
Nupur Chakravorty, MD1, Devashish Chakravarty, MD, PDCC2, Rashim Vachhani,
DA3, DNB, R. V. Shidhaye, DA, MD4
1Associate Professor; 4Professor
Department of Anesthesiology, L.N. Medical College & J.K. Hospital, Kolar Rd, Chuna Bhatti, Bhopal, Madhya Pradesh
462007, (India)
2Assistant Professor, Department of Anesthesiology, Chirayu Medical College & Hospital, Bhainsakhedi, Bhopal, Madhya Pradesh
462030, (India)
3Assistant Professor, Department of Anesthesiology, C.M. Medical College, Durg District, Kachandur, Chhattisgarh 490024, (India)
Correspondence: Dr. Nupur Chakravorty, MD, Associate Professor Anesthesiology, L.N. Medical College & J.K.
Hospital, Bhopal, Madhya Pradesh, India; Cell: +91 9425011099; E-mail: drnupurc@yahoo.com
ABSTRACT
Introduction: One of the main concerns for the anesthesiologist in obese hypertensive patients is to prevent hypertension, tachycardia and arrhythmias during extubation, and to ensure an awake patient with full airway control and stable hemodynamics. Our aim was to compare the effects of single bolus of intravenous nitroglycerine and intravenous esmolol on hemodynamic response and quality of extubation following tracheal extubation in obese patients posted for elective laparoscopic surgery.
Methodology: 60 ASA PS II and III patients with BMI > 25, undergoing elective laparoscopic cholecystectomy under general anesthesia were randomly divided into two groups: Group E (n=30) received esmolol 2 mg/kg intravenously; Group N (n=30) received nitroglycerine 2 μg/kg before extubation. Heart rate (HR), systolic, diastolic and mean arterial pressures were recorded at time of discontinuation of isoflurane (T0), at time of reversal (T1), before (T2) and after (T3) extubation, 3 min (T4) and 5 min (T5) postextubation. Statistical analysis was done using Stata 11 software. For continuous variables, mean and standard deviations were compared using unpaired t-test. For categorical data chi-square test was applied. For comparison of scores two-sample Wilcoxon rank-sum (Mann-Whitney) test was used. P-value < 0.05 was considered significant. Rate pressure product was calculated and was the primary outcome measure.
Results: HR rate was significantly lower in Group E as compared to Group N at T2 (82.06 ± 13.7 vs 100.31 ± 12.04, p < 0.05), T3 (80.8 ± 8.7 vs 99.06 ± 16.17, p > 0.05) and T4 (67.23 ± 8.68 vs 90.03±8.27, p <0.01). Maximum percentage decline in HR (19.22%) in Group E was seen at T4 compared to T0. Systolic blood pressure was significantly low compared to Group N at T2 (148.9 ± 8.66 vs 155.7 ± 14.81, p < 0.05), T3 (131.9 ± 8.91 vs 137.9 ± 8.86, p < 0.01 and T4 (127.56 ± 9.01 vs 135.63 ± 9.71, p < 0.01). Rate pressure product was significantly lower in Group E at T2, T3 and T4 as compared to Group N. Maximum percentage decline in rate pressure product (23.38%) in Group E was seen at T4 when compared to T0. No significant difference was observed in sedation score, time to extubation or quality of extubation.
Conclusion: Administration of nitroglycerine and esmolol intravenously prior to extubation in obese hypertensive patients is a practical and safe method to ensure stable hemodynamics with good patient awakening and airway control during extubation. Esmolol has a significantly better effect in controlling rate
pressure product.
Keywords: Extubation; Esmolol; Hypertension; Nitroglycerine; Obesity; General anesthesia; Hemodynamic effects; Laparoscopic surgeries
Citation: Chakravorty N, Chakravarty D, Vachhani R, Shidhaye RV. Comparison of esmolol and nitroglycerine on hemodynamic parameters during extubation in obese patients following laparoscopic cholecystectomy: a prospective randomized study. Anaesth Pain & Intensive Care 2015;19(4):437-443
comparison of esmolol and nitroglycerine in obese patients
INTRODUCTION
Emergence from general anesthesia (GA) and tracheal extubation is associated with increased oxygen consumption, catecholamine secretion, tachycardia and hypertension for about 5-15 min.1 In patients with preoperative hypertension cardiovascular responses are more marked than normotensive patients,2 predisposing them to cardiac or cerebral complications.3 Prevention of sympathetic overactivity is essential to maintain hemodynamic stability and reduction of morbidity in these patients.1 In obese hypertensive patients with potential postoperative airway problems, ensuring a fully awake patient with good control of cardiovascular parameters poses a problem for the
anesthetist.
Many drugs have been used with varying success rates to control hemodynamic changes during tracheal intubation and extubation.4,5 Infusions of the antihypertensive drugs esmolol and nitroglycerine have been used in attenuating the pressor response to extubation.6-8
We conducted this study to compare the effects of a single bolus dose of intravenous nitroglycerine with esmolol on hemodynamic responses to extubation and recovery in hypertensive obese patients undergoing laparoscopic surgery. Our primary outcome measure was the efficacy in controlling rate pressure product (RPP) and the maximum percentage decline in RPP in both groups. Quality of extubation was also assessed.
METHODOLOGY
The study was designed as a prospective randomized double blind study. Eighty ASA PS III patients of both sexes, between the ages of 30-65, having BMI > 25, scheduled for laparoscopic cholecystectomy under GA were screened preoperatively. Sixty patients diagnosed with essential hypertension, systolic blood pressure (SBP) > 140 mmHg, diastolic blood pressure (DBP) > 90 mm Hg) on antihypertensive therapy, having normal left ventricular function were included in the study. Preoperative exclusion criteria were patient refusal, patients having heart rate (HR) <50/min, sick sinus syndrome, bronchial asthma, previous intolerance to beta blocker therapy, cerebrovascular disease and atrioventricular block. Institutional ethics committee permission was taken and informed consent regarding interventions was taken from the patients. Method of randomization of patients was block randomization. Subjects were allocated to two groups: Group E and Group N of 30 patients each (n=30).Total 15 Blocks of size 4 each with treatment allocation of 1:1 for Group E and Group N were created with the help of computer software. Coded opaque sealed envelopes (total 15) were used and each envelope was used for four patients leading to random assignment of one subject to one group. In case of deviation from study protocol in any patient due to medical or surgical causes, another patient was given the same envelope and included in the study thus ensuring similar sample size.
Group E patients received a single dose of esmolol (2 mg/kg diluted in 10 ml normal saline IV) (Esocard® Samarth Lifesciences Pvt Ltd.) and Group N to receive inj. nitroglycerine (Nitrocin® Samarth Life sciences Pvt Ltd) 2 μg/kg diluted in 10 ml normal saline IV as a slow bolus at a predetermined time before emergence. Both drugs were prepared in identical syringes and coded by an assistant who was unaware of patient grouping. Postoperative caregivers recording data were also unaware of patients grouping and drugs given thus ensuring blinding.
Standard fasting and premedication guidelines were followed. After securing IV access, necessary monitors were attached (NIBP, ECG, arterial oxygen saturation (SpO2), end tidal carbon dioxide (EtCO2) (Philips Medical Systems VM Sure Sign USA). Baseline HR, SBP and DBP were recorded. Anesthesia was induced with 2 mg/kg propofol, 2 μg/kg fentanyl, and relaxation was achieved with 0.5 mg/kg atracurium IV for endotracheal intubation. Maintenance of anesthesia was done with 50% air in O2, isoflurane (inspired 0.8-1%) and atracurium as required. Mechanical ventilation was adjusted to maintain EtCO2 between 30-35 mmHg. After extraction of gall bladder, isoflurane was discontinued. Muscle relaxant was reversed with neostigmine (0.05 mg/kg) and glycopyrrolate (0.01 mg/kg) at the first spontaneous breath and study drugs were administered to the patients after one minute.
SBP, DBP, mean arterial pressure (MAP) and HR were recorded at discontinuation of isoflurane (T0), at the time of reversal and study drugs administration (T1), just before extubation (T2), immediately post extubation (T3), at 3 min (T4) and 5 min (T5) post extubation.
Rate pressure product at these time intervals was calculated. Sedation was evaluated on a six point Ramsey scale:
1 Anxious, agitated restless or both
2 Cooperative, oriented and tranquil
3 Drowsy but responds to commands
4 Asleep, brisk response to light glabellar tap or loud auditory stimulus
5 Asleep, sluggish response to light glabellar tap or loud auditory stimulus, and
6 Asleep and unarousable.9
The quality of extubation was assessed with a 5-point rating scale where;
1 no cough and normal breathing
2 mild cough
3 moderate cough
4 severe cough and difficulty in breathing, and
5 laryngospasm with severe cough and forced breathing.10
Need for atropine (HR < 40/min) or ephedrine (SBP < 80 mmHg) or additional dose of nitroglycerine or esmolol (SBP > 200 mmHg, DBP > 120 mmHg or HR > 150/min) was recorded. Duration of surgery was taken as time from skin incision to skin closure. Duration of anesthesia was taken as time of unresponsiveness to induction agent to ability to follow verbal commands.
Statistical analysis: Demographic characteristics, hemodynamic parameters, level of sedation and other complications were compared between two groups and data were analyzed statistically using Stata 11 software. For continuous variables, descriptive statistics (mean and standard deviations) were computed. Comparison of means in Group E and Group N was done using unpaired t-test. For categorical data Pearson chi square test was applied. For comparison of scores two-sample Wilcoxon rank-sum (Mann-Whitney) test was used. P value < 0.05 was considered significant.
The sample size could not be calculated before the start of the study due to paucity of similar studies. Post-hoc power analysis was carried out for rate pressure product, HR and SBP between two groups at 5 min post extubation . This study had 100 % power to detect effect size of 3334.2 for rate pressure product , 100% power to detect effect size of 22.8 for HR and 91.57 % power to detect effect size of 8.07 for SBP, between Group E and Group N, assuming alpha error 0.05 (two-sided).
RESULTS
Both groups were comparable as regards their demographics, duration of surgery and duration of anesthesia. (Table 1).
Hemodynamic profile of both groups was comparable at T0 and T1. HR was significantly lower in Group E as compared to Group N at T2 (82.06 ± 13.7 vs 100.31 ± 12.04, p < 0.05), T3 (80.8 ± 8.7 vs 99.06 ± 16.17, p < 0.05) and T4 (67.23 ± 8.68 vs 90.03 ± 8.27, p < 0.05) (Table 2, Fig.1). At T2 3 patients (10%) in Group E had HR >100 compared to 18 (60%) patients in Group N, at T3 1 patient in Group E had HR > 100, compared to 15 (50%) patients in Group N. Maximum percentage decline (19.22%) in HR in Group E was seen at T4 when compared to T0 (67.23 ± 8.68 vs 83.23 ± 5.63). At T5 no statistically significant difference could be observed in HR between both groups.
SBP was significantly lower in Group E as compared to Group N at T2 (148.9 ± 8.66 vs 155.7 ± 14.81, p < 0.05), T3 (131.9 ± 8.91 vs 137.9 ± 8.86, p < 0.01) and T4 (127.56 ± 9.01 vs 135.63 ± 9.71, p < 0.01) (Table 2, Figure 2). Mean DBP and mean pressure were higher in Group E as compared to Group N at T2, T3 but lower at T4 (Table 2). At T5 no statistically significant difference could be observed in arterial pressures between both groups.
Rate pressure product was significantly lower in Group E as compared to Group N at T2 (12524.6 ± 2376 vs 15691 ± 3320, p < 0.01), T3 (10589.53 ± 1245.40 vs. 13717 ± 2631.5, p < 0.01) and T4 (8650 ± 948.77 vs. 11984.2 ± 1653.52, p < 0.01) (Table 2, Figure 3). A maximum percentage decline (23.38 %) in rate pressure product in Group E was seen at T4 when compared to T0 (Fig 3). In Group N rate pressure product increased by 10.64% at T4 compared to T0. At T5 no significant difference was observed between both groups.
Sedation score was comparable in both Groups at T5 (2.8 ± 1.24 in Group E vs. 3.5 ± 1.40 in Group N) (p > 0.05). At T4 bradycardia (PR < 40) was observed in one patient in Group E which was corrected with appropriate doses of glycopyrrolate. Hypotension (SBP < 80 mm Hg) was seen in one patient in Group E and 3 in Group N at T4 which responded to rapid fluid administration and ephedrine. Average time interval in min required to extubate patients after reversal (T1-T2 interval) was comparable (4.43 ± 1.30 min) in Group E compared to and 4.96 ± 1.29 in Group N, p > 0.05). Extubation score 1 was observed in 25 (83%) patients in Group E compared to 24 (81%) in Group N (p > 0.05).
Table 1: Patient characteristics. Data given as Mean ± SD except
where specified
| Variable | Group E
( n = 30) |
Group N
( n = 30) |
|
| Age (years) | 46.8 ± 9.33 | 43.83 ± 8.57 | |
| Height (cm) | 156.8 ± 9.54 | 154.06 ± 6.658 | |
| Weight (kg) | 62.03 ± 9.10 | 62.16 ± 7.77 | |
| BMI (kg/cm2) | 25.52 | 26.22 | |
|
Gender |
Male | 7 (23.33)* | 9 (30)* |
| Female | 23 (76.67)* | 21 (70)* | |
| Duration of surgery(min) | 74.83 ± 21.59 | 76.16 ± 17.93 | |
| Duration of Anesthesia(min) | 82.9 ± 18.99 | 88.3 ± 14.99 | |
Table 2: Comparison of hemodynamic parameters between two groups
<trclass=”row0″>MBP93.26 ± 5.20100.43 ± 7.540.05
| Time interval | Parameters | Group E ( n = 30)
(Mean ± S.D.) |
Group N ( n = 30)
(Mean ± S.D.) |
p value |
| T 0 | HR | 83.23 ± 5.63 | 83.5 ± 5.95 | > 0.05 |
| SBP | 135.66±3.44 | 136.5 ± 4.12 | > 0.05 | |
| DBP | 86 ± 5.55 | 84.26 ± 7.21 | > 0.05 | |
| MBP | 104.21 ± 9.88 | 101.65 ± 5.01 | > 0.05 | |
| Rate Pressure Product | 11289.97 ± 775.9 | 11393.07 ± 810.98 | > 0.05 | |
| T1 | HR | 85.3 ± 12.34 | 83.2 ± 10.12 | > 0.05 |
| SBP | 158.1 ± 10.42 | 155.96 ± 9.12 | > 0.05 | |
| DBP | 96.86 ± 7.38 | 96.46 ± 6.67 | > 0.05 | |
| MBP | 124.76 ± 42.8 | 118.03 ± 12.24 | > 0.05 | |
| Rate Pressure Product | 13366.53 ± 2360.17 | 12918 ± 1777 | > 0.05 | |
| T2 | HR | 82.06 ± 13.7 | 100.31 ± 12.04 | < 0.05 |
| SBP | 148.9 ± 8.66 | 155.7 ± 14.81 | < 0.05 | |
| DBP | 96.9 ± 6.19 | 77.93 ± 6.95 | < 0.05 | |
| MBP | 115.62 ± 6.36 | 103.6 ± 6.17 | < 0.05 | |
| Rate Pressure Product | 12524.6 ± 2376 | 15691 ± 3320 | < 0.01 | |
| T3 | HR | 80.8 ± 8.7 | 99.06 ± 16.17 | < 0.05 |
| SBP | 131.2 ± 8.91 | 137.96 ± 8.86 | < 0.01 | |
| DBP | 98.13 ± 8.88 | 75.46 ± 5.29 | < 0.05 | |
| MBP | 108.91 ± 7.45 | 96.28 ± 4.78 | < 0.05 | |
| Rate Pressure Product | 10589.53 ± 1245.40 | 13717 ± 2631.5 | < 0.05 | |
| T4 | HR | 67.23 ± 8.68 | 90.03 ± 8.27 | < 0.05 |
| SBP | 127.56 ± 9.01 | 135.63 ± 9.71 | < 0.01 | |
| DBP | 76.96 ± 4.83 | 83.63 ± 7.56 | < 0.05 | |
| Rate Pressure Product | 8650 ± 948.77 | 11984.2 ± 1653.52 | < 0.01 | |
| T5 | HR | 86.06 ± 7.43 | 82.9 ± 6.02 | > 0.05 |
| SBP | 131.13 ± 13.70 | 134.03 ± 12.63 | > 0.05 | |
| DBP | 85.4 ± 7.18 | 84.7 ± 7.83 | > 0.05 | |
| MBP | 100.61 ± 6.16 | 101.08 ± 8.06 | > 0.05 | |
| Rate Pressure Product | 11255.1 ± 1320.56 | 11115.7 ± 1352.29 | > 0.05 |
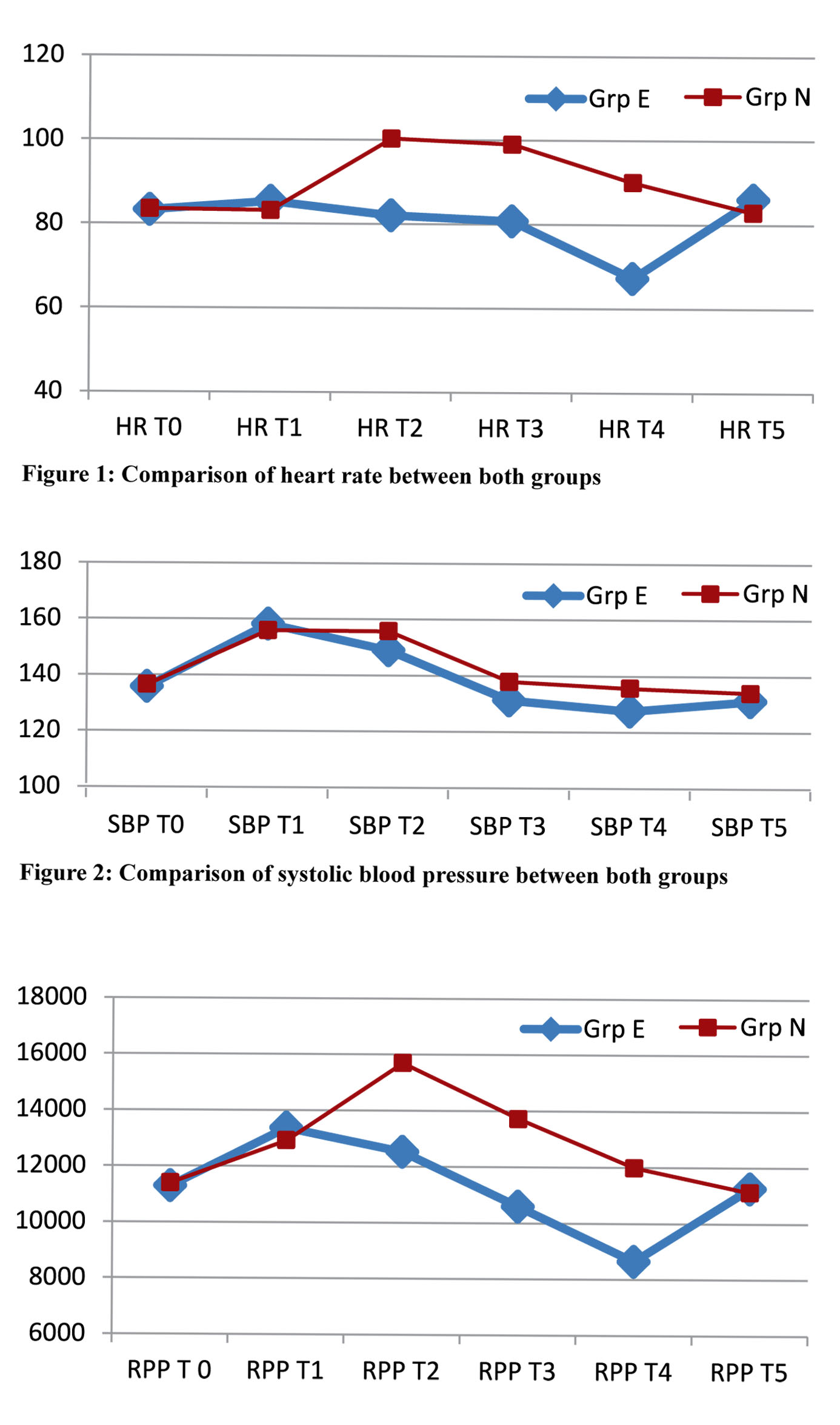 Figure 3: Comparison of rate pressure product between both groups
Figure 3: Comparison of rate pressure product between both groups
DISCUSSION
During laryngoscopy, intubation, and extubation, the plasma concentrations of noradrenaline and adrenaline increase, causing a significant increase in blood pressure and HR. This may result in severe and even life-threatening complications in patients with coronary heart disease and hypertension.11
In our study we compared the effects of a single bolus dose of intravenous nitroglycerine and esmolol on tracheal extubation since both antihypertensive drugs have a rapid onset and short duration of action12 and this time corresponded with the time duration of effect we required avoiding any unwanted side effects. Lowrie et al13 studied the hemodynamic responses after extubation, and found that HR and adrenaline concentration at 5 min after extenuation increased significantly compared with the measurement at the end of the surgery. We emphasised therefore on controlling these parameters at that point of time. In our study we observed maximum decline in SBP and HR with esmolol but not with nitroglyerine at 3 min post extubation (T4). At 5 min post extubation (T5) we observed parameters returning to baseline values. We take into account the fact that a time lapse (4.43 ± 1.30 min in Group E and 4.96 ±1.29 in Group N) had elapsed between drug administration and extubation which accounts for these observations.
Unal et al14 compared effects of an esmolol infusion with placebo during and after extubation in spine surgeries. They observed that at as compared to placebo, esmolol had a better control on MAP and HR during extubation and upto 10 min post extubation. However when compared to nitroglycerine in our study esmolol was less effective in controlling MAP at all observation periods except at T4. We understand that the difference in findings may be due to the fact that Unal et al14 compared esmolol to a placebo.
The significant decline in MAP and DBP with esmolol at T4 as compared to nitroglycerin, an observation in contrast with those at previous intervals may be because of the declining effect of nitroglycerine which has a shorter duration of action compared to esmolol.
The incidence of adverse cardiac events during comparison of esmolol and nitroglycerine in obese patients intubation and extubation in patients undergoing different surgical operations has been reported to be similar.3 Rate pressure product (RPP) measures stress put on cardiac muscle and is an index of myocardial oxygen consumption. A high (RPP) has been found to be significantly correlated with increased morbidity immediately before tracheal extubation and 1 minute after tracheal extubation.3 This was why we analysed rate pressure product as our primary endpoint in control of cardiovascular parameters.
We observed a steady decline in RPP and HR in Group E after giving the drug. Mean maximum decline in both values at 3 min post extubation (T4), correlates with the peak action of esmolol, followed by a rise and return to baseline values
at 5 min post extubation. The increase in HR and rate pressure product at T4 in Group N was an undesirable observation, questioning the use of nitroglycerine under these circumstances.
Unlike intubation, time of extubation is not a fixed entity which could raise the question of timing of drug administration. Singhal et al15 found esmolol to be most effective in attenuating hemodynamic responses to intubation when it was administered 3 min prior to laryngoscopy. Other authors mention that intravenous esmolol 1.5 mg/kg given 2-5 min before extubation is effective.16 However we administered both drugs with reversal at first spontaneous breath and found time to extubation to be comparable. Thus we could compare the action of both drugs with respect to their pharmacokinetics.
We used a dose of 2 mg/kg of esmolol compared to 1.5 mg /kg in the study by Singhal et al.15 Dyson el al7 found a bolus dose of esmolol of 1.5 mg/kg as optimal for controlling both the SBP and HR responses to extubation. They observed distinct hypotension with a dose of 2 mg/kg. However we observed no such finding in our study.
Pérez Peña JM17 compared intravenous nitroglycerine in a dose of 2 μg/kg with a control group and found it to effectively prevent increases in SBP and rate pressure product during and after intubation. They did not observe any significant difference in control of increases in diastolic pressure or HR modification at any time interval. In our study we compared nitroglycerine with esmolol and this was probably why we found HR to be significantly higher in Group N for upto 3 min post extubation.
The time elapsed between administration of study drugs and extubation (T1-T2) in our study implies that at 5 min post extubation (T5), action of both may have declined, which explains the lack of significant difference between all parameters between both groups at T5. Complications like hypotension, bradycardia were a direct pharmacological response to the drugs and easily treatable. Sedation scores were comparable between groups, as was time to extubation and quality of extubation. Single bolus doses of nitroglycerine do not cause sedation which is a known side effect of nitroglycerine infusions. These positive observations fulfilled our aim of extubating obese patients when they were awake without increases in hemodynamic parameters.
We realize that the administration of single bolus doses of short acting drugs is in contradiction to their pharmacokinetics and raises questions as to their efficacy. However we feel that the short duration of action required was adequately fulfilled by a single bolus dose. It would have been preferable to measure the plasma levels of drugs at the mentioned time intervals to study the onset, peak and offset with relation to extubation in both groups but we were not able to do so due to lack of facilities for the same.
CONCLUSION
We conclude that a single intravenous bolus of both, esmolol or nitroglycerine, before extubation is effective in attenuating hemodynamic changes due to cardiovascular stimulus in obese hypertensive patients and facilitate smooth extubation. However, esmolol 2 mg/kg is more effective than nitroglycerine 2 μg/kg for attenuating the systolic blood pressure and heart response to extubation and had a more beneficial effect on rate pressure product in these patients.
Conflict of interest: None declared by the authors.
Authors’ Contribution:
NC: Concept, patient selection, conduction of study.
DC: Manuscript writing.
RV: Data collection.
RVS: Manuscript editing and statistical analysis
REFERENCES
- Miller KA, Harkin CP, Bailey PL. Postoperative tracheal extubation. Anesth Analg1995;80:149-72. [PubMed]
- Stone JG, Foex P, Sear JW, Johnson LL, Khambatta HJ, Triner L. Risk of myocardial ischemia during anaesthesia in treated and untreated patients. Br J Anaesth 1988;61(6):675-679. [PubMed]
- Edwards ND,Alford AM, Dobson PM, Peacock JE, Reilly CS. Myocardial ischaemia during tracheal intubation and extubation. Br J Anaesth. 1994 Oct;73(4):537-9. [PubMed]
- Mikawa K, Nishina K, Takao Y, Shiga M, Maekawa N, Obara H. Attenuation of cardiovascular responses to tracheal extubation: Comparison of Verapamil, Lidocaine and Verapamil-Lidocaine combination. Anesth Analg 1997;85:1005-10. [PubMed]
- Nho JS, Lee SY, Kang JM, Kim MC, Choi YK, Shin OY, et al. Effects of maintaining a remifentanil infusion on the recovery profiles during emergence from anaesthesia and tracheal extubation. Br J Anaesth 2009;103:817-21. doi: 10.1093/bja/aep307 [PubMed]
- Muzzi DA, Black S, Losasso TJ, Cucchiara RF. Labetalol and esmolol in control of hypertension after intracranial surgery. Anesth Analg 1990;70:68-71. [PubMed]
- Dyson A, Isaac PA, Pennant JH, Giesecke AH, Lipton JM. Esmolol attenuates cardiovascular responses to extubation. Anesth Analg 1990;71:675-8. [PubMed]
- Dutta S, Rudra A, Ray M, Sarkar A, Mitra D. Haemodynamic changes during intubation and extubation in patients with mitral stenosis: Effects of Nitroglycerin and Esmolol. Ind J Anaesth 1999 June;43(3):45-53.
- Ramsay MA, Huddleston P, Hamman B, Tai S, Matter G. The patient state index correlates well with the Ramsay sedation score in ICU patients. Anesthesiology 2004;101:A338.
- Turan G, Ozgultekin A, Turan C, Dincer E, Yuksel G. Advantageous effects of dexmedetomidine on haemodynamic and recovery responses during extubation for intracranial surgery. Eur J Anaesthesiol 2008;25: 816-20. doi: 10.1017/S0265021508004201 [PubMed]
- Kayhan Z, Aldemir D, Mutlu H, Oğüş E. Which is responsible for the haemodynamic response due to laryngoscopy and endotracheal intubation? Catecholamines, vasopressin or angiotensin? Eur J Anaesthesiol 2005;22:780-5. [PubMed]
- .Gorczynski RJ, Shaffer JE, Lee RJ. Pharmacology of ASL-8052, a novel beta-adrenergic receptor antagonist with an ultra short duration of action. Journal of Cardiovasc Pharmacol 1983;5:668-77. [PubMed]
- Lowrie A, Johnston PL, Fell D, Robinson SL. Cardiovascular and plasma catecholamine responses at tracheal extubation. Br J Anaesth1992;68:261-263. [PubMed]
- Unal Y, Ozsoylar O, Sariguney D, Arslan M, Yardim RS. The efficacy of esmolol to blunt the haemodynamic response to endotracheal extubation in lumbar disc surgery. Res J Med Sci.2008;2(2):99-104.
- Singhal SK, Malhotra N, Kaur K, Dhaiya D. Efficacy of esmolol administration at different time intervals in attenuating hemodynamic response to tracheal intubation. Indian J Med Sci.2010 Oct;64(10):468-75. [PubMed]
- Karmarkar S, Varshney S. Tracheal extubation. Contin Educ Anaesth Crit Care Pain 2008;8(6):214-220.
- Pérez Peña JM, Olmedilla Arnal L, Jimeno Fernández C, Navia Roque J. Effect of an intravenous nitroglycerine bolus on the hemodynamic impact of laryngoscopy and intubation. Rev Esp Anestesiol Reanim 1991;38(4):234-7.



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube