
Jestin Elias Ninan1, Ranjan RV2, T. R. Ramachandran3, Sagiev Koshy George4
1Senior resident; 2Associate Professor; 3Professor; 4Professor & Head,
Department of Anesthesiology, Pondicherry Institute of Medical Sciences (PIMS), Pondicherry (India)
Correspondence: Dr. Jestin Elias Ninan, Door No. 18, Jolly Bhavan, Cholan Nagar, O. K. Palayam, 100 Feet Road, Mudaliarpet, Pondicherry 605004, (India)
ABSTRACT
Objective: We aimed to compare C-MAC videolaryngoscope (VLC) with Macintosh laryngoscope with regard to the laryngoscopic view, the need for external laryngeal manipulation, requirement of airway adjuncts like stylet, time required to complete the tracheal intubation and the hemodynamic changes in Mallampati class 2 and 3 patients.
Methodology: Sixty patients who were admitted for elective surgery requiring general anesthesia with endotracheal intubation were randomly allocated to proceed with endotracheal intubation using the conventional Macintosh VLC (Group A) or the C-MAC VLC (Group B). Following a standardised general anesthetic protocol, time for intubation, laryngoscopic view, need for external manipulation, and hemodynamic parameters during and after intubation were registered during study period.
Results: It was observed that C-MAC VLC improves the laryngoscopic view in predicted difficult airway setting, and thus reduces the need for external laryngeal manipulation and the use of stylet. However, the hemodynamic stress response was significant with C-MAC VLC than Macintosh laryngoscopy. There was significant reduction in time taken for intubation with conventional Macintosh laryngoscope when compared with C-MAC® VLC. The median total intubation time for the Macintosh and C-MAC® laryngoscopes was 23.8 sec and 35.33 sec respectively (p = 0.000).
Conclusion: C-MAC® videolaryngoscope improves laryngoscopic view in difficult airway settings compared to the conventional Macintosh laryngoscope, but at the cost of prolonged time taken for intubation and increased hemodynamic stress response. Large scale studies may be required to determine the ultimate success of intubation with this new tool.
Key words: Videolaryngoscope; Laryngoscopy; Intubation; Stress response; Hemodynamic; Airway Management/instrumentation; Glottis; Intubation, Intratracheal/instrumentation; Laryngoscopy/instrumentation
Citation: Ninan JE, Ranjan RV, Ramachandran TR, George SK. C-MAC videolaryngoscope improves the laryngoscopic view in Mallampati class 2 and 3 patients. Anaesth Pain & Intensive Care 2016;20(3):261-265
Received: 13 April 2016; Reviewed: 13 April 2016 & 24 June 2016; Corrected: 28 Augusr 2016; Accepted; 02 September 2016
INTRODUCTION
Endotracheal intubation has become a routine part of delivering a general anesthetic. Laryngoscopy is usually performed to facilitate intubation as a part of general anesthesia. The Macintosh laryngoscope is the most commonly used device to directly visualise the structures of the larynx and thus facilitate endotracheal intubation. However, its usefulness in many cases of difficult airway proves to be limited. Few studies have suggested that the use of videolaryngoscope (VLS) could improve the view of larynx and eases intubation in difficult airway situations.1-5
The C-MAC® VLS (Karl Storz Tuttlingen, Germany) blade is designed similar to the Macintosh, with an added advantage of a video camera at the distal end of the blade. It can be used similar to Macintosh for direct laryngoscopy and also for indirect laryngoscopy when the operator views the larynx on the video screen. Indirect laryngoscopic view on the video screen enables the assistant to see the effect of any external laryngeal manipulation on the laryngoscopic view in situation of difficult intubation. However, the stress response due to laryngoscopy and tracheal intubation have a profound influence on the circulatory parameters and the intracranial pressure.6,7
The aim of this study was to evaluate the glottic view, the requirement of optimization maneuver, the need for airway adjunct, the time taken for intubation and the hemodynamic response between Macintosh laryngoscope and C-MAC® VLS during endotracheal intubation in Mallampati class 2 and 3 patients.
METHODOLOGY
After approval from local Research Ethics Committee, sixety patients with Mallampati class 3 & 3 belonging to ASA grade 1 & 2, undergoing elective surgery under general anesthesia withendotracheal intubation in The Pondicherry Institute of Medical Sciences (PIMS), Pondicherry (India) between 2015-2016, were enrolled. During the preoperative assessment, the participants were given a patient information sheet and time to read the material and any queries regarding the study were answered. The patients with uncontrolled hypertension, children below eighteen years of age, any patient with recent respiratory tract infection, morbid obesity, pregnant or edentulous patients were excluded. Preoperative airway assessment included modified Mallampati score8, mouth opening and cervical spine movement. Patients were premedicated with standard drugs. On the day of surgery patients were shifted to OR complex and electrocardiogram, non-invasive BP and pulse oximeter were connected. Intravenous access was established with 18 G cannula and the slow infusion of crystalloids was started. All patients were preoxygenated for 5 min, premedicated with midazolam 0.03 mg/kg, glycopyrrolate 5-10 µg/kg, fentanyl 1-2 µg/kg; induced with thiopentone 4-6 mg/kg and vecuronium 0.1 mg/kg. Anesthesia was maintained with isoflurane in oxygen and nitrous oxide.
The patients were positioned supine with their head and neck at the optimum position for intubation. Prior to induction of anesthesia, one of the two laryngoscopes, either C-MAC® or Macintosh, was chosen randomly by computer generated random numbers. The same anesthetist performed all intubations in the study group. C-MAC® size 4 and Macintosh size 4 blades were chosen for all patients in the study. During induction and throughout the procedure, oxygen saturation, end tidal CO2, non-invasive blood pressure and heart rate were monitored. The data collected included Cormack-Lehane classification of laryngoscopic view9, the requirement of optimization maneuver, the need for airway adjunct (if Cormack-Lehane class was more than 2b), the time taken for intubation and the hemodynamic response between Macintosh laryngoscope and C-MAC® VLS during endotracheal intubation in the operating room. The intubation time was defined as the interval from insertion of the laryngoscope blade into the mouth to inflation of the tracheal tube cuff. Following tracheal intubation, correct placement of tracheal tube was confirmed by auscultation and capnography. If the time to successful intubation exceeded 120 sec, the attempt was considered a failure and qualified for exclusion from the study. The airway was then managed according to the ASA difficult airway algorithm and guidelines.
The results were expressed in means and proportions. The differences between the two groups were compared using Chi-square test, t-test and ANOVA. P value < 0.05 was considered as statistically significant.
RESULTS
The demographic variables were evenly distributed between the two groups (Table 1). The intubation time, laryngoscopic view and additional maneuvers required, stylet used are presented (Table 2).
Table 1: Patient demographics
| Demographic Data | Group A
(Macintosh) |
Group B
(C-MAC) |
| Mean age (years) | 38.03 | 41.03 |
| Sex (male:female) | 22:8 | 20:10 |
| Mean BMI (kg/m2) | 25.3 | 25.8 |
| Mallampati 2:3 | 20:10 | 18:12 |
Table 2: Comparative intubation data
| Intubation data | Group A
(Macintosh) |
Group B
(C-MAC) |
P value |
| Intubation Time (sec) | 23.8 | 35.33 | 0.000 |
| Laryngoscopic view
(Class 1/2a/2b/3a/3b/4) |
0/20/9/1/0/0 | 0/21/9/0/0/0 | 0.599 |
| External Laryngeal Manipulation (n) | 10 | 9 | 0.681 |
| Need for stylet (n) | 6 | 2 | 0.254 |
| Success rate (%) | 100% | 100% | NS |
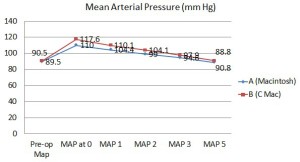
The hemodynamic responses to intubation between both the groups at preop, 0, 1, 2, 3 and 5 mins are presented in Table 3. The median intubation time for the C-MAC® and Macintosh was 35.33 sec and 23.8 sec respectively (p = 0.000). A difference of more than 5 sec to intubate between the groups was considered clinically significant. There were no significant differences in laryngoscopic view or additional maneuvers required. Indirect laryngoscopy with C-MAC® revealed grade 1/2a/2b/3a/3b/4 (Cormack-Lehane) views in 0/21/9/0/0/0 patients respectively, whereas the same grades were revealed in 0/20/9/1/0/0 patients with direct laryngoscopy with Macintosh respectively. The Mallampati scores were evenly distributed between the two groups. In the C-MAC group, 9 patients required external laryngeal manipulation (BURP maneuver), 2 patients required the use of stylet to facilitate tracheal intubation. In the Macitnosh group 10 patients required BURP, 6 patients required the use of stylet to facilitate tracheal intubation. That is, out of 9 patients in C-MAC group and 10 patients in Macintosh group, who required BURP, 2 in C-MAC Group (p value 0.0827) and 6 in Macintosh Group (p value 0.00035) required stylet for intubation. This need for stylet was statistically significant in Macintosh group. The overall success rate of tracheal intubation was 100% in both groups. The hemodynamic stress response to laryngoscopy (Table 3, Figure 1 & 2) was profound in C-MAC group at 0, 1 and 2 min intervals, possibly due to prolonged duration of laryngoscopy. An increase in heart rate of more than 20% and mean arterial pressure of more than 10 mmHg between the groups was considered clinically significant.
Table 3: Comparison of heart rate (HR) and mean arterial pressure (MAP)
| Parameter | Group A
N = 30 |
Group B
N = 30 |
p-value |
| Mean ± SD | Mean ± SD | ||
| Preop HR | 77.60 ± 4.64 | 78.07 ± 4.01 | .68 |
| Preop MAP | 89.50 ± 2.86 | 90.50 ± 3.60 | .24 |
| HR-Zero | 110.07 ± 3.93 | 126.60 ± 5.08 | .03 |
| MAP-Zero | 110.03 ± 3.19 | 117.60 ± 4.12 | .02 |
| HR-1 | 101.63 ± 3.49 | 118.00 ± 5.09 | .02 |
| MAP-1 | 104.47 ± 2.68 | 110.17 ± 4.17 | .01 |
| HR-2 | 95.80 ± 3.41 | 110.97 ± 3.24 | .03 |
| MAP-2 | 99.07 ± 2.95 | 104.13 ± 3.79 | .02 |
| HR-3 | 90.03 ± 3.34 | 90.43 ± 1.99 | .58 |
| MAP-3 | 94.67 ± 1.81 | 97.90 ± 1.77 | .24 |
| HR-5 | 76.07 ± 3.28 | 80.50 ± 3.43 | .29 |
| MAP-5 | 88.80 ± 1.45 | 90.83 ± 1.80 | .18 |
Figure 1: Comparison of mean heart rate between the groups
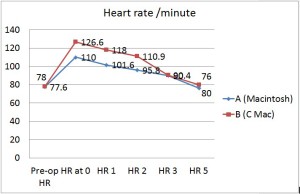
Figure 2: Comparison of mean arterial pressure between the groups
DISCUSSION
Our results showed a small but statistically significant difference in the mean intubation time between C-MAC® and Macintosh laryngoscopes. The C-MAC® and Macintosh blades are identical in design and the skills acquired using one device should be transferable to the other device when C-MAC® is used as direct laryngoscope. In anticipated difficult airway, C-MAC® VLS has better performance in terms of shorter intubation time, higher success rate and less number of optimising maneuvers.10,11 Although VLS provides a good view of the larynx, it may not guarantee an easy tracheal intubation12,13 and may prolong the time required for successful intubation. Therefore, we compared the performance of C-MAC® with Macintosh in patients with a predicted difficult airway with respect to the laryngoscopic view, need for optimization maneuvers, requirement of stylet, time taken for intubation and the hemodynamic changes at 0, 1, 2, 3 and 5 min intervals. Recently introduced C-MAC® D-blade (difficult airway blade) has been shown to improve the success rate of endotracheal intubation in patients with anticipated difficult airway.14
There was no significant difference between the two devices in terms of the laryngoscopy views and the optimization maneuvers required to facilitate intubation. This may be due to the fact that the blades are of similar design and the two groups were of similar demographics. All patients with Cormack-Lehane grade 2b/3a views were provided with external laryngeal manipulation (ELM). 9 patients in C-MAC group and 10 patients in Macintosh group were provided with ELM. On providing ELM, the laryngoscopic view of some patients progressed to lower grade. This progress was more significant in C-MAC Group (7 out of 9 patients progresssed to 2a view) than Macintosh group (4 out of 10 patients progressed to better view). On statistical analysis, this difference between the groups was not significant. However, this difference was clinically significant. Airway adjunct (stylet) was used in patients who continued to be 2b views after ELM. Stylet was, therefore, used in 6 patients in Macintosh group and 2 patients in C-MAC® videolaryngoscopic view, suggesting that stylet use was less with videolaryngoscopy than direct laryngoscopy. This need for stylet was statistically significant in Macintosh group (p value 0.00035). In an attempt to compare C-MAC® videolaryngoscopy and Macintosh laryngoscopy, the present study showed that the time taken by C-MAC® videolaryngoscopy (35.33 sec) was significantly higher compared to Macintosh direct laryngoscopy (23.8 sec). This difference in groups was statistically significant (p < 0.001), and clinically significant [difference of >5 sec]. In our study, on intergroup comparison, the C-MAC group showed a statistically significant rise in heart rate and MAP at 0, 1, 2 min on comparing with Macintosh group. An increase in heart rate of more than 20%, mean arterial pressure of more than 10 mmHg between the groups was considered clinically significant. There was a decreasing trend observed in all parameters after the initial rise. The prolonged duration of laryngoscopy may be the reason for profound hemodynamic stress response observed in the C-MAC group. Our study was comparable with others like Abdullah et al15 who compared C-MAC, Glidescope, and Macintosh laryngoscopes in manikin and found that VLSs offer better laryngoscopic view and reduced intubation time. VLSs offer advantage not only in novice hand but also help experiencd anesthesiologists during difficult intubation scenarios. Shahir M et al16 compared C-MAC® with macintosh direct laryngoscope during cervical spine immobilization and concluded that VLSs reduces intubation time and increases first time success rates.
Patients from both groups had no significant complications. Oxygenation was well maintained despite the variation in intubation times due to the process of preoxygenation that was conducted in our study. There are a few limitations that can be identified in our study. Firstly, it was not possible to blind the investigator about the device being used. This study was done on ASA 1 and 2, non hypertensive patients posted for elective surgeries. Results may vary in emergencies or in hypertensive patients or if the patient is having other difficult airway predictors.
CONCLUSION
We conclude that C-MAC® videolaryngoscope improves the laryngoscopic view in Mallampati class 2 and 3 airway views and lessens the need for external laryngeal manipulation and the stylet use. The time taken for intubation is longer with the C-MAC® videolaryngoscope than the conventional Macitnosh laryngoscope. The C-MAC® videolaryngoscope does improve laryngoscopic view in difficult airway settings, however, larger studies are required to determine the ultimate success of intubation.
Conflict of interest: None declared by the authors
Author contribution: JEN / RRV – Concept, study conduction & editing; RTR / SKG – Editing
REFERENCES
- Kaplan MB, Hagberg CA, Ward DS, Brambrink A, Chhibber AK, Heidegger T, et al. Comparison of direct and video assisted views of the larynx during routine intubation. J Clin Anesth. 2006;18(5):357-62. [PubMed]
- Enomoto Y, Asai T, Arai T, Kamishima K, Okuda Y. Pentax-AWS, a new videolaryngoscope is more effective than the Macintosh laryngoscope for tracheal intubation in patients with restricted neck movements: a randomised comparative study. Br J Anaesth. 2008 Apr;100(4):544-8. [PubMed] [Free full text]
- Cooper RM, Pacey JA, Bishop MY, McCluskey SA. Early clinical experience with a new videolaryngoscope(Glidescope) in 728 patients. Can J Anaesth. 2005 Feb;52(2):191-8. [PubMed]
- Malik MA, Subramaniam R, Maharaj CH, Harte BH, Laffey JG. Randomised controlled trial of the Pentax AWS, Glidescope, and Macintosh laryngoscope in predicted difficult intubation. Br J Anaesth. 2009 Nov;103(5):761-8.[PubMed] [Free full text]
- Teoh WH, Saxena S, Shah MK, Sia AT. Comparison of three videolaryngoscopes: Pentax Airway Scope , C-MAC, Glidescope vs the Macintosh laryngoscope for tracheal intubation. Anaesthesia. 2010 Nov;65(11):1126-32. doi: 10.1111/j.1365-2044.2010.06513. [PubMed]
- Miller RD, Pardo M. Airway management of Anesthesia. Basics of anesthesia 2005;6:1636
- Kaur S, Gupta A, Ranjana, Rita. Intubating conditions and stress response to laryngoscopy: Comparison between Macintosh and levering (McCoy’s Type) Laryngoscope. J Anaesthesiol Clin Pharmacol. 2009;25(3):333-336.
- Mallampati SR, Gatt SP, Gugino LD, Desai SP, Waraksa B, Freiberger D, et al. Aclinical sign to predict difficult tracheal intubation: a prospective study. Can Anaesth Soc J. 1985 Jul;32(4):429-434. [PubMed]
- Cormack RS, Lehane J .Difficult tracheal intubation in obstetrics. Anaesthesia 1984 Nov;39(11):1105-1111. [PubMed]
- Cavus E, Kieckhaefer J, Doerges V, Moeller T, Thee C, Wagner K. The C-MAC videolaryngoscope: first experiences with a new device for videolaryngoscopy guided intubation. Anesth Analg. 2010 Feb;110(2):473-477. [PubMed]
- Jungbauer A, Schumann M, Bunkhorst V, Börgers A, Groeben H.Expected difficult tracheal intubation: a prospective comparison of direct laryngoscopy and video laryngoscopy in 200 patients. Br J Anaesth. 2009 Apr;10(4)2:546-555. [PubMed] [Free full text]
- Frerk CM, Lee G . Laryngoscopy: time to change our view. Anaesthesia. 2009 Apr;64(4):351-354. doi: 10.1111/j.1365-2044.2008.05855.x. [PubMed]
- Van Zundert A, Maassen R, Lee R. Willems R, Timmerman M, Siemonsma M, et al. A Macintosh laryngoscope blade for videp laryngoscopy reduces stylet use in patients with norma lairways. Anesth Analg. 2009 Sep;109(3):825-831. doi: 10.1213/ane.0b013e3181ae39db [PubMed]
- Cavus E, Neumann T, Doerges V, Moeller T, Scharf E, Wagner K, et al. First clinical evaluation of the C-MAC D-blade videolaryngoscope during routine and difficult intubation. Anesth Analg. 2011 Feb;112(2):382-385. doi: 10.1213/ANE.0b013e31820553fb [PubMed]
- Kaki AM, AlMarakbi WA, Fawzi HM, Boker AM. Use of Airtraq, C-Mac, and Glidescope laryngoscope is better than Macintosh in novice medical students’ hands: A manikin study. 2011;5(4):376-381. [Free full text]
- Shahir h, M akbar, Joanna SM.Comparison between C-mac® video-laryngoscope and macintosh direct laryngoscope during Cervical spine immobilization. M.E.J. Anesth. 2015;23(1):43-50. [Free full text]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube