
Imran Amer, FCPS-I1, Shahid Hafeez, DA2, Zahid Rafique: FRCA, FFARCSI3
1House Officer Anaesthesia Jinnah Hospital, Lahore (Pakistan)
2Consultant Anesthetist, Aziz Bhatti Shaheed Hospital, Gujrat (Pakistan)
3Consultant Anesthetist, Hull and East Yorkshire Hospitals NHS Trust, (UK)
Correspondence: Dr Zahid Rafique (FRCA, FFARCSI, MSc Pain management); Consultant Anaesthetist, Hull and East Yorkshire Hospitals, NHS Trust, Anlaby Road, Hull HU3 2 JZ, (UK); E-mail: zahidrafique175@hotmail.com
ABSTRACT
Objectives: Maternal mortality rate remains unacceptably high in Pakistan. Nearly 200 women die in Pakistan for every 100000 live births as compared to 8 in Europe. According to Pakistan Demographic and Health Survey (PDHS) 2006-2007, anesthesia is one of the contributing factors to this high mortality rate. The aim of this survey was to find out what standards and guidelines in obstetric anesthesia are followed by anesthesiologists in teaching and district hospitals in Punjab, which is the largest province of Pakistan.
Methodology: From January 2016 to March 2016, seventeen teaching hospitals and twenty-four district hospitals in Punjab were asked to take part in telephonic or face-to-face survey. Questions were asked regarding the availability of internationally acceptable guidelines and protocols for managing obstetric emergencies like massive hemorrhage and failed intubation. Questions were also asked about the availability of equipment for difficult airway, blood products and regional anesthetic techniques used for cesarean sections. Data were collected in Microsoft Excel format and analyzed using simple statistics
Results: Overall availability of guidelines was lowest for massive hemorrhage (12%) and highest for managing difficult intubation (29%). For the management of difficult airway only 36% had endotracheal tube introducers. For major obstetric hemorrhage, 68% of the hospitals could get blood in 30 min and 24% could get fresh frozen plasma (FFP) in 30 min. Regional anesthesia was the preferred technique in all the government hospitals. For performing spinal anesthesia all of the anesthesiologists used sterile gloves while 51% used masks and gowns and only 39% washed their hands before spinal. Sensation of pain and leg raising were the main modalities used to test the spinal block with 41% anesthesiologists considering block up to T8 a good level to start cesarean section. 85% anesthesiologists used 25G Quincke spinal needle.
Conclusion: Our survey showed a grim state of affairs as far as obstetric anesthesia in government hospitals of Punjab is concerned however; a comprehensive survey is needed to draw final conclusions and make further recommendations.
Key words: Maternal mortality rate; Questionnaire; Teaching hospitals; District headquarter hospitals; Guidelines
Citation: Amer A, Hafeez S, Rafique Z. A survey of obstetric anesthesia practices in district level and government teaching hospitals in Punjab, Pakistan. Anaesth Pain & Intensive Care 2017;21(2):212-217
Received: 26 May 2016, Reviewed: 27 May 2016, 24, Jan, 12 Mar 2017, Corrected: 13, 14 Jun, 13, Dec 2016, 21 Jul 2017, Accepted: 21 Jul 2017
INTRODUCTION
Pakistan continues to be among the countries with high to very high maternal mortality.1 According to Pakistan Demographic and Health Survey (PDHS) 2006-2007, the National Maternal Mortality Ratio (MMR) in Pakistan was 276 per 100,000 live births.2 Difference between Rural and Urban areas was quite remarkable. The MMR was almost twice as high in rural areas (319) than in urban (175).2 One of the disturbing facts in the PDHS report was the number of deaths that were classified as iatrogenic i.e. due to improper management and negligence in hospital settings. This included deaths due to general anesthesia complications.
Obstetric anesthesia presents unique challenges to anesthesiologists. These challenges range from providing simple pain relief during labor to the management of life threatening issues like difficult airway, spinal hypotension, major obstetric hemorrhage and pre-eclampsia. To cope with these challenges Anesthesia and Obstetric organizations all over the world have issued guidelines and protocols.3,4,5,6 As there is very little data regarding the implementation of these guidelines in Pakistan, we carried out a survey of 17 teaching hospitals (TH) and 24 district headquarter (DHQ) hospitals in Punjab, which is the biggest province in Pakistan, to look at the practices of obstetric anesthesiologists in those hospitals.
METHODOLOGY
The study was performed as a cross-sectional questionnaire survey. Ethical approval for the project was acquired from The Research and Development department of the University of Gujrat. Between January and March 2016, questionnaires were either presented face to face or via telephone to the Head of the anesthesia department. There are 23 TH and 34 DHQH in Punjab. We managed to survey 17 (74%) TH and 24 (71%) DHQ hospitals of Punjab.
The questionnaire contained questions about the availability of obstetric anesthesia guidelines. These guidelines have been issued by the world’s leading professional organizations. They have been published in anesthesia journals and are freely available on the internet. It is recommended that all hospitals should have written protocols according to their circumstances based on these guidelines.
Further questions were asked regarding the availability of airway adjuncts during difficult intubation as per the guidelines of Difficult Airway Society (DAS).5 , availability of blood products during major obstetric hemorrhage as per guidelines by RCOG.6 , the availability and use of different kinds of fluids and inotropes to treat maternal hypotension, practice of aseptic measures in performance of spinal anesthesia, ways of testing spinal block and height of block at which to start surgery, (according to present guidelines by Obstetric Anesthesiologists Association (OAA), and types of spinal and epidural needles used.
Questions were framed so as to require a simple “yes” or “no” answer. All the responses were entered in Microsoft Excel sheet; simple statistics were used to convert the responses to numerical percentages. Results were tabulated and also graphically presented in the form of bar charts.
RESULTS
The results available from all the hospitals included in the survey are presented in Table 1. The availability of guidelines or written protocol was between 4-8% in the DHQ hospitals while it ranged from 29-59% in the TH (Table 1). Majority of the guidelines available in the TH were those for the management of failed intubation (59%), hypotension (53%) and management of PDPH (53%). Guidelines or protocols for managing major obstetric hemorrhage (23.5%), management of pre-eclampsia (41%) and guidelines for nil by mouth policy (29%) fared less well in our survey.
All TH and DHQ hospitals had complete availability of laryngoscopes and different sizes of blades (100%). Trained anesthesia assistant was present in 82% of TH but only in a 29% DHQ hospitals. McCoy laryngoscopes were available in 41% of TH and 13% of DHQ hospitals. Endotracheal tube introducer (bougie), a simple intubating aid was available in 59% TH and 21% district hospitals. I-gel and 2nd generation supraglottic devices are now recommended by the latest guidelines of Difficult Airway Society (DAS).5 These are available in 76% of TH and 38% of DHQ hospitals. Videolaryngoscope and cricothyrotomy sets were not available in any of the DHQ hospitals whereas 18% of TH reported their availability.
In all teaching and DHQ hospitals, anesthesiologists had immediate access to crystalloids; 93% had colloids too. FFP were available within 30 min of demand in 47% of teaching and 13% of DHQ hospitals; whereas platelets could be arranged within 60 min in 35% of teaching and only 4% of DHQ hospitals.
Regarding the use of inotropes/vasoconstrictors for spinal hypotension, phenylephrine was the drug of choice in 82% and 67% of the TH and DHQ hospitals respectively (Table 1).
Regarding asepsis during spinal/epidural anesthesia, sterile gloves were used by 100% of anesthesiologists in all hospitals. The practice of hand washing before a spinal/epidural was more prevalent in DHQ hospitals (46%) as compared to TH (29%). No other hand scrub was used in either of the subsets.
For testing a spinal block, anesthesiologists in DHQ hospitals favored leg raising test (79%) while testing pain sensation with blunt needle was the preferred mode of testing at TH (76%). Use of cold for sensory testing was noted in 29% and 4% of the teaching and DHQ hospitals respectively (Figure 1).
47% anesthesiologists in TH preferred a block up to T4 compared with 12% in district hospitals. Overall 41% anesthesiologists let surgery to start at T8 level (Figure 2). Pencil point spinal needles were not available in any of the government hospitals. 25G Quincke spinal needle was used by 88% TH and 83% DHQ hospitals. The use of 27G Quincke was 35% and 29% respectively (Figure 3).
Table 1: Comparative responses by teaching and DHQ hospitals to the questionnaire
| Questions |
Teaching hospitals n=17 |
DHQ hospitals n=24 |
Total N (%) |
| Are the guidelines available in your department regarding… | |||
| · Management of major obstetric hemorrhage | 4 | 1 | 5 (12) |
| · Management of failed Intubation | 10 | 2 | 12 (29) |
| · Management of hypotension | 9 | 2 | 11 (27) |
| · Management of PDPH | 9 | 1 | 10 (24) |
| · Management of pre-eclampsia | 7 | 1 | 8 (19) |
| · Oral intake during labor | 5 | 1 | 6 (15) |
| · Oral intake before and after LSCS | 5 | 1 | 6 (15) |
| With regards to difficult airway, are the following available; | |||
| · Different sizes of laryngoscope blades | 17 | 24 | 41 (100) |
| · A trained assistant | 14 | 7 | 21 (51) |
| · McCoy laryngoscope | 7 | 3 | 10 (24) |
| · Gum elastic bougie | 10 | 5 | 15 (36) |
| · I-gel/ LMA Supreme | 13 | 9 | 22 (53) |
| For the management of major obstetric hemorrhage | |||
| · Do you have crystalloids available immediately | 17 | 24 | 41 (100) |
| · Do you have colloids available immediately | 16 | 22 | 38 (93) |
| · Do you have blood available in 30 min | 13 | 15 | 28 (68) |
| · Do you have FFP available in 30 minute | 8 | 3 | 11 (27) |
| · Do you have platelets available in 60 min | 6 | 1 | 7 (17) |
| Which inotrope do you use to treat spinal hypotension? | |||
| · Ephedrine | 6 | 10 | 16 (39) |
| · Phenylephrine | 14 | 16 | 30 (73) |
| · Adrenaline | 10 | 13 | 23 (56) |
| · Noradrenaline | 1 | 3 | 4 (10) |
| · Atropine | 1 | 5 | 6 (15) |
| Regarding aseptic technique for spinal anesthesia | |||
| · Do you wear a mask while doing the spinal/epidural | 12 | 9 | 21 (51) |
| · Do you wear a sterile gown for spinal/epidural | 12 | 9 | 21 (51) |
| · Do you wear a sterile gloves for spinal/epidural | 17 | 24 | 41 (100) |
| · Do you wash your hands before doing a spinal/epidural | 5 | 11 | 16 (39) |
| · Do you clean patients back before spinal/epidural | 17 | 17 | 34 (83) |
| What do you use for cleaning patient’s back | |||
| · Iodine-povidone solution | 17 | 24 | 41 (100) |
| · Chlorhexidine | 1 | 0 | 1 (3) |
| · Alcohol | 0 | 2 | 2 (5) |
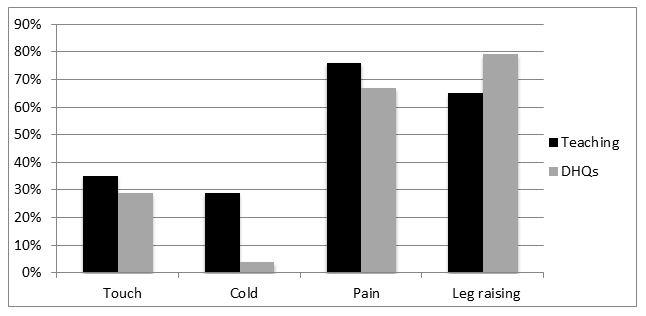
Figure 1: Test used to determine sensory and motor block level in teaching and district hospitals
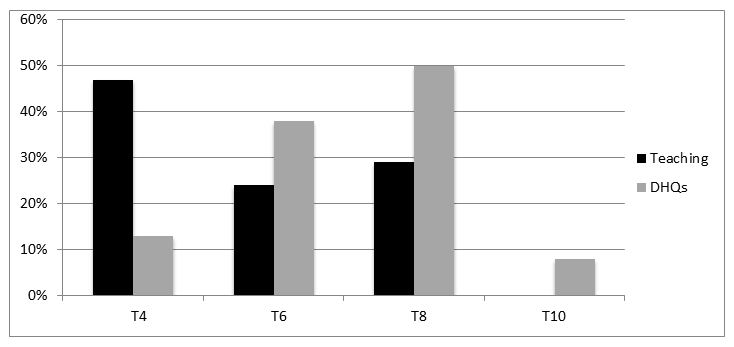
Figure 2: Level of block desired before starting cesarean at teaching vs. district hospitals
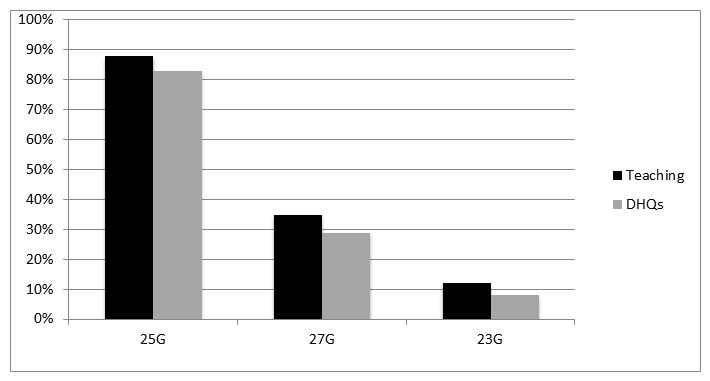
Figure 3: The gauge of spinal needle used in teaching and district hospitals
DISCUSSION
In 2013, an estimated 289000 mothers died during pregnancy and childbirth, across the globe. Pakistan contributed nearly 8000 maternal deaths to this number.1 Fact is that maternal and fetal mortality is unacceptably high in developing countries, and the practice of obstetric anesthesia has an important influence on this outcome. To safeguard against maternal morbidity and mortality, professional organizations throughout the world have issued guidelines and set protocols for the obstetric anesthesiologists. These organizations include OAA, Royal College of Anesthesiologists UK, Difficult Airway Society (DAS), Association of Anaesthetists in Great Britain and Ireland (AAGBI) and many more. OAA recommends that departments should have written guidelines, setting out local standards of care..3
Our survey showed that the published guidelines/protocols were available in 10% of the district hospital departments; the figures varied amongst the teaching facilities. Guidelines for management of failed intubation, hypotension and PDPH were present in about 50% of TH and rest of the guidelines like management of postpartum hemorrhage and management of post dural puncture headache were present in lesser proportions even in the TH. McGarrity et al. showed that most of the OAA/AAGBI recommended emergency guidelines such as those for hemorrhage, pre-eclampsia/eclampsia and difficult/ failed intubation were available in all units in UK.7 A similar result would benefit Pakistan a lot.
Our study also shows a major difference between the secondary and tertiary obstetric anesthesia facilities with regards to adequate basic equipment for management of difficult airway. Maternal Airway complications are known cause of maternal mortality,5 but most of the DHQ’s lack even the simplest equipment like gum elastic bougies and 2nd generation LMA’s for the management of difficult airway. Both these are among the “must haves” in Difficult Airway Society (DAS) guidelines.5 More advanced equipment like Video laryngoscope and life saving cricothyrotomy sets were only available in 18% of TH and none of the DHQs.
Peripheral hospitals also lag behind in terms of immediate availability of life-saving blood products such as FFP and platelets. 63% of the DHQs could get fresh blood within 30 min through a donor arranged by patients’ family but not through hospital’s blood bank. Other essential blood components like FFP and platelets were even more difficult get. These products must be available within a short span of time interval if young lives are to be saved after postpartum hemorrhage. RCOG has published comprehensive guidelines on the management of postpartum hemorrhage,6 and we need similar guidelines in Pakistan as well.
Neuraxial anesthesia remains the preferred choice for Cesarean deliveries across the world.7 In our survey 95% cesareans are being done under regional anesthesia in periphery while in TH in big cities percentage drops down to 85%. Spinal anesthesia causes hypotension in as much as 55% to 90% of the mothers receiving spinal anesthesia for cesarean section.8 The American Society of Anesthesiologists Task Force on Obstetric Anesthesia recommends phenylephrine for improved fetal acid-base status in uncomplicated pregnancies.4 In our survey, phenylephrine was the preferred vasoconstrictor used to treat maternal hypotension (used by 73% anesthesiologists ) followed by adrenaline (used by 56%). It is interesting to see the use of adrenaline in obstetrics as it is certainly not the agent of choice because of its detrimental effects on fetus and relaxant effects on the uterus.9 Reason for it use may be low cost of adrenaline which is 10 times cheaper than phenylephrine in Pakistan. Noradrenaline, has shown promise in recent studies, and is now considered by many as a better vasoconstrictor in obstetrics than phenylephrine.10,11 This will be important from Pakistan point of view since Noradrenaline is also freely available in Pakistan.
Aseptic technique is pivotal for the practice of central neuraxial block (CNB). Optimum aseptic technique for CNB requires thorough hand washing with surgical scrub solution, use of barrier precautions including the wearing of a cap, mask, sterile gown and gloves, and use of a large sterile drape.12 In our survey practice of hand washing was poor although 100% of the anesthesiologists used sterile gloves, In District hospitals 38% of district anesthesiologists used masks and gown while this percentage was 70% in TH.
The assessment of block height following the administration of a regional anesthetic block for cesarean section is very important for pain free surgery. However, the best method for assessing the block has always been a subject for debate.13 There are multiple methods for assessing the height of block, and surveys have consistently demonstrated a marked variation in techniques among anesthesiologists.14 However, Ian Russell’s views are generally more acceptable internationally that loss of sensation to touch is the most appropriate way to test the height of block and T6 is the most acceptable level of block.15,16 Our finding suggests that anesthesiologists in Punjab favor leg raising and sensation of pain to pin prick as methods of choice to test their height of block. However, it is worrying to note that almost 50% of district anesthesiologists and 30% of TH anesthesiologists would let the surgery start at T8 level as opposed to internationally accepted level of T6. This can result in considerable pain and discomfort for the patient.
Post dural puncture headache (PDPH) is one of the most debilitating complications of spinal anesthesia. When using Quincke spinal needle the incidence of PDPH is directly related to the size of the needle. When performing spinal anesthesia for cesarean section with 25 G Quincke needle incidence of PDPH is between 6 – 8% and 3% with 27 G. When 25 G Whitacre spinal needle is used the incidence of PDPH drops down to less than 2%.17 Our survey suggested that 25G Quincke spinal needle is the most commonly used needle for spinal anesthesia in all the hospitals we surveyed followed by 27 G Quincke. Pencil point spinal needles were not available in any of the government hospitals.
LIMITATIONS
We acknowledge that this was a small scale survey of obstetric anesthesia and had its limitations. We could not reach all the intended hospitals either because of logistic difficulties or unavailability of appropriate communication resources. Despite the difficulties we surveyed more than 70% of the hospitals in the Punjab province of Pakistan, which may be termed as satisfactory by any standards. Survey is also limited by the content which could be more comprehensive but this was just a start and we intend to do a more comprehensive survey very soon.
CONCLUSION
Despite the limitations, results of this survey do give a glimpse of overall grim state of affairs in government hospitals in Punjab. Lack of guidelines and protocols, unavailability of essential airway equipment and lack of blood and blood products are three major factors which can impact maternal mortality adversely. Root cause of the shortages of essential items is underfunding and mismanagement of available resources by the relevant authorities. If any recommendations are to be made then a much bigger and comprehensive survey is needed to get a clearer picture of obstetric anesthesia practices all over Pakistan. In the meantime a responsible professional body in Pakistan needs to make sure that the current guidelines and protocols are available in each and every hospital of the country.
Conflict of interest: The authors declare no conflict. The study was conducted without any external funding
Author’s Contributions:
IA: Wrote the manuscript
SH: Collected the data
ZR: Designed the survey, analyzed the data and corrected/edited the final copy of article
REFERENCES
- World Health Organization. 2014. Trends in maternal mortality: 1990 to 2013. Estimates by WHO, UNICEF, UNFPA, The World Bank and the United Nations Population Division. WHO Geneva 2014
- Demographic and Health Survey 2006–07. Islamabad and Calverton, MA: National Institute of Population Studies and Macro International; 2008. Available at; https://dhsprogram.com/pubs/pdf/FR200/FR200.pdf.
- Obstetric Anaesthetists’ Association, Association of Anaesthetists of Great Britain & Ireland. OAA/AAGBI guidelines for obstetric anaesthetic services 2013. Available at; http://www.oaa-anaes.ac.uk/content.asp?ContentID=580DOI http://dx.doi.org/10.xx36/g.OAS2.2013
- American Society of Anesthesiologists: Practice Guidelines for Obstetric Anesthesia-An Updated Report by the American Society of Anesthesiologists Task Force on Obstetric Anesthesia and the Society for Obstetric Anesthesia and Perinatology. Anesthesiology 2016; 124:00-00 [PubMed] [Free full text] doi: 10.1097/ALN.0000000000000935.
- Mushambi MC, Kinsella SM, Popat M, Swales H,Ramaswamy KK, Winton AL,et al. Obstetric Anaesthetists’ Association and Difficult Airway Society guidelines for the management of difficult and failed tracheal intubation in obstetrics. Anaesthesia 2015;70:1286-1306 [PubMed] [Free full text] doi: 10.1111/anae.13260.
- Royal College of Obstetricians and Gynaecologists. Postpartum Haemorrhage, Prevention and Management (Green-top Guideline No. 52). May 2009 Minor revisions November 2009 and April 2011. Available at https://www.rcog.org.uk/en/guidelines-research-services/guidelines/gtg52/
- McGarrity L, O’Connor R, Young S. A national survey of obstetric anaesthesia guidelines in the UK. Int J Obstet Anesth 2008;17:322–328. [PubMed] [Free full text] doi:10.1016/j.ijoa.2008.04.006
- Reynolds, F. and Seed, P. T. Anaesthesia for Cesarean section and neonatal acid-base status: a meta-analysis. Anaesthesia 2005;60:636–653 [PubMed] [Free full text] DOI:
- 1111/j.1365-2044.2005.04223.x
- Mercier FJ, Bonnet MP, De la Dorie A, Moufouki M, Banu F, Hanaf A, et al. Spinal anaesthesia for caesarean section: fluid loading, vasopressors and hypotension. Ann Fr Anesth Reanim. 2007;26:688–693 [PubMed]
- Mirmansouri A, Farzi F, Raoufi A, Zahiri Sorouri Z, Mortazavi Najafabadi F. Epinephrine; a vasoconstrictor or a uterine relaxant? A case series. Professional Med J 2016;23 (4):504-508 [Free full text]
- Ngan Kee WD, Lee SWY, Ng FF, et al. Randomized evaluative study of phenylephrine or norepinephrine for maintenance of blood pressure during spinal anaesthesia for caesarean delivery: the RESPOND study. International Journal of Obstetric Anesthesia2014;23 (Suppl 1): S10. https://doi.org/10.1016/j.ijoa.2017.03.004
- Association of Anaesthetists of Great Britain and Ireland, Obstetric Anaesthetists’ Association; Regional Anaesthesia UK; Association of Paediatric Anaesthetistsof Great Britain and Ireland, Campbell JP, Plaat F, et al. Safety guideline: skin antisepsis for central neuraxial blockade. Anaesthesia. 2014 Nov;69(11):1279-86. [PubMed] [Free full text] doi: 10.1111/anae.12844
- Yentis SM. Height of confusion: assessing regional blocks before caesarean section. Int J Obstet Anesth 2006; 15: 2–6 [PubMed] DOI: 1016/j.ijoa.2005.06.010
- Husain T, Liu YM, Fernando R, Nagaratnam V, Sodhi M, Tamilselvan P, et al. How UK obstetric anaesthetists assess neuraxial anaesthesia for caesarean delivery: national surveys of practice conducted in 2004 and 2010. Int J Obstet Anesth 2013 Nov;22:298–302 [PubMed] doi:10.1016/j.ijoa.2013.
- Russell IF. At caesarean section under regional anaesthesia, it is essential to test sensory block with light touch before allowing surgery to start. Int J Obstet Anesth 2006; 15: 294–7 [PubMed] DOI: http://dx.doi.org/10.1016/j.ijoa.2006.06.006
- Russell IF. A comparison of cold, pinprick and touch for assessing the level of spinal block at caesarean section. Int J Obstet Anesth 2004; 13: 146–52 [PubMed] DOI: http://dx.doi.org/10.1016/j.ijoa.2003.12.007
- David H. Chestnut, Cynthia A Wong, Lawrence C Tsen, Warwick D NganKee, Yaakov Beilin, Jill Mhyre (Rd). Chestnut’s Obstetric Anesthesia: Principles and Practice. Philadelphia: Elsevier Saunders, 2014, 721-722



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube