
Kayo Tsugita, Yuka Matsuki, Tsuyoshi Murakami, Maki Mizogami, Kenji Shigemi
Department of Anesthesiology and Reanimatology, Faculty of Medical Sciences, University of Fukui, (Japan)
Correspondence: Yuka Matsuki, Department of Anesthesiology and Reanimatology, Faculty of Medicine Sciences, University of Fukui, 23-3 Eiheijicho, Yoshidagun, Fukui 910-1193, (Japan); Tel: +81-776-61-8391; Fax: +81-776-61-8116; E-mail: ymatsuki@u-fukui.ac.jp
ABSTRACT
Purpose: Alkalinization of local anesthetics to enhance their efficacy is controversial in peripheral nerve block. To define the efficacy of alkalinized mepivacaine 1% for supraclavicular brachial plexus block, we verified the onset and duration of sensory block using an ultrasound-guided technique.
Methodology: A randomized, double-blinded, controlled, prospective trial was conducted at our hospital after ethical committee approval and informed consents. Twenty patients, 47 – 82 years old and ASA physical status 3, scheduled for vascular access surgery, were randomly divided into Group M (n = 10), receiving 20 ml of mepivacaine 1% alone for nerve block, and Group MSB (n = 10), receiving mepivacaine 1% with sodium bicarbonate for nerve block. Supraclavicular brachial plexus block was performed with a 22-gauge, 50 mm insulated peripheral block needle, peripheral nerve stimulator and ultrasound imaging. Needle placement was confirmed at 0.5 mA, and the drugs were injected. Time to onset of sensory block and duration of sensory block were recorded. Data were statistically analyzed with the t test and Fisher’s exact test, as appropriate, using SPSS Statistics version 22.0 software (SPSS, Chicago, IL). Values of p < 0.05 were considered significant.
Results: Time to onset of sensory block was 9.5 ± 5.5 min in Group M and 7.8 ± 3.4 min in Group MSB, showing no significant difference. Likewise, no difference in duration of sensory block was observed between groups; 257.3 ± 198.0 min vs. 197.3 ± 90.6 min in Group M and Group MSB respectively.
Conclusions: Alkalinization of mepivacaine does not provide faster onset or longer duration of ultrasound-guided supraclavicular brachial plexus block.
Key words: Alkalinization; Local anesthetic; Ultrasound-guided; Supraclavicular brachial plexus block
Citations: Tsugita K, Matsuki Y, Murakami T, Mizogami M, Shigemi K. A randomized controlled trial to verify the efficacy of alkalinized local anesthetics in ultrasound-guided supraclavicular brachial plexus block. Anaesth Pain & Intensive Care 2017;21(3):301-305
Received – 26 Jun 2017; Reviewed – 14 Jul 2017; Corrected & Accepted – 16 Jul 2017
INTRODUCTION
Use of peripheral nerve blocks, with or without general anesthesia, has recently increased for peri- and postoperative pain relief. While this provides superior pain control and decreased side effects compared with the use of opioids,1 the relatively slow onset and short duration of anesthesia represent the limiting factors. Alkalinization of local anesthetics have been used in peripheral nerve blocks with the assumption that it will hasten the onset and prolong the anesthetic effects of these drugs,2 but some investigators failed to find any improvement.3 Similarly conflicting results have been seen for brachial plexus block using alkalinized local anesthetic solution.4
Success of the brachial plexus block depends greatly on proper technique of nerve localization, accurate needle placement and the local anesthetic solution used. Blind technique, which relies on surface landmarks before needle insertion and elicitation of paresthesia or nerve-stimulated muscle contraction after needle insertion, have often been used in previous studies. These techniques always carry an inherent rate of block failure, particularly with the supraclavicular approach, because this approach directs the needle toward the first rib close to the pleura and provides a more extensive block than the axillary block, as musculocutaneous and axillary nerves are also blocked with it. To improve success rate, ultrasound technology allows the needle tip to be placed near the targeted nerve and facilitates precise monitoring of the spread of local anesthetics5). In addition, ultrasound guidance enables the physician to replace the needle in the case of maldistribution of the local anesthetic in real time. We, therefore, aimed to verify the effects of alkalinization of mepivacaine 1% on supraclavicular brachial plexus block using an ultrasound guided technique.
METHODOLOGY
The study was approved by the hospital ethics committee and was registered with University hospital Medical Information Network Clinical Trial Registry (UMIN000013121). After obtaining informed consent from patients, 20 adult patients between 47 and 82 years old and ASA physical status 3, scheduled for vascular access surgery, were included in this study. A randomized, double-blinded, controlled, prospective trial design was used. Cases, in which supraclavicular brachial plexus block was contraindicated, including allergy against local anesthetics, presence of infection, or who were uncooperative or who refused to participate in the study, were excluded from the study. Patients were randomly divided into two groups: Group M (n = 10) receiving 20 ml of mepivacaine 1% for nerve block; and Group MSB (n = 10) receiving 19.5 ml of mepivacaine 1% + 0.5 ml of sodium bicarbonate 8.4% for nerve block. After applying routine monitors and insertion of a peripheral intravenous cannula, the brachial plexus and its spatial relationship to surrounding structures were pre-scanned using a 10 MHz linear transducer and a standard diagnostic high resolution GE LOGIQ-e ultrasound machine (GE Healthcare, Milwaukee, WI). After disinfecting the skin and infiltrating lidocaine 1%, supraclavicular brachial plexus block was performed by the author using a 22-gauge, 50 mm insulated peripheral block needle (Stimuplex®, A50; B Braun, Melsungen, Germany) guided by a peripheral nerve stimulator (Stimuplex®, DIG; B Braun) and ultrasound imaging. Needle movement was observed in real time. Once the needle reached the brachial plexus cluster, a nerve stimulator was turned on, starting from 1.0 mA and increasing up to 1.5 mA to elicit muscle twitch. We confirmed a lack of muscle twitch under 0.5-mA stimulation. The site of muscle twitch and presence of paresthesia were checked and recorded. Thereafter, 20 ml of local anesthetic solution was injected incrementally over 3–5 min and spread of the agent was observed in real time. If the local anesthetic solution did not spread around the brachial plexus, the needle was repositioned.
The blinded observer added the sodium bicarbonate directly to the mepivacaine solution and measured the pH using a pH meter (Twin pH meter®, B-212; HORIBA, Kyoto, Japan) just before injection. Time to onset of sensory block after injection was determined using the pinprick test on the skin incision area every 1 min. Established block was defined as complete loss of the ability to sense pinprick. Duration of sensory block was also recorded as the interval between complete loss of sensation and onset of pain or disappearance of numbness. If intraoperative analgesia was needed, we directly injected 1% lidocaine into surgical site. Intra- and postoperative nausea and numbness, and other side effects were recorded. Postoperative pain was evaluated by visual analog scale (VAS) the following morning and oral acetaminophen was used for adjunctive treatment.
Results are expressed as mean ± standard deviation. Data were statistically analyzed with the t test and Fisher’s exact test, as appropriate, using SPSS Statistics version 22.0 software (SPSS, Chicago, IL). Values of p < 0.05 were considered significant.
RESULTS
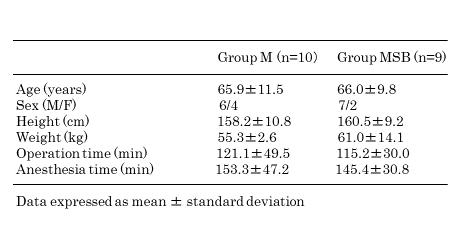
Of the 20 patients initially enrolled, one was withdrawn from the study following randomization because insufficient nerve block was achieved. No significant difference was seen between groups in terms of demographic characteristics, duration of surgery or anesthesia (Table 1).
Table 1: Demographic characteristics, operation time and anesthesia time
The pH of solutions differed significantly between groups, at 6.17 ± 0.15 in Group M and 6.92 ± 0.15 in Group MSB. Onset of sensory block was 9.5 ± 5.5 min in Group M and 7.8 ± 3.4 min in Group MSB, with no significant difference between groups (Figure 1).
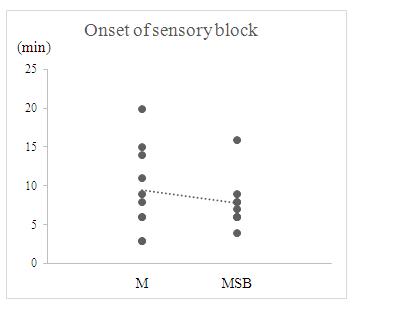
Figure 1: Effect of each local anesthetic on onset of sensory block. No difference is evident between mepivacaine and alkalinized mepivacaine
Duration of sensory block did not differ significantly between Group M (257.3 ± 198.0 min) and Group MSB (197.3 ± 90.6 min) (Figure 2).
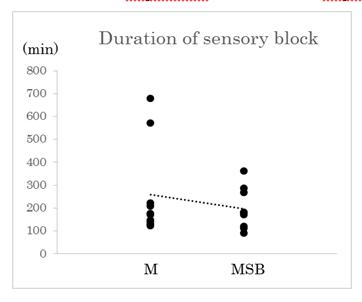
Figure 2: Effect of each local anesthetic on duration of sensory block. No difference is evident between mepivacaine and alkalinized mepivacaine
No significant differences were found among groups with respect to additional intraoperative analgesia, postoperative VAS score or oral acetaminophen. Numbness over the thenar eminence and hemorrhage related re-operation were noted as postoperative complications in Group M.
DISCUSSION
Our results indicate that alkalinization of local anesthetic does not hasten the onset time or elongate anesthetic effects, as verified by supraclavicular brachial plexus block using an ultrasound guided technique.
Clinically used local anesthetics are structurally tertiary amines with aromatic rings, and thus exist as charged and uncharged molecules with the relative amounts depending on the pH and pKa of the medium. While both species are relevant to pharmacological activities, local anesthetics diffuse in uncharged form through nerve sheaths and penetrate cell membranes to reach the cytoplasmic binding sites of voltage-gated sodium channels. Adding alkalinized substances to local anesthetic solutions is generally believed to either shorten the onset of regional anesthesia or prolong the anesthetic effect by increasing the proportion of the uncharged form and facilitating penetration to the nerve cell membrane.6 The pKa of mepivacaine is 7.72 at 36 ºC, as determined by spectrophotometric methods.7 When applying this value to the Henderson-Hasselbalch equation {log[uncharged form]/[charged form] = pH – pKa}, the percentage of uncharged mepivacaine in the total concentration is calculated as follows: 2.7% at pH 6.17; and 13.6% at pH 6.92. Even though the change in pH after alkalinization may have been large enough in the study, this theoretical increase of uncharged mepivacaine did not equate to a relative increase in anesthetic potency.
Previous studies using alkalinized local anesthetics in brachial plexus block have yielded conflicting results. Alkalinization of mepivacaine (pH 7.25) in axillary block reportedly decreased the time to onset of motor and sensory analgesia as compared with plain solution (pH 6.0).8 However, Berman et al. found that alkalinization of mepivacaine did not hasten the time to onset of axillary block as measured by a sensory and motor scoring system.9 Unfortunately, the standard approaches used in those previous studies were “blind” techniques using a nerve stimulator. Recently, improvements in ultrasound technology have allowed placement of the needle tip near the targeted nerve and precise monitoring of the spread of local anesthetics. A supraclavicular approach offers potential advantages over other approaches and the compactness of the brachial plexus in this location facilitates rapid onset and complete nerve block. The ultrasound-guided supraclavicular approach reportedly provides faster onset and reduced puncture times compared to the conventional approach with a nerve stimulator alone.10 The present study was, therefore, conducted using both ultrasound imaging and electrical nerve stimulation to verify the efficacy of alkalinized local anesthetic. The results confirmed that ultrasound guidance for supraclavicular brachial plexus block was useful for accurate nerve localization and to minimize the number of needle attempts without serious complications.
Although we found that alkalinization exerted no significant effect on the development of analgesia, several factors that may have contributed to these contradictory results. As one theoretical explanation for these results, positively charged local anesthetics may likewise penetrate into cell membranes by ion-pairing with anionic membranes constituting lipids such as counter-ionic phosphatidylserine and cardiolipin.11 While lipid bilayers of cell membrane represent a barrier to charged or highly polar molecules, membrane penetration of cationic peptides is mediated by negatively charged phospholipids through the formation of ion pairs.12 An alternative relevant factor that can be considered includes the buffering capacity of the tissue, which may rapidly decrease the pH and uncharged molecules,13 or metabolic acidosis associated with chronic renal failure, which might affect the time to onset and duration of effect of anesthesia.14
LIMITATIONS
Several limitations were present in this study, including the small sample size. Further studies are required to clarify the potential benefits of alkalinization of local anesthetics in motor nerve block, if any.
CONCLUSION
We conclude that alkalinization of mepivacaine does not provides faster onset or longer duration of sensory block in ultrasound-guided supraclavicular brachial plexus block.
Conflicts of interest (Disclosures): The authors declare no conflicts of interest in this study.
Author contribution: All authors took part in the conduct of study, data collection, literature search and manuscript preparation
REFERENCES
- Hadzic A, Ariss J, Kerimoglu B, Karaca PE, Yufa M, Claudio RE, Vloka JD, et al. A comparison of infraclavicular nerve block versus general anesthesia for hand and wrist day-case surgeries. Anesthesiology 2004;101:127–132. [PubMed] [Free full text]
- Galindo A. pH-adjusted local anesthetics: clinical experience. Reg Anesth 1983;8:35–6.
- Gaggero G, Meyer O, Van Gessel E, Rifat K. Alkalinization of lidocaine 2% does not influence the quality of epidural anaesthesia for elective caesarian section. Can J Anaesth 1995;42:1080. [Free full text] org/10.1007/BF03015092
- Mehta R, Verma DD, Gupta V, Gurwara AK. To study the effect of alkalinization of lignocaine hydrochloride on brachial plexus block. Indian J Anaesth 2003;47:283–6.
- Ting PL, Sivagnanaratnam V. Ultrasonographic study of the spread of local anaesthetic during axillary brachial plexus block. Br J Anaesth 1989;63:326–9. [PubMed]
- Turan A, Memiş D, Karamanlioğlu B, Güler T, Pamukçu Z. Intravenous regional anesthesia using lidocaine and magnesium. Anesth Analg 2005;100:1189–92. [PubMed] [Free full text] DOI:10.1213/01.ANE.0000145062.39112.C5
- Strichartz GR, Sanchez V, Arthur GR, Chafetz R, Martin D. Fundamental properties of local anesthetics. II. Measured octanol: buffer partition coefficients and pKa values of clinically used drugs. Anesth Analg 1990;71:158–70. [PubMed]
- Büttner J, Klose R. Alkalinization of mepivacaine for axillary plexus anesthesia using a catheter. Reg Anesth 1991;14:17–24. [PubMed]
- Berman S, Rosenquist RW, Finucane BT. Alkalinization of mepivacaine for axillary brachial plexus block. Can J Anaesth 1988;35S93–5.
- Liu GY, Chen ZQ, Jia HY, Dai ZG, Zhang XJ. The technique comparison of brachial plexus blocks by ultrasound guided with blocks by nerve stimulator guided. Int J Clin Exp Med 2015;8:16699–703. eCollection 2015.. [PubMed] [Free full text]
- Tsuchiya H, Mizogami M. Membrane interactivity of charged local anesthetic derivative and stereoselectivity in membrane interaction of local anesthetic enantiomers. Local Reg Anesth 2008;1:1–9. [PubMed] [Free full text]
- Esbjörner EK, Lincoln P, Nordén B. Counterion-mediated membrane penetration: cationic cell-penetrating peptides overcome Born energy barrier by ion-pairing with phospholipids. Biochim Biophys Acta 2007;1768:1550–8. [PubMed] [Free full text] DOI: 10.1016/j.bbamem.2007.03.004
- Wennberg E, Haljamäe H, Edwall G, Dhuner KG. Effects of commercial (pH approximately 3.5) and freshly prepared (pH approximately 6.5) lidocaine-adrenaline solutions on tissue pH. Acta Anaesth Scand 1982;26:524–7. [PubMed] DOI: 10.1111/j.1399-6576.1982.tb01812.x
- Al-mustafa MM, Massad I, Alsmady M, Al-qudah A, Alghanem S. The effect of low serum bicarbonate values on the onset of action of local anesthesia with vertical infraclavicular brachial plexus block in patients with end-stage renal failure. Saudi J Kidney Dis Transpl 2010;21494–500. [PubMed] [Free full text]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube