | 4 (6.2) | 5 (7.7) | 0.72 |
Data given as n (%)
DISCUSSION
Laparoscopic cholecystectomy is now a preferred technique for the treatment of cholecystitis with very smaller number of operative complications. It is most commonly performed under general anesthesia that is an independent risk factor of PONV in early surgical period. Moreover, the risk of PONV is increased in patients who underwent laparoscopic procedures because of the creation of pneumoperitonium in these patients. In addition to these there are several other factors that can predispose a patient to PONV such as; previous history of nausea and vomiting, young age, female gender, choice of anesthetic drugs and duration and type of surgery.7,12 Several anti-emetic drugs are used for the prevention of PONV in patients undergoing laparoscopic cholecystectomy. In this study, we evaluated the efficacy and safety of ondansetron, cyclizine and prochlorperazine in patients of LC.
In this study, we took patients having similar baseline characteristics e.g. age, gender and BMI in all groups to minimize the biasedness. In our study, there was no statistically significant difference in the incidence of PONV between the groups. However, incidence of PONV was comparatively less in cyclizine group of patients as compared to the other groups and 6.2 patients required rescue anti-emetics for the prevention of PONV in this group. In Group O 10.8% patients required rescue anti-emetics and 7.7% patients in Group P required additional dose of anti-emetic drugs. On the other hand, incidence of adverse effects e.g. headache, dizziness and sedation was little in Group P patients (7.7%, 7.7% and 6.2% respectively) as compared to 4.6%, 6.2% and 3.1% resp. in Group C and 46%, 3.1% and 4.6% resp. in Group O.
Cholwill et al.13 compared ondansetron with cyclizine and concluded that both these drugs are equally effective and safe in prevention of PONV in laparoscopic gynecological procedures. Chen et al.(11)reported that prochlorperazine is superior to the ondansetron in reducing the incidence of PONV after hip or knee replacement procedures. Chang et al.14 also reported similar results and they stated that prochlorperazine is also a cost effective drug as compared to ondansetron and it significantly reduces the cost of anti-emetics used during surgery. Some studies have stated that cyclizine and ondansetron are superior to dexamethasone and metoclopramide in reducing the risk of PONV after surgical procedures.15,16 Dundee et al.17reported that cyclizine is a better drug for the prevention of PONV as compared to perphenazine for the management of PONV.
Some studies have conclude that choice of the anesthetic drugs also have a major influence of the PONV. According to these studies, inhalational anesthetics and opioids increases the risk of PONV.18 Zhang et al.19 reported that maintenance of general anesthesia with sevoflurane alone increases the risk of PONV after surgery and maintenance with propofol alone or propofol with sevoflurane significantly reduces of PONV. Turkistani et al.20 have reported that pre-operative fluid overload significantly reduces risk the PONV and fluid deficit during surgery is a major contributor to PONV.
So different studies have found different methods and treatments strategies to reduce the incidence of PONV after open or laparoscopic procedures. Nevertheless, PONV is still a major problem for both the surgeon and the anesthetist because it significantly delays the wound healing process and increases the hospital stay of the operated patients.
LIMITATIONS
Our study needed to be designed around disproving our null hypothesis. We have not used statistical tests meant to prove non-inferiority, like the TOST procedure, failing which our study is likely to be under powered.
CONCLUSION
In this study, we have concluded that ondansetron, cyclizine and prochlorperazine are equally effective in reducing the incidence of PONV after laparoscopic cholecystectomy with acceptable safety profile.
Conflict of interest: Nil declared by the authors
Authors’ contribution:
AMM & CAA- Concept, data collection
AS – Data analysis
MAQ – Data collection
REFERENCES
- Park S, Cho E. A randomized, double-blind trial of palonosetron compared with ondansetron in preventing postoperative nausea and vomiting after gynaecological laparoscopic surgery. J Int Med Res 2011;39(2):399-407. [PubMed]
- Daria U, Kumar V. Qualitative comaparison of Metoclopramide, ordansetron and granisetron alone and in combination with dexamethasone in the prevention of postoperative nausea and vomiting in day care laparoscopic surgery under general anaesthesia. Asian J Pharm. 2012;5:165-7.
- Srivastava A, Niranjan A. Secrets of safe laparoscopic surgery: Anaesthetic and surgical considerations. J Minim Access Surg. 2010;6(4):91.
[PubMed] [Free full text] doi: 10.4103/0972-9941.72593 - Gecaj-Gashi A, Hashimi M, Sada F, Baftiu N, Salihu S, Terziqi H, et al. Propofol vs isoflurane anesthesia-incidence of PONV in patients at maxillofacial surgery. Adv Med Sci. 2010;55(2):308-12. doi: 10.2478/v10039-010-0033-4.[PubMed]
- Aziz N, Naz U, Ilyas M. A comparative study between metoclopramide and dexamethasone for prevention of post operative nausea and vomiting in laparoscopic aroscopic cholecystectomy. J Med Sci. 2011;19(3):129-32. [Free full text] [Free full text]
- Gan TJ. Postoperative nausea and vomiting—Can it be eliminated? JAMA. 2002;287(10):1233-6. [PubMed] DOI: 10.1111/j.1365-2044.2006.04794.x
- Ahmed N, Muslim M, Aurangzeb M, Zarin M. Prevention of postoperative nausea and vomiting in laparoscopic cholecystectomy. J Med Sci. 2012;20(1):33-6.[Free full text]
- Som A, Bhattacharjee S, Maitra S, Arora MK, Baidya DK. Combination of 5-HT3 Antagonist and Dexamethasone Is Superior to 5-HT3 Antagonist Alone for PONV Prophylaxis After Laparoscopic Surgeries: A Meta-analysis. LWW; 2016. [PubMed]
- Johns R, Hanousek J, Montgomery J. A comparison of cyclizine and granisetron alone and in combination for the prevention of postoperative nausea and vomiting. Anaesthesia. 2006;61(11):1053-7. [PubMed]
- Jellish WS, Owen K, Fluder E, Sawicki K, Sinacore J. Patient-controlled analgesia combined with either ondansetron or ondansetron plus prochlorperazine for control of pain and nausea and vomiting in patients undergoing abdominal surgery. J Clin Anesth. 2008;20(8):594-600. [PubMed] doi: 10.1016/j.jclinane.2008.06.008
- Chen JJ, Frame DG, White TJ. Efficacy of ondansetron and prochlorperazine for the prevention of postoperative nausea and vomiting after total hip replacement or total knee replacement procedures: a randomized, double-blind, comparative trial. Arch Int Med. 1998;158(19):2124-8. [PubMed] [Free full text]
- Apfel C, Heidrich F, Jukar-Rao S, Jalota L, Hornuss C, Whelan R, et al. Evidence-based analysis of risk factors for postoperative nausea and vomiting. Br J Anaesth.2012;109(5):742-53. [PubMed] [Free full text] doi: 10.1093/bja/aes276
- Cholwill J, Wright W, Hobbs G, Curran J. Comparison of ondansetron and cyclizine for prevention of nausea and vomiting after day-case gynaecological laparoscopy. Br J Anaesth 1999;83(4):611-4. [PubMed] [Free full text]
- Chang P. Cost-Effectiveness Analysis of Ondansetron and Prochlorperazine for the Prevention of Postoperative Nausea and Vomiting. J Manag Care Pharm 2005;11(4):317-21. [PubMed] [Free full text]
- Nortcliffe SA, Shah J, Buggy D. Prevention of postoperative nausea and vomiting after spinal morphine for Caesarean section: comparison of cyclizine, dexamethasone and placebo. Br J Anaesth 2003;90(5):665-70.[PubMed]
- Sandhu T, Tanvatcharaphan P, Cheunjongkolkul V. Ondansetron versus metoclopramide in prophylaxis of nausea and vomiting for laparoscopic cholecystectomy: a prospective double-blind randomized study. Asian journal of surgery. 2008;31(2):50-4.[PubMed] [Free full text] doi: 10.1016/S1015-9584(08)60057-3.
- Dundee J, Loan W, Morrison J. A comparison of the efficacy of cyclizine and perhenazine in reducing the emetic effects of morphine and pethidine. Br J Clin Pharmacol.1975;2(1):81-5.[PubMed] [Free full text]
- Horn CC, Wallisch WJ, Homanics GE, Williams JP. Pathophysiological and neurochemical mechanisms of postoperative nausea and vomiting. Eur J Pharmacol. 2014;722:55-66. [PubMed] [Free full text] doi: 10.1016/j.ejphar.2013.10.037
- Zhang D, Shen Z, You J, Zhu X, Tang Q-F. Effect of ondansetron in preventing postoperative nausea and vomiting under different conditions of general anesthesia: A preliminary, randomized, controlled study. Ups J Med Sci.2013;118(2):87-90.[PubMed] [Free full text] doi: 10.3109/03009734.2013.768315.
- Turkistani A, Abdullah K, Manaa E, Delvi B, Khairy G, Abdulghani B, et al. Effect of fluid preloading on postoperative nausea and vomiting following laparoscopic cholecystectomy. Saudi J Anaesth 2009;3(2):48. [PubMed] [Free full text] doi: 10.4103/1658-354X.57872



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube