
Pouran Hajian*, Navid Haddadzadegan**, Mahshid Nikouseresht***,
Mohamad-Ali Seif-Rabiee****, Alireza Yavarikia******
*Assistant Professor & Head; **Resident; ***Assistant Professor, Fellowship of Pain Medicine
Department of Anesthesiology, Fatemia Hospital, Hamedan University of Medical Sciences, Hamedan, IRAN
****Assistant Professor
Department of Community Medicine, Hamedan University of Medical Sciences, Hamedan, IRAN
*****Assistant Professor
Department of Orthopedic Surgery, Hamedan University of Medical Sciences, Hamedan, IRAN
Correspondence: Navid Haddadzadegan MD, department of anesthesiology, Besat Hospital, Hamedan, Iran; Tel: +989121145268; Email: aramgol@gmail.com
ABSTRACT
Background & Aims: Incidence of anterior cruciate ligament (ACL) tearing is especially high in athletes, and reconstruction surgery is often required, associated with severe post-operative pain requiring active interventions. In the present study we compared the continuous intravenous morphine infusion technique with femoral nerve block regarding efficacy of pain management and patients’ satisfaction, so that the best post-operative pain management for ACL reconstruction can be decided.
Methodology: We recruited 54 patients for this study and divided them randomly in 2 equal groups; Group-A (continuous intravenous morphine infusion) and Group-B (femoral nerve block). Femoral block for coded subjects was performed at the end of the surgery right before shifting the patient. For patients in the other group, catheter was inserted for continuous infusion after extubation and transfer to recovery room. Pain intensity was assessed and recorded in recovery service and right after complete consciousness, and then every 4 hours by trained nurses of the department, using visual analogue scale (VAS). After complete consciousness and every 12 hours, patients’ satisfaction from post-operative analgesia was questioned and recorded, using five Likert scale items. Post-operative complication were recorded.
Results: The pain in Group-A (the continuous infusion pump group) at 20 and 24 hours after surgery was significantly lower than Group-B (nerve block group) (p<0.05). Post-operative complications (especially nausea) in femoral nerve block was lower.
Conclusion: Analgesic degree of nerve block is comparable with the impact of continuous infusion pump at least during 20 hours after anterior cruciate ligament reconstruction surgery.
Keywords: Post-operative pain; Pain management; Continuous infusion pump; Femoral nerve block; Anterior cruciate ligament; ACL reconstruction surgery
Citation: Hajian P, Haddadzadegan N, Nikouseresht M, Seif-Rabiee MA, Yavarikia A. Comparison of analgesic effect of femoral nerve block and continuous intravenous infusion pump, after anterior cruciate ligament reconstruction in first postoperative day. Anaesth Pain & Intensive Care 2014;18(3):250-255
INTRODUCTION
Anterior Cruciate Ligament (ACL) is one of major ligaments that stabilizes the knee joint and is critical for its stability during running and sports activities.1 Since the incidence of ACL tearing is especially high in young athletes, reconstruction surgery may be required in physically active individuals.2 Indirect repair of the anterior cruciate ligament is not very successful and Conservative non-surgical treatment is not satisfactory in active people, thus surgery is considered an effective treatment for those Young people and those with a high excersise level who need to return to the same level of activity.3
The majority of orthopedic patients experience post-operative pain. Incidence of pain directly affects patients’ quality of life in terms of patient physiology, psychology, and social characteristics.
Severe pain not only causes discomfort and suffering, but also prevents the patient from resuming his or her daily activities, which can be of major socio- economic relevance. Besides, insufficient postoperative pain therapy may have a negative impact on perioperative morbidity and mortality and decrease the postoperative quality of life.4
Pain is also one of the primary concerns of the surgeon because of its close ties with clinical outcome and acute postoperative patient well-being. Negative clinical outcomes resulting from ineffective postoperative pain management include deep vein thrombosis, pulmonary embolism, coronary ischemia, myocardial infarction, pneumonia, poor wound healing, insomnia, and demoralization Associated with these complications are economic and medical implications, such as extended lengths of stay, readmissions, and patient dissatisfaction with medical care.5-8
During last few years, major breakthroughs with potential to considerably improve the field of postoperative analgesia have occurred and are still in progress.9 Advances in the knowledge of molecular mechanisms have led to the development of multimodal analgesia and new pharmaceutical products to treat postoperative pain. Newer postoperative patient-controlled analgesia (PCA) in ways such as, regional, transdermal, and pulmonary, presents another interesting opportunity of development.10, 11 Local anesthetic techniques and for the most part, peripheral nerve blocks, are effective and safe if appropriate patient selection is done and will be one of the foundations of postoperative pain controlling.
At present, various methods of drug delivery are used, of which intravenous catheters, epidural and peripheral nerve block can be pointed12).
Peripheral nerve blocks also have proven to be effective in treating acute pain, thereby minimizing the requirement for opiate analgesics10).
Recently, femoral nerve block, both single-injection and continuous modalities, proved effective postoperative pain control in the lower extremity surgeries, it is a standard analgesic intervention following total knee arthroplasty or anterior cruciate repair in many centers.5,7,9-10
Given that the degree of neural blockage is proportional to the amount of local anesthetic, the anesthetic should be injected as close to the nerve sheath as possible (but not intraneuronal). However, its principal disadvantage is the resulting motor weakness that may contribute to impaired ambulation and rehabilitation.13-14
The duration of single-injection femoral nerve block is limited to last 12 to 24 hours (depending on the type of local anesthetic). Prolonged analgesia can be achieved with continuous femoral nerve block. However, it requires additional skill, time, and postoperative management, and furthermore, the placement of femoral nerve catheter involves the risk of infection and nerve injury. Although femoral nerve block has gained popularity in orthopedic surgery, some clinicians advocate that it should be considered as a part of multimodal analgesia and not as a single pain control modality because it does not block the entire operative limb.12-17
Since there is a need for the development of an evidence-based approach to reliable, comprehensive, individualized analgesic plans for specific surgical procedure, in the present study we compared the continuous intravenous morphine, administered via a continuous IV infusion pump with femoral block regarding efficacy of pain management and patients’ satisfaction, so that the best post-operative pain management for ACL reconstruction can be decided.
METHODOLOGY
The present study was designed as a randomized clinical trial and was conducted on 54 ASA I&II patients from July 2012 to March 2014. The study protocol was approved by local ethics committee of Hamedan University of Medical Sciences and registered in Iran Registration of Clinical Trials (IRCT) database under the ID: IRCT201402279014N27.
Inclusion criteria included Patients aged 12-70 years, admitted to BESAT Medical Center for ACL open reconstruction.
Exclusion criteria was; patients unwilling to participate in the study; history of cardiovascular, renal or hepatic disease; pre-existing allergies to local anesthetics; history of drug abuse; Bilateral organ surgery, previous ileoinguinal surgery (femoral vascular grafts, renal transplantation etc), large ilioinguinal tumor or lymph node; femoral nerve neuropathy; local or peritoneal infections, perioperative complications and technical problems.
Sample size for each group was determined from the formula:
An alpha level < 0.05 was considered to be statistically significant. The power value was determined to be 80%, with an assumed dropout rate of 20%. A former study found a standardized difference of 0.817-18), thus, sample size of approximately 27 patients is obtained.
Accordingly 54 patients recruited in the study and were divided in 2 equal groups; Group-A (continuous IV infusion pump) and Group-B (femoral nerve block), using randomized blocks. Allocation proceeded by randomly selecting one of the blocks of participants and assigning the next block to study groups according to the specified sequence.
The protocol, possible benefits and complications were explained to each patient, and they all (for children under 18, a legal guardian) signed their informed consent forms prior to operation.
Premedication with 2 mg midazolam and 0.3 mcg/kg fentanyl was done according to the standard protocol and anesthesia induction was performed using 2 mg/kg propofol. In addition 0.5 mg/kg atracurium was administrated for muscle relaxation and ease of intubation. Three minutes later, the patient was intubated with a cuffed tracheal tube and anesthesia was maintained using 1.2% Isoflurane in 50% O2 and 50% N2O. During the surgery, fluid therapy was given according to standard protocols.
Femoral block for coded subjects was performed at the end of the surgery right before exit. For patients in the other group, continuous IV infusion catheter was inserted after extubation and the patient transferred to recovery room.
Femoral nerve block technique
After recovery from muscle relaxation, the patient was placed in supine position and anatomic references (upper anterior iliac crest, pubic tubercle, inguinal ligament, and femoral artery) were located. Inguinal ligament was localized between upper anterior iliac crest and pubic tubercle. Femoral artery was touched and localized under the ligament. Then, under the guide of ultrasound, the needle was advanced at a 60 degree angle in a posterior and cephalad direction. Stimulation of quadriceps muscle of thigh is expressed with patellar twitches, medial and lateral muscle twitches were also seen if the needle was too much medial; or distal and lateral to center of the nerve. 25mg bupivacaine 0.25% equal to 10 ml was injected. Femoral block was confirmed by ultrasound if the nerve was totally surrounded by anesthetic agent.
Continuous IV infusion pump insertion technique
Continuous infusion pump with 100 ml of volume was used. 0.01 mg/kg morphine was diluted in 0.9% normal saline, up to 100 ml and was administered at a constant rate of 4 ml/h.
Pain evaluation method
Pain intensity was assessed and recorded in recovery service and right after complete consciousness, and then every 4 hours by trained nurses of the department, using visual analogue scale (VAS), in which 0 represented no pain, while 10 indicated worst possible pain.
After being awake and achieving complete consciousness, patients’ satisfaction from post-operative analgesia was questioned and recorded every 12 hours, using five-level Likert item. A Likert scale is the most widely used approach to scaling responses in survey research. When responding to a Likert questionnaire item, respondents specify their level of agreement or disagreement on a symmetric agree-disagree scale for a series of statements. The format of this scale is as follow: strongly satisfied, satisfied, neutral, dissatisfied, and strongly dissatisfied.
The patients were monitored for at least 8 hours. Vital signs were checked every 15 minutes in the first hour, every 30 minutes in the next 3 hours and once an hour afterwards. Nursing staff was asked to discontinue the infusion in case of apnea or stupor. No sedative was given except that of the protocol. In case of patient’s insistence for any other pain killers, the patient was removed from the study and parenteral analgesics were administered.
Statistical Analysis
Gathered data transferred to statistical software SPSS V.16. Quantitative variables were reported using central parameters as mean and standard deviation. For a qualitative comparison between the two groups, chi-square analysis was used. Independent t-test and repeated measures of ANOVA were used to compare the means. In case of not following the normal average of data, non-parametric analysis was used.
RESULTS
In the current clinical trial, all 54 subjects completed the study with mean age of 36.55 ± 8.1 years, ranging from 12 to 70 years. Mean age of group A (continuous IV infusion pump) was 44.35±7.8 years and in group B (femoral block) it was determined as 37.66 ± 13.8 years. 42(77.8%) patients were males; 21 in each group. No statistical significance was noted in age and gender differences in two groups.
Mean VAS of pain intensity and patient satisfaction in two groups was analyzed. Scores showed statistical difference only at 20 and 24 hours after surgery in which, Pain intensity was lower in Group-A (continuous IV infusion pump) than in group B (femoral block)(Table 1).
Mean patient satisfaction was recorded right after the surgery, and 12 & 24 hours afterwards. No statistical difference was noted (Table 2).
Any post-operative complication was noted and recorded in each group. 10 patients in Group-A (continuous IV infusion pump) and 4 patients in Group-B (femoral nerve block) developed complications such as nausea, vertigo, weakness and dry mouth which were treated accordingly (Figure 1). No incidence of apnea or stupor was reported.
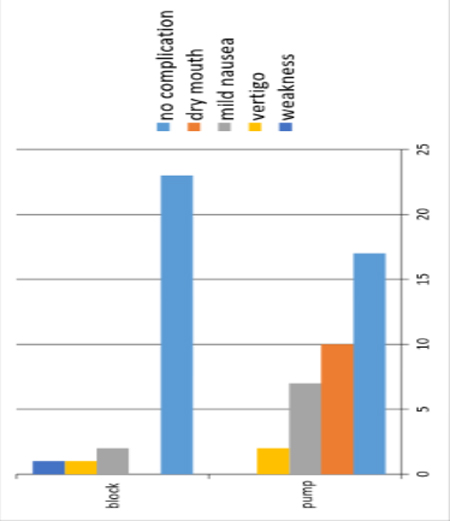
Table 1: VAS scores for pain at different times
|
▼Time sections (Hrs) |
VAS scores |
P-value |
|
|
Group-A (continuous IV infusion pump) N=27 |
Group-B (Femoral block) N=27 |
||
|
0 |
2.681 |
2.819 |
0.705 |
|
4 |
2.983 |
2.517 |
0.24 |
|
8 |
2.928 |
2.52 |
0.36 |
|
12 |
2.678 |
2.82 |
0.70 |
|
16 |
2.413 |
3.08 |
0.08 |
|
20 |
2.3 |
3 |
0.02 |
|
24 |
2.291 |
3.20 |
0.02 |
Table 2: Patient satisfaction scores at different times
|
▼Time sections (Hour) |
Satisfaction scores |
P-value |
|
|
Group-A (continuous IV infusion pump) N=27 |
Group-B (Femoral block) N=27 |
||
|
0 |
2.339 |
2.76 |
0.95 |
|
12 |
2.63 |
2.86 |
0.56 |
|
24 |
2.65 |
2.64 |
0.6 |
DISCUSSION
The method of choice to treat postoperative pain is a multimodal analgesic approach combining different drugs and techniques. Orthopedic operations of the extremities are amongst the most painful procedures, with frequent post operative pain, which requires effective analgesic techniques in the company of minimal side effects. Understanding the course of postoperative pain would be of utmost importance for future quality improvement of postoperative pain therapy.4
In point of fact, the main protocol for ACL surgery is to move the operated knee as soon as possible, in order to reduce the postoperative complications and hospital costs and to accelerate the time of discharge. The current study focused on the first 24 hours after surgery for ACL reconstruction, during which many patients happen to experience highest levels of pain. This study was designed to compare the analgesic effects of single-injection femoral block and continuous IV infusion pump on postoperative pain in the early postoperative period (first 24 hours) after anterior cruciate ligament reconstruction surgery in patients admitted to BESAT medical center during June 2012 until March 2013. Noteworthy in this study is to develop an appropriate post-operative analgesia for patients. Reducing post operative patients’ need for opiods is of great importance in goal establishment of trials, and our study revealed a desirable analgesia in 24 hours after anterior cruciate ligament reconstruction surgery, although in femoral nerve block technique, VAS score and nerve block complications were lower, while patient satisfaction was higher especially during the first 8 hours after surgery. Therefore this method of analgesia can be recommended for lower extremities surgeries.
Findings from our study showed no statistical significant difference in demographic data between two groups, which is consistent with the study conducted by Imani, et al in 2011.19
Studies had showed that peripheral nerve block in both upper and lower extremities increase duration of post operative analgesia and patient satisfaction. Although rare cases of neural complications may occur.20 In the present study, mean pain score of two groups (femoral nerve block and continuous IV infusion pump) were compared which revealed significant difference only at 20 and 24 hours after surgery, and was lower in continuous IV infusion pump group. Mean pain score of group B (femoral nerve block) was lower in 4 and 8 hours of post operation, although the difference was not statistically significant. These findings are consistent with multiple researches which are previously conducted.
As cases in point, Hunt et al in 2009 evaluate the addition of a single-injection sciatic nerve block to a femoral nerve block for analgesia after total knee arthroplasty. Lower visual analog pain scale scores were noted in both femoral nerve blockade and FSNB groups through 48 hours while Morphine use was significantly lower in the FSNB group. They concluded that Femoral and sciatic nerve block can be placed quickly and consistently in the operating room with improved postoperative pain relief and reduced narcotic consumption.21
Another study conducted by Mulroy et al, evaluated the efficacy of femoral nerve block in reducing postoperative pain and duration of analgesia compared with standard analgesia following outpatient anterior cruciate ligament repair. Femoral nerve block with bupivacaine contributes significantly to postoperative analgesia in the immediate postoperative period and the first 24 hours after surgery.22
Patient satisfaction in two groups was assessed and compared right after the surgery, and 12 & 24 hours afterwards. Results showed higher degree of patient’s satisfaction in femoral nerve block group rather than continuous IV infusion pump group, as a whole; femoral nerve block had not reduced patients’ satisfaction significantly. These findings are consistent with other accomplished studies.
For case in point, is a prospective multicenter study: Mullaji et al evaluated the efficacy of a local anesthetic by comparing pain scores, on the day of surgery, first postoperative day, day of discharge, and 2 and 4 weeks after surgery patients undergoing simultaneous bilateral computer-assisted total knee arthroplasty who were randomized to receive the injection in the right or left knee. In comparison to the noninfiltrated side, the infiltrated knee showed significantly lower pain scores. They showed that this simple and inexpensive technique can significantly reduce pain after total knee arthroplasty.23
In another study, authors prospectively evaluated the effect of femoral nerve block on a numeric rating scale (NRS) of pain intensity. They showed that femoral nerve block catheters dependably keep NRS scores below the moderate-to-severe pain threshold for the first 4 days after anterior cruciate ligament reconstruction.24
This mechanism is confirmed by several other studies. Williams et al compared continuous epidural infusion, continuous femoral block, or intravenous patient-controlled morphine. Pain was assessed at rest and during continuous passive motion using a visual analog scale. The continuous epidural infusion and continuous femoral block groups showed significantly lower visual analog scale scores compared to patient-controlled pump group while side effects encounter was more common in the continuous epidural infusion group.25 In the present study, Post operative complications was also evaluated. Findings revealed less frequency of dry mouth, nausea, vertigo and weakness in femoral nerve block group in comparison with continuous IV infusion pump which is consistent to the mentioned study.
LIMITATIONS
A limitation of the current study is that in randomization of the blocks, the allocation of participants may be predictable and result in selection bias, when the study groups are unmasked. That is, the treatment assignment that has so far occurred least often in the block likely will be the next chosen.
CONCLUSION
Conclusively, post-operative complications (especially nausea) in femoral nerve block are lower, but the pain scores in the continuous intravenous infusion group at 20 and 24 hours after surgery were significantly lower than femoral nerve block group, but analgesia achieved by femoral nerve block is comparable with continuous IV infusion pump before 20th postoperative hour. It is recommended to design and conduct further blinded clinical trials particularly with short and ultra short acting analgesic infusions.
Conflict of interests: The authors have no conflicts of interest to disclose.
Funding: None
REFERENCES
1-Robert H. Miller Knee Injuries. S.Terry Canale. Campbell’s Operative Orthopaedics. Philadelphia. Mosby. 2003. Vol.3, 10th ed. 2166-2323.
2-Badizadeh K. How long athletes remain athletes after anterior cruciate ligament reconstruction. Iran J Orthop Surg 2004;2-3:61-64.
3-Svensson M, Sernert N, Ejerhed L, Karasson J, Kartas JT. A prospective comparison of bone-patellar tendon-bone and hamstring grafts for anterior cruciate ligament reconstruction in female patients. Knee Surg Sports Traumatol Arthrosc 2006;14:278-86. [PubMed]
4- Gramke HF, de Rijke JM, van Kleef M, Raps F, Kessels AG, Peters ML, et al. The prevalence of postoperative pain in a cross–sectional group of patients after day case surgery in a university hospital. Clin J Pain 2007;23:543-48. [PubMed]
5- Carr DB, Goudas LC. Acute pain. Lancet 1999;353:2051. [PubMed]
6. Breivik H. Postoperative pain management: why is it difficult to show that it improves outcome? Eur J Anaesthesiol 1998;15:748. [PubMed]
7. Practice guidelines for acute pain management in the perioper-ative setting: a report by the American Society of Anesthesiol-ogists Task Force on Pain Management, Acute Pain Section.
Anesthesiology 1995; 82:1071. [PubMed]
8. Twersky R, Fishman D, Homel P. What happens after dis-charge? Return hospital visits after ambulatory surgery. Anesth Analg 1997;84:319. [PubMed]
9- Sechzer PH. Studies in pain with the analgesic-demand system. Anesth Analg 1971; 50:1–10. [PubMed]
10- Miller R. Millers anesthesia. In: Malhotra V. Chronic pain and preoperative pain. 6th ed. Philadelphia: Elsevier Churchill Livingston; 2005. P: 2175-343
11- Smeltzer SC, Bare BG, Hinkle JL, Cheever KH. Brunner and suddarth’s textbook of medical surgical nursing: in one volume (brunner & suddarth’s textbook of medical-surgical nursing). Third ed. New York: Lippincott Williams & Wilkins; 2009.
12- de Lima e Souza R,Henrique Correa C, Delage Henriques M, Barbosa de Oliveira C, Afonso NunesT, Santiago Gomez R. Single-injection femoral nerve block with 0.25% ropivacaine or 0.25% bupivacaine for postoperative analgesia after total knee replacement or anterior cruciate ligament reconstruction. J of Clin Anesth 2008;20:521–27. [PubMed]
13. Momeni M, Crucitti M, De Kock M. Patientcontrolled analgesia in the management of oostoperative pain. Drugs; 2006;66:2322-35. [PubMed]
14. Miller MD, Cole BJ. Arthroscopy of the lower extremity. In: Text book of arthroscopy, 1st ed, Philadelphia: Lippincott, Williams & Wilkins; 2004. Chapter 48, P 2855-2886.
15-Rubenovitch J, d’Athis F. Effects of perioperative analgesic technique on the surgical outcome and duration of rehabilitation after major knee surgery. Anesthesiology; 1999. 91: 8-15. [PubMed] [Free Full Text]
16-Marcia K. Anderson. Knee Conditions. Eric Johnson. Sports Injury Managment. Philadelphia. Lippincott Williams & Wilkins.2000, 2th ed.431-482.
17-Hunt K, H. Bourne M, Mariani M. Single-Injection Femoral and Sciatic Nerve Blocks for Pain Control After Total Knee Arthroplasty. J Arthroplasty 2009;24:553-57. [PubMed]
18- Williams, Brian A. M.D., M.B.A.; Kentor, Michael L. Reconstruction with 2-Day Continuous Femoral Nerve Block.The journal of American.2006,104:515-327. [PubMed] [Free Full Text]
19- Farnad imani , Ghodrat akhavan-akbari , Ali Mohammadian-erdi , Poupak Rahimzadeh. An evaluation of the effects of adding oral pregabaline to morphine sulfate in patients receiving Intravenous PCA after orthopedic surgery. J Anesth & Pain 2011;4:72-78.
20- Rubenovitch J, d’Athis F. Effects of perioperative analgesic technique on the surgical outcome and duration of rehabilitation after major knee surgery. Anesthesiology; 1999. 91: 8-15. [PubMed] [Free Full Text]
21. Hunt JK, H. Bourne M, Mariani M. Single-Injection Femoral and Sciatic Nerve Blocks for Pain Control after Total Knee Arthroplasty. J Arthroplasty 2009;24:553-57. [PubMed]
22. Mulroy, Michael F. M.D.; Larkin, Kathleen. Femoral Nerve Block With 0.25% or 0.5% Bupivacaine Improves Postoperative Analgesia Following Outpatient Arthroscopic Anterior Cruciate Ligament Repair. Anesthesia and pain, 2001:26:24-29. [PubMed]
23. Mullaji A, Kanna R, Shetty GM, Chavda V, Singh DP. Efficacy of periarticular injection of bupivacaine, fentanyl, and methylprednisolone in total knee arthroplasty:a prospective, randomized trial. J Arthroplasty 2010; 25: 851-7. [PubMed]
24. Matava MJ, Prickett WD, Khodamoradi S, Abe S, Garbutt J. Femoral nerve blockade as a preemptive anesthetic in patients undergoing anterior cruciate ligament reconstruction: A prospective, randomized, double-blinded, placebo-controlled study. Am J Sports Med 2009; 37:78-86. [PubMed]
25.Capdevila X, Barthelet Y, Biboulet P, Ryckwaert Y, Rubenovitch J, d’Athis F. Effects of perioperative analgesic technique on the surgical outcome and duration of rehabilitation after major knee surgery. Anesthesiology 1999; 91:8-15. [PubMed] [Free Full Text]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube