
Naseem Ahmed1, Kiran Naseem2, Muhammad Rafiq, PhD3
1Department of Anesthesiology, Combined Military Hospital, Rawalpindi (Pakistan)
2MS Economics, Institute of Business Administration (IBA), KU Circular Rd, University of Karachi, Karachi, 75270 (Pakistan)
3C-II, Institute of Clinical Psychology, University of Management Technology C-II, Johar Town, Lahore-54077 (Pakistan)
Correspondence:
Brig Naseem Ahmed,
Department of Anesthesiology,
CMH Rawalpindi (Pakistan)
Mobile: +92 336 2800074
E-mail: naseemahmed937@gmail.com
ABSTRACT
Objective: Tracheal stenosis is usually iatrogenic, a result of an accident or due to tracheal tumors. Anesthesia for tracheal resection and reconstruction is a challenging job and requires expertise. The crux of anesthetic management is securing the airway early and maintenance of ventilation and oxygenation during resection and reconstruction. This study is aimed to share the anesthetic management and outcome of 21 cases of tracheal resection and reconstruction surgery for tracheal stenosis.
Methodology: This prospective, descriptive study was carried out at PNS Shifa Hospital Karachi and Combined Military Hospital Rawalpindi between October 2014 and July 2018. All 21 patients undergoing tracheal resection and reconstruction surgery for tracheal stenosis at these centers were enrolled. Informed consent was obtained from all patients and institutional ethics committee approval was secured. The site of tracheal stenosis, type of anesthesia used, ventilation and oxygenation before and during resection and anastomosis of trachea and the type of surgery and the outcome was noted. The data were collected in MS Excel sheet and simple statistical analysis done to present the results.
Results: Out of 21 patients, 9 (43%) were males and 12 (57%) were females, between 6 to 66 years of age of ASA II-IV. Post intubation stenosis was the leading cause of stenosis followed by tumor, trauma and corrosive ingestion. Fourteen patients had high cervical / subglottic stenosis and were operated by high anterior cervical collar incision, while five had lower tracheal lesions, and 2 had carinal lesion and were operated by right thoracotomy. Seven patients were anesthetized through tracheostomy tube, one by fiberoptic intubation, and the rest with 5-7 mm ETT with or without muscle relaxant. One patient developed cardiac arrest during surgery, but was revived successfully. Four (19%) out of 21 had to be put on ventilator postoperatively while remaining 17 (89%) were extubated on operating table. Two patients on ventilator were weaned of successfully. Outcome was excellent in 19 (90%) cases while in 2 (10%) patients, operation was unsuccessful and they landed up with permanent tracheostomy.
Conclusion: The study highlights the importance of prevention of post-intubation tracheal stenosis with strict vigilance and high quality professional nursing care. Thorough preoperative assessment and preparation, intra operative management, a backup plan and close communication between the surgeon and anesthesiologist are necessary for successful outcome. Most of these patients require general anesthesia and profound relaxation.
Keywords: High frequency jet ventilation; HFJV; Subglottic stenosis; Thoracotomy; Tracheal resection; Tracheal reconstruction; Tracheo-esophageal fistula
Citation: Ahmed N, Naseem K, Rafiq M. Anesthetic challenges in tracheal resection and reconstruction surgery. Anaesth Pain & Intensive Care 2018;22(3):323-329
Received: 18 Aug 2018, Reviewed: 22 Aug 2018, Corrected & Accepted: 15 Sep 2018
INTRODUCTION
The anesthetic challenges of major tracheobronchial surgery relate to airway control, ventilation management, maintaining optimal surgical exposure and appropriate patient selection. Anesthesia for tracheal resection and reconstruction is one of the most challenging ones for anesthesiologist because of the compromised airway.1 Only a few centers have relevant expertise and many of the experienced anesthesiologist may be unfamiliar with its successful management. The need to share the airway requires very close communication and coordination between the surgical and the anesthesia teams. Conditions unique to this disorder include a stenosed airway, difficulties with maintaining ventilation and oxygenation during induction, bronchoscopy and during surgical procedure. Non-conventional modes of ventilation and oxygenation like high frequency jet ventilation (HFJV), extra corporeal membrane oxygenation (ECMO) or ventilation across surgical field are the unique techniques which are often needed for successful ventilation and oxygenation. A through preoperative assessment, good plan for induction and intubation, close coordination with the surgeon during intubation, excision and anastomosis, expert management of expected emergencies and postop care are the fundamentals of successful outcome. Avoidance of coughing and bucking, and awake extubation at the end of surgery are desirable. Neck is placed in flexed position which is achieved with chin sutures ensuring that the airway anastomosis is tension free.
We aimed to share our experience regarding anesthetic management and outcome of 21 cases of tracheal resection and reconstruction surgery for tracheal stenosis carried out at two military hospitals between October 2014 and July 2018.
METHODOLOGY
This prospective, descriptive study was carried out at PNS Shifa Hospital Karachi and Combined Military Hospital Rawalpindi between October 2014 and July 2018. All patients (21) undergoing tracheal resection and reconstruction surgery for tracheal stenosis at these centers between age 6 – 66 years of ASA physical status II-IV were enrolled. Informed consent was obtained from all patients and institutional ethics committee approval was secured. All were elective cases and proper pre-anesthesia assessment was done a day or two before operation and besides routine investigations, special tests including PFTs, ABGs, flow Volume Loops, CT scan chest, 2D echo was done. Fiber optic Bronchoscopy was performed by the surgeons pre-operatively in all cases to determine site and extent of lesion. Patients with severe pulmonary disease and multiple co morbidities were excluded from the study. For proper optimization; bronchodilators, chest physiotherapy and appropriate antibiotics were advised when required. Informed high risk consent was taken and counseling was done in detail. Two units of RCC were arranged in all cases and ventilator bed in surgical ICU/ HDU was confirmed.
In operating room two large bore IV cannulas were secured and monitors were attached including ECG, NIBP, SpO2, EtCO2 and temperature. Thoracic epidural catheter was placed before induction in seven of the patients scheduled to be operated by right thoracotomy incision. No premedication was given to any patient. Intravenous induction with propofol 2 mg/kg was used in 7 patients who had tracheostomy in situ and in 8 cases with mild to moderate stenosis without stridor, and they were intubated with 6 -7 mm cuffed endotracheal tube. Inj atracurium 0.6 mg/kg was used as muscle relaxant. One patient of tracheal tumor required awake fiberoptic intubation due to difficult airway. Inhalational induction in rest of the five cases was achieved with sevoflurane 6-8% in 50% O2 in air and they were intubated when adequately deep, maintaining spontaneous breathing without muscle relaxant. Inj nalbuphine 0.1 mg/ kg and inj paracetamol 15 mg/kg was used for analgesia. Once anesthetized, all the patients were catheterized and arterial line was passed for urine output and IBP monitoring. CVP line in right internal jugular vein was passed in seven cases that were operated by right thoracotomy incision. The stenosed portion of trachea was excised. Before the start of reconstruction and anastomosis the distal tube was removed and the proximal one reintroduced across the proposed anastomosis line, its cuff was inflated and ventilation resumed through this tube. Anastomosis started first with posterior and lateral sutures and finally completed anteriorly. Neck was placed in flexed position with the help of chin sutures (Figure ).

Figure 1: Neck flexion achieved with chin suture
At the end of surgery all patients were reversed with injection neostigmine and glycopyrrolate (Except one who developed cardiac arrest during operation who was electively ventilated for 24 h). Seventeen cases were extubated successfully on operating table. Demographic data was recorded in MS Microsoft Excel 2010 and descriptive analysis was done using frequencies and percentages.
RESULTS
Out of 21 patients, 9 (43%) were male and 12 (57%) were females between 6 to 66 years of age of ASA II- IV. Table I.
Table 1: Demographic data. [n (%)]
| Parameters | No. of Patients
n= 21 |
| Age (years) | 29 ± 12 (6-66)* |
| Gender
· Male · Female |
9 (43) 12 (57) |
| ASA Physical Status
· II · III · IV |
12 (57) 7 (33) 2 (1) |
| Tracheostomy | 7 (33) |
*mean ± SD (Range)
Post intubation stenosis was the leading cause of tracheal stenosis followed by tracheal tumors, trauma and corrosive ingestion (Figure 2).
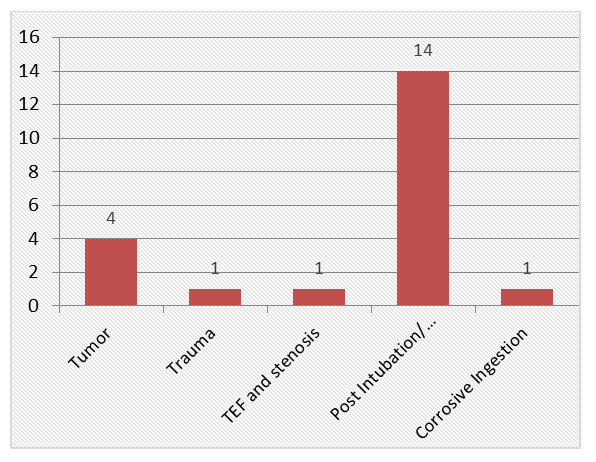
Figure 2: Etiology of tracheal stenosis
Out of 21 patients, seven had a tracheostomy in situ. Fourteen patients had high cervical / subglottic stenosis and were operated by high anterior cervical collar incision, while five had lower tracheal stenosis, and two had carinal lesions and were operated by right thoracotomy (Figure 3).
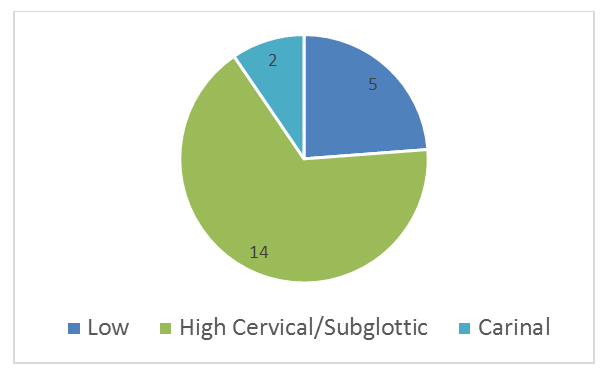
Figure 3: Site of stenosis
Seven patients were anesthetized through tracheostomy tube, one by fiberoptic intubation and the rest with 5-7mm ETT with or without muscle relaxant. One patient developed cardiac arrest during surgery but was revived successfully. Four (19%) out of 21 had to be put on ventilator postoperatively while remaining 17 (81%) were extubated on operating table. Two patients on ventilator were weaned off successfully. Outcome was excellent in 19 (90%) cases while in 2 (10%) patients, operation was unsuccessful and they landed up with permanent tracheostomy. Perioperative mortality was zero although one patient died of acute MI eight months after surgery.
Discussion
The trachea extends from cricoid cartilage to carina (C6-T4). In adult it is 10 – 12cm long, 1.5-2cm in diameter and consists of C shaped cartilaginous ring anteriorly and fibro muscular tissue posteriorly which abuts the esophagus. Its first 2cm from vocal cords to cricoid is called subglottic airway and one third of the trachea is extra thoracic. Although it has a rich blood supply but its mucosa is vulnerable to ischaemic injury by high intra cuff pressure of endotracheal or tracheostomy tube. Seventy five to 90% cases of tracheal stenosis are due to prolonged intubation or tracheostomy and in United States the incidence is 4-13% in adult and 1-8% in neonates2. Other causes are tumor (primary or secondary) 3, trauma, infection, congenital causes and in our part of the world suicide attempt with corrosive ingestion. Symptoms start when tracheal diameter is reduced to 50% and wheeze or stridor appears when it is 5mm or less. There is persistent cough and progressive dyspnea and patients are often mistakenly been treated for asthma.
A thorough pre anesthetic assessment including a detail history, clinical examination and investigations, preoperative preparation and planning and discussion with surgeon is mandatory. There may be history of prolong endotracheal intubation or tracheostomy. X- ray chest may show narrowing of air column (Figure 4). Standard CT of chest is not sensitive enough and may require high resolution CT with virtual bronchoscopy and 3D reconstruction (Figure 5). Flow volume loop and pulmonary function tests are valuable for detection of site (intra or extra thoracic), type (variable or fixed), or obstructive / restrictive disease pattern. Preoperative fiber optic bronchoscopy is done to determine site and extent of lesion. Cardiac assessment is mandatory including echocardiography.
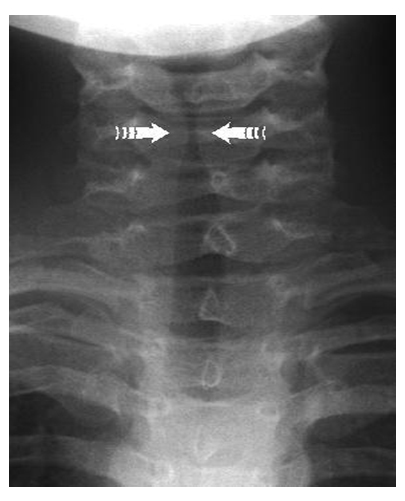
Figure 4: X-ray chest showing narrowing of air column
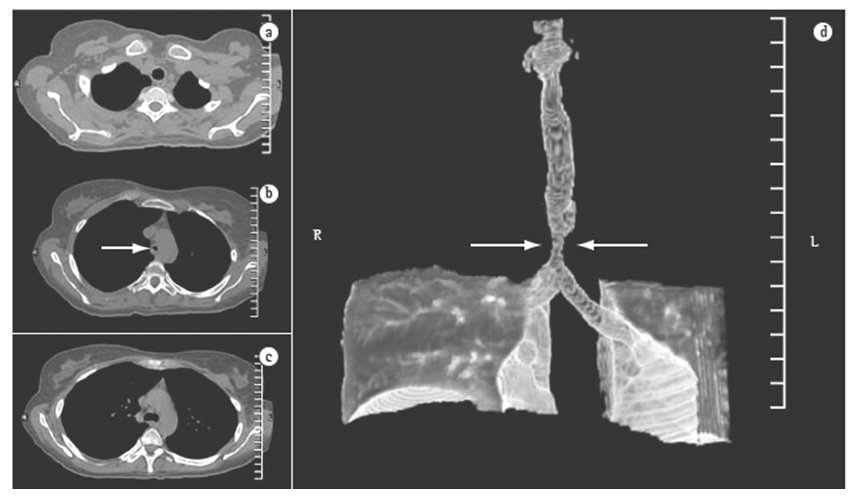
Figure 5: (a, b, c); CT scan of chest; axial slices (d) Three dimensional reconstruction. White arrows show tracheal stenosis
Special equipment needed are assortment of small diameter ETT, high frequency jet ventilation machine, adult and pediatric fiberoptic and rigid bronchoscopes, sterile armored tube, sterile tubing with connectors etc.
Two peripheral large bore IV lines are normally sufficient, but pronged surgery and blood loss require central line which is preferred in subclavian or femoral vein. Premedication is generally avoided because there may be loss of airway control or it may thicken the secretion. Monitoring includes NIBP, IBP, ECG, SpO2, EtCO2, Temperature, urine output and neuromuscular monitoring. Minor degree of airway obstruction can be induced with propofol and intubated with neuro-muscular relaxation. Critical obstruction require deep inhalational induction with sevoflurane and intubation with spontaneous breathing. Induction may be through tracheostomy if present in situ. In difficult airway situation, awake fiber optic intubation is recommended. Whichever method is adopted a back up plan should be ready for securing airway and ventilation in emergency. The tip of ETT should be kept either above the stenosis or smaller tube can be passed distal to the lesion. Surgery is performed either through anterior cervical collar incision, through median sternotomy or right thoracotomy. When trachea is opened, the oral tube is pulled proximally but still in trachea and usually, a sterile armored cuffed endotracheal tube is placed under vision across surgical field by the surgeon to the distal airway for the period of segmental resection followed by reintroduction of the native orotracheal tube under vision for the primary end-to-end anastomotic reconstruction.4 Alternatively intermittent cannulation and decannulation may be required or high frequency jet ventilation may be used. Cardiopulmonary bypass is reserved in very severe stenosis especially at carina and in neonates.5 To avoid stress on suture line the neck is kept in flexed position with the help of chin sutures. Alternatively Mueller Fiberglass Orthosis Splint6 or Shiraz Brace7 can be applied. Anastomotic leak is checked with 20-30 cmH2O positive pressure ventilation. Reversal of NM block, thorough suction of airway and an awake patient extubated on OT table is desired. Preparation for intubation and re-intubation should be at hand preferably with FOB. Patients often need nebulization and are kept in ICU with neck in flexed position for 7 days. Mortality in experienced center is 3%.8 Complications may be early or late. Early complications include laryngeal edema or recurrent laryngeal nerve damage which may present as hoarseness. Late complications are wound dehiscence, anastomotic granuloma, stenosis, infection, vocal cord paralysis and disruption of suture line.
Tracheal resection and reconstruction is required in patients with tracheal stenosis which may be due to prolonged intubation and tracheostomy, primary and secondary tracheal tumor, tracheal trauma, congenital or in our part of the world following failed suicide attempt with corrosives. Other management options for tracheal stenosis are intermittent dilatation, laser ablation,9 tracheal stents and artificial engineered tracheal tissue and tracheal transplant.10 The anesthetic concerns are a compromised airway, early airway control, ventilation and oxygenation throughout the procedure. The surgeon requires an unobstructed and motionless field. So close communication and coordination between the two team is crucial. Airway can be secured either via preexisting tracheostomy tube, different varieties of ETT, high frequency jet ventilation (HFJV) or LMA. In our study we used tracheostomy or direct endotracheal intubation and ventilation. Krecmerova M.11 has described successful use of LMA in a retrospective analysis of 54 cases of tracheal surgery. The surgical approach in our study was high anterior cervical collar incision and right thoracotomy. There is increasing interest of doing this procedure with minimal invasive VATS technique with four, three or even one port. He J. and colleagues showed improvement in minimal invasive VATS surgery for tracheal resection during recent past. In five paper they published between November 2015 and November 2016,12,13,14,15,16 they showed the improvement from resection of a tracheal mass with three-port-VATS under non-intubated anesthesia,12 followed by VATS with carinal reconstruction13 and finally in single port VATS for tracheal resection in a spontaneous breathing patient16. Fung et al. has reported a case of elective veno-venous Extra Corporeal Membrane Oxygenation (ECMO)17 and high flow nasal oxygen for subtotal resection of a distal malignant tumor. In our study we used muscle relaxant and intubated the distal airway across the surgical field in all cases and ventilated with IPPV or manually. Khalid K et al.18 at Agha Khan Hospital Karachi has reported a case of anesthetic management of tracheal reconstruction using manual jet ventilation (JV) with Sander’s injector (Instrumentation Industries Inc, Bethel Park, PA). Cardio pulmonary bypass is preferred for tracheal resection and reconstruction surgery in neonates and in complicated carinal reconstruction.19 Subglottic and high tracheal stenosis are easy to operate (Figure 6), but carinal surgeries are most challenging both for surgeon and anesthetist. Broadly, approaches for carinal resection and reconstruction fall in three categories. Firstly those requiring only tracheal resection, cross field intubation to distal airway is traditionally used. Secondly surgery requiring full carinal resection and reconstruction, cross-field ventilation as described above and the cross-field tube is inserted into the left main bronchus after the carina is resected. Thirdly surgery requiring partial carinal resection/ reconstruction and right bronchial resection, cross-field ventilation is not necessary in this case. A small single lumen ET intubation can be advanced directly into the left main bronchus for the procedure (Figure 7).20
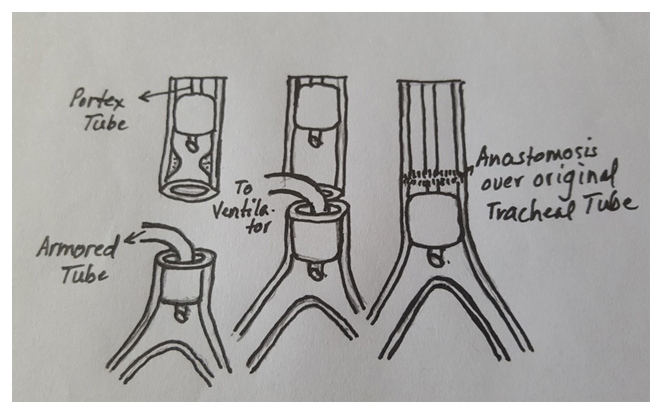
Figure 6: Ventilation during tracheal resection and reconstruction in lower tracheal stenosis
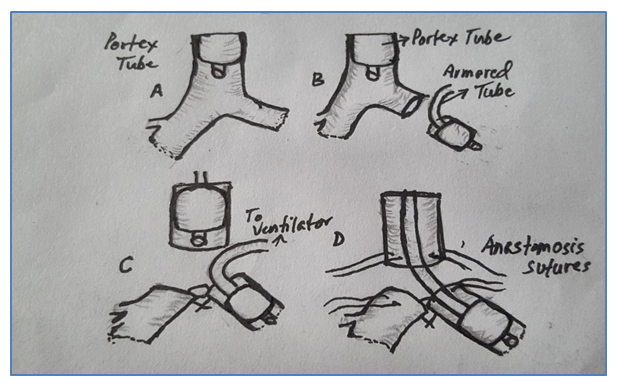
Figure 7: Carinal resection and reconstruction
In our study one patient of subglottic stenosis developed cardiac arrest due to hypoxia following delay in cannulation of distal trachea in the neck which got retracted inside chest but fortunately it was retrieved and the patient was revived successfully. An awake extubation on operating table is desirable and in our study we extubated seventeen patients on operating table. Two patients developed repeated anastomotic leak and disruption of suture line and infection and landed with permanent tracheostomy. Noh KB et al.21 has reported paraplegia, a rare complication after tracheal resection anastomosis surgery. Possible explanation according to him may have been extreme neck flexion in post-operative period causing compression on anterior spinal artery. In our study outcome was excellent in 19 patients with 90% success rate which is comparable with international figures. Operative mortality was zero although one obese lady who was operated for lower tracheal tumor died of acute MI eight months after surgery.
LIMITATIONS
Sample size was small because this surgery is relatively performed only in a few centers in Pakistan. A larger sample size would have enhanced the validity of this study.
CONCLUSION
Prevention is better than cure. Meticulous attention of endotracheal and tracheostomy tube and its intra cuff pressure is the most desirable preventive measure with strict vigilance and high quality professional nursing care. Tracheal resection and reconstruction is a relatively rare surgical procedure and is a challenging job for the anesthetist which requires expertise. The crux of anesthetic management is securing the airway early and maintenance of ventilation and oxygenation during resection and reconstruction. Thorough preoperative assessment, preparation, intra operative management, a backup plan and close communication between the surgeon and anesthesiologist are necessary for successful outcome. Most of these patients require general anesthesia and profound relaxation.
Picture credits: Picture/ Images/ Diagram credits: Dr. Naseem Ahmed and
Radiology Department.
Conflict of interest: None declared.
Author’s Contribution:
NA: Study design, literature review, manuscript writing.
KN: Statistical analysis, proof reading.
MR: Manuscript review and editing.
REFERENCES
- McCaffrey TV. Classification of laryngotracheal stenosis. Laryngoscope. 1992;102:1335-40. DOI: 1288/00005537-199212000-00004 [PubMed]
- Cho JW, Jeong MA, Choi JH et al. Anaesthetic Considerations for Surgery of the Trachea and main Bronchi. Anaesthesia & Intensive Care Medicine. 2017 Nov 21;18(12):300-302.
- Beyer PY, Wilson RS. Anesthetic management of tracheal resection and reconstruction. Journal Cardiol Anesth. 1988;2:821-2.
- Mueller DK, Becker J, Schell SK, Karamchandani KM, Munns JR, Jaquet B. An alternative method of neck flexion after tracheal resection. Annals of Thoracic Surgery. 2004;78(2):720-1. DOI: 1016/j.athoracsur.2003.09.024 [PubMed]
- Ziaian B, Foroutan A, Tahamtan M, Moslemi S. A new brace for maintaining the neck in a suitable position following tracheal reconstruction. Iran J med Sci. 2014;39(3):308-310. [PubMed] [Free Full Text]
- Gaissert HA, Grillo HC, Shadmehr MB, Wright CD, Gokhale M, Wain JC, et al. Long term survival after resection of primary adenoid cystic and squamous cell carcinoma of trachea and carina. Ann Thorac Surg. 2004;78(6):1889-96. DOI: 1016/j.athoracsur.2004.05.064 [PubMed]
- Cho JW, Jeong MA, Choi JH, Cho JW, Lee HJ, Kim DW, et al. Anesthetic consideration for patients with severe tracheal obstruction caused by thyroid cancer. a report of 2 cases. Korean J Anesthesiol. 2010;58(4);396-400. DOI: 4097/kjae.2010.58.4.396 [PubMed]
- Mentzelopoulos SD, Tzoufi MJ. Anesthesia for tracheal and endobroncheal interventions. Curr Opin Anaesthesiol. 2002;15(1):85-94. [PubMed]
- Jungebluth P, Moll G, Baiguera S, Macchiarini P. Tissue engineered airway: a regenerative solution. Clin Pharmacol Ther. 2012;9(1):81-93. DOI: 1038/clpt.2011.270 [PubMed]
- Krecmerova M, Schutzner J, Michalek P, Johnson P, Vymazal T. Laryngeal mask for airway management in open tracheal surgery—a retrospective analysis of 54 cases. J Thorac Dis. 2018;10(5):2567-72. DOI: 21037/jtd.2018.04.73 [PubMed]
- Li S, Liu J, He J, Dong Q, Liang L, Cui F, et al. Video assisted transthoracic surgery resection of a tracheal mass and reconstruction of trachea under non-intubated anesthesia with spontaneous breathing.J Thorac Dis. 2016;8(3):575-85. DOI: 21037/jtd.2016.01.62 [PubMed]
- He J, Wang W, Li J, Yin W, Xu X, Peng G, et al. Video assisted thoracoscopic surgery tracheal resection and carinal reconstruction for tracheal adenoid cystic carcinoma.J Thorac Dis. 2016;8(1):198-203. DOI: 3978/j.issn.2072-1439.2016.01.45 [PubMed]
- Peng G, Cui F, Ang KL, Zhang X, Yin W, Shao W, et al. Non-intubated combined with video-assisted thoracoscopic in carinal reconstruction.J Thorac Dis. 2016;8(3):586-93. DOI: 21037/jtd.2016.01.58 [PubMed]
- Liu J, Li S, Shen J, Dong Q, Liang L, Pan H, et al. Non-intubated resection and reconstruction of trachea for the treatment of a mass in the upper trachea.J Thorac Dis. 2016;8(3):594-9. DOI: 21037/jtd.2016.01.56 [PubMed]
- Guo M, Peng G, Wei B, He J. Uniportal video assisted thoracoscopic surgery in tracheal tumour under spontaneous ventilation anaesthesia.Eur J Cardiothorac Surg. 2017;52(2):392-4. DOI: 1093/ejcts/ezx076 [PubMed]
- Fung RKF, Stellios J, Bannon PG, Ananda A. Forrest P. Elective use of veno-venous extracorporeal membrane oxygenation and high-flow nasal oxygen for resection of subtotal malignant distal airway obstruction. Anaesth Intensive Care. 2017;45(1):88-91. [PubMed]
- Khalid S, Faisal S, Sohail A, Qamarul H. Anaesthetic management of tracheal reconstruction using jet ventilation (jv). J Anaesth Clin Pharmacol. 2008;24(1):79-82. [Free Full Text]
- Beyer PY, Wilson RS. Anesthetic management of tracheal resection and reconstruction. Journal Cardiol Anesth. 1988;2:821.
- Keng A, Guiling PL, Jing PL, Jian XE. Video assisted thoracoscopic tracheal and carinal resection. perspectives in cardio thoracic surgery.The SCTS- Ionescu and Ireland. 2017;2(12):155-162.
- Noh KB. Khairul B, Irfan M, Thevagi M, Sanjeevan N, Fariza NH. Paraplegia as a rare complication of tracheal resection anastomosis. Int J Otorhinolaryngol Head Neck Surg. 2018 May;4(3):823-825. DOI: http://dx.doi.org/10.18203/issn.2454-5929.ijohns20181877



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube