
Khushali R. Tilvawala1, Parul R. Panchotiya2
1Resident; 2Professor
Department of Anesthesiology, NHL Municipal Medical College, Ahmedabad, Gujarat (India)
Correspondence: Dr. Khushali R. Tilvawala, Department of Anesthesiology, NHL Municipal Medical College, Ahmedabad, Gujarat (India); E-mail: drpiyushpujara@gmail.com
ABSTRACT
Background and objective: Laparoscopic techniques have rapidly increased in popularity because of associated benefits. Although the most commonly performed surgery still remains laparoscopic cholecystectomy, many other surgical procedures have been included in the list. Our aim of this study was to compare the hemodynamic changes and emergence characteristics during maintenance of anesthesia either with sevoflurane or propofol infusion in laparoscopic surgeries.
Methodology: Fifty patients of ASA physical status I or II, aged between 18-60 years, of either sex, scheduled for various elective laparoscopic surgeries of around 2 hours duration under general anesthesia were selected for this study. All the patients were given premedications; inj glycopyrrolate 0.004 mg/kg, inj ondansetron 0.08 mg/kg and inj fentanyl 1.0 mg/kg IV. Induction was done with inj thiopentone sodium 5 mg/kg and inj succinylcholine 2 mg/kg, followed by intubation. Muscle relaxation was achieved with inj vecuronium 0.1 mg/kg loading dose followed by 0.02 mg/kg IV 20-45min post initial PRN. Patients were then randomly divided into 2 groups: Group S (Sevoflurane group) was maintained on sevoflurane 1-1.5% + O2:N2O (50:50). Group P received inj propofol 1 mg/kg bolus followed by 100-300 µg/kg/min infusion + O2:N2O (50:50). Mean arterial pressure, mean heart rate, and emergence characteristics were recorded. All the quantitative data were analyzed using unpaired T test.
Results: Mean heart rate after pneumoperitonium was 93.32 ± 6.29 vs. 91.00 ± 4.46 per min for Group S and Group P respectively. Mean blood pressure after pneumoperitonium for Group S was 101.72 ± 6.32 and for Group P was 98.00 ± 7.69 mmHg. There was no significant difference in EtCO2, and SpO2 was maintained at 99-100% throughout the surgery in both groups. Time for spontaneous respiration, time to spontaneous eye opening, following verbal command and telling own name by the patient were significantly lower in Group S than Group P.
Conclusion: We conclude that maintenance of general anesthesia with sevoflurane is associated with faster emergence from anesthesia when compared with propofol, while propofol is associated with lower incidence of PONV in laparoscopic surgical procedures.
Key words: Propofol; Laparoscopic surgery; Emergence phenomenon; Nausea; Vomiting, Postoperative
Citation: A randomized, comparative study of propofol infusion and sevoflurane as the sole maintenance agent in laparoscopic surgery. Anaesth Pain & Intensive Care 2017;21(2):154-158
Received: 19 Jan 2017, Reviewed: 17 Apr 2017, Corrected: 19 Apr 2017, Accepted: 21 Apr 2017
INTRODUCTION
Laparoscopic techniques have rapidly increased in popularity because of associated benefits. Anesthesia for laparoscopic surgery has various physiological changes associated with it which may be related to increased intra-abdominal pressure due to pneumoperitoneum, position of the patient and CO2 insufflation and its absorption leading to hypercarbia.1
Propofol an intravenous anesthetic characterized by rapid metabolic clearance has been used extensively in day care anesthesia for smooth maintenance and rapid recovery with lesser post-operative complications (nausea, vomiting and respiratory depression). Its specific pharmacodynamic characteristics e.g., decrease in heart rate and blood pressure, are particularly useful for physiological changes of pneumoperitoneum like tachycardia and hypertension. The brevity of action and rapid recovery with propofol has led to extensive usage of this agent for maintenance of anesthesia along with oxygen and nitrous oxide.2,3
Newly introduced volatile anesthetic, sevoflurane also allows faster recovery from anesthesia4 because of its favorable pharmacokinetic properties.
The present study has been carried out with an objective to compare sevoflurane with propofol infusion for anesthesia maintenance with respect to hemodynamic characteristics and recovery profile in laparoscopic surgeries.
METHODOLOGY
Fifty patients of ASA physical status I or II aged between 18-60 years of either sex were selected for this study who were scheduled for various elective laparoscopic surgeries of about 2 hours duration under general anesthesia. Informed written consent was obtained from each patient.
All the patients were premedicated; inj glycopyrrolate (0.004 mg/kg), inj ondansetron (0.08 mg/kg) and inj fentanyl (1.0 mg/kg) IV. After preoxygenation, induction was done with inj thiopentone sodium (5 mg/kg). In both of the groups, endotracheal intubation with appropriate number of cuffed endotracheal tube was facilitated with inj succinylcholine (2 mg/kg). Inj vecuronium was given in a loading dose of 0.1 mg/kg followed by 0.02 mg/kg 35-40 min after.
Then the patients were randomly assigned to Group S to receive sevoflurane-N2O-O2 anesthesia for maintenance, and Group P to receive propofol- N2O-O2 for maintenance of general anesthesia in laparoscopic surgery.
Patients of Group P were given inj propofol 1 mg/kg bolus followed by 100-300 µg/kg/min infusion. During maintenance, anesthetic concentrations were adjusted so that the hemodynamic parameters (MAP and HR) are maintained within 15% of baseline values to ensure adequate depth of surgical anesthesia.
The parameters recorded were, heart rate, noninvasive blood pressure, arterial oxygen saturation (SpO2) and end tidal CO2 (EtCO2) at the start of anesthesia (baseline parameters). Then all the parameters were recorded after induction, soon after intubation, then every minute for 5 min and then soon after creation of pneumoperitoneum, 10 min after pneumoperitoneum then every 5 min till half an hour and then every 15 min till the end of surgery, then at the removal of trocar, at extubation and 10 min after extubation. Administration of anesthetic agent was discontinued at the removal of the trocar, reversal of neuromuscular blockade was done using inj glycopyrrolate (0.008 mg/kg) and inj neostigmine (0.05 mg/kg). Endotracheal extubation was done after adequate recovery.
Following parameters were recorded during recovery: time of spontaneous respiration; time of spontaneous eye opening; time of following verbal command and time to be able to tell own name.
Vital signs were recorded for next 10 min after extubation. Patients were watched for any complication or untoward reaction e.g., nausea and vomiting, respiratory depression, involuntary movements or excitement and general discomfort for 1 hour post operatively. Total maintenance anesthesia time (from intubation to removal of trocar) and surgery time (from incision to closure of incision) were recorded.
Statistical analysis:
The data was coded and entered into Microsoft Excel spreadsheet. Analysis was done using SPSS version 15 (SPSS Inc. Chicago, IL, USA) Windows software program. Descriptive statistics included computation of percentages. For all tests, confidence level and level of significance were set at 95% and 5% respectively. All the quantitative data were analyzed using unpaired T test. The results were expressed as mean ± SD.
RESULTS
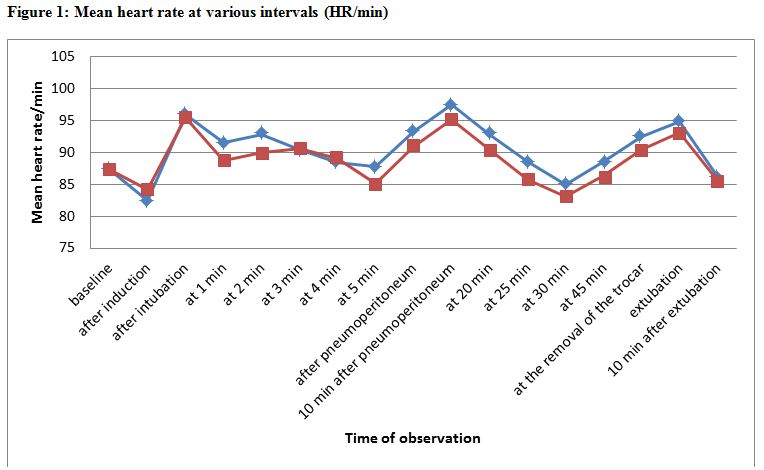
Mean heart rates at various time intervals in the groups are given in Table 1 and Figure 1.
Table 1: Mean heart rate at various intervals
| Time | Group S | Group P |
| Baseline | 87.24 ± 5.79 | 87.32 ± 4.62 |
| After induction | 82.44 ± 5.75 | 84.16 ± 6.55 |
| After intubation | 95.88 ± 5.82 | 95.48 ± 5.96 |
| At 1 min. | 91.48 ± 6.04 | 88.72 ± 4.27 |
| At 2 min. | 92.84 ± 5.93 | 90.04 ± 5.03 |
| At 3 min. | 90.40 ± 5.98 | 90.60 ± 4.20 |
| At 4 min. | 88.44 ± 6.26 | 89.12 ± 4.84 |
| At 5 min. | 87.72 ± 6.48 | 85.12 ± 4.59 |
| After pneumoperitoneum | 93.32 ± 6.29 | 91.00 ± 4.46 |
| 10 min after pneumoperitoneum | 97.48 ± 5.73 | 95.2 ± 4.30 |
| At 20 min. | 92.84 ± 5.84 | 90.48 ± 4.91 |
| At 25 min. | 88.60 ± 5.35 | 85.80 ± 4.27 |
| At 30 min. | 85.00 ± 5.07 | 83.04 ± 3.95 |
| At 45 min. | 88.56 ± 5.21 | 86.36 ± 4.11 |
| At the removal of trocar | 92.52 ± 5.23 | 90.40 ± 5.27 |
| Extubation | 94.88 ± 5.16 | 93.12 ± 5.39 |
| 10 min after extubation | 86.20 ± 5.75 | 85.56 ± 4.61 |
Figure 1: Mean heart rate at various intervals (HR/min)
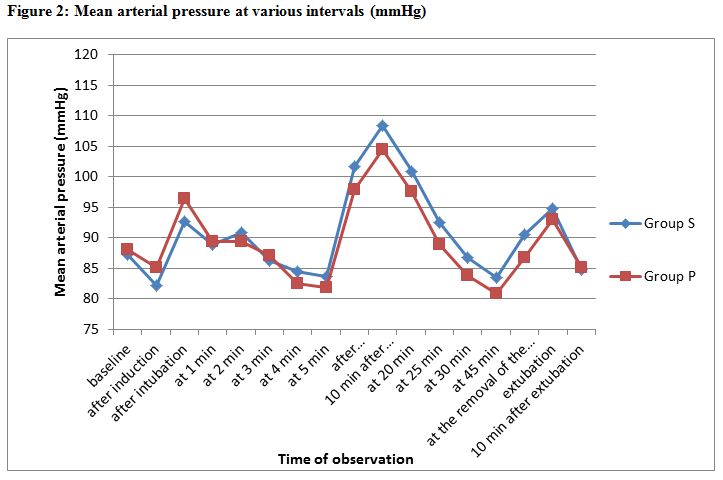
Mean arterial pressures at various time intervals in the groups are given in Table 2 and Figure 2.
Table 2: Mean blood pressure (mmHg) at various intervals
| Time | Group S | Group P |
| Baseline | 87.24 ± 8.32 | 88.12 ± 7.22 |
| After induction | 82.12 ± 9.06 | 88.12 ± 7.49 |
| After intubation | 92.60 ± 6.58 | 96.40 ± 6.92 |
| At 1 min. | 88.96 ± 6.52 | 89.36 ± 6.68 |
| At 2 min. | 90.80 ± 6.29 | 89.40 ± 7.94 |
| At 3 min. | 86.24 ± 7.61 | 87.08 ± 8.09 |
| At 4 min. | 84.40 ± 6.87 | 82.52 ± 6.48 |
| At 5 min. | 83.64 ± 5.69 | 81.88 ± 6.89 |
| After pneumoperitoneum | 101.72 ± 6.32 | 98.00 ± 7.69 |
| 10 min after pneumoperitoneum | 108.44 ± 7.32 | 104.48 ± 6.84 |
| At 20 min. | 100.96 ± 7.83 | 97.52 ± 7.57 |
| At 25 min. | 92.56 ± 7.56 | 88.84 ± 7.89 |
| At 30 min. | 86.72 ± 7.85 | 83.80 ± 7.33 |
| At 45 min. | 83.40 ± 7.75 | 80.88 ± 6.50 |
| At the removal of trocar | 90.52 ± 8.23 | 86.80 ± 6.56 |
| Extubation | 94.80 ± 7.92 | 92.96 ± 6.52 |
| 10 min after extubation | 84.80 ± 7.08 | 85.12 ± 5.66 |
Figure 2: Mean arterial pressure at various intervals (mmHg)
There was no significant difference in EtCO2 and SpO2 was maintained 99-100% throughout the surgery in both groups.
Table 3: Characteristics at emergence (Mean ± SD)
| Emergence characteristics | Mean emergence time (min) | |
| Group S | Group P | |
| Spontaneous respiration | 2.80 ± 0.70 | 3.36 ± 0.74 |
| Spontaneous eye opening | 4.36 ± 0.86 | 5.08 ± 0.74 |
| Following verbal command | 5.96 ± 0.89 | 6.56 ± 0.89 |
| Speaking name | 8.04 ± 0.80 | 8.84 ± 0.92 |
Time for spontaneous respiration, spontaneous eye opening, following verbal command and speaking name by the patient were significantly lower in Group S than Group P (Table 3).
Regarding postoperative complications, 8% patients in Group S had vomiting at the end of procedure compared to 4% patients in Group P. There were no significant hemodynamic complications noted postoperatively in both groups.
DISCUSSION
Laparoscopy has revolutionized surgical procedure because of the important advantages it offers. Maintenance of anesthesia in laparoscopic surgeries is particularly challenging because of physiological changes associated with pneumoperitoneum.
Both propofol and sevoflurane have smooth and rapid onset of action. Both can be used for induction and maintenance of general anesthesia in laparoscopic surgeries with highly satisfying anesthetic conditions.
In our study sample the intraoperative hemodynamic parameters were within acceptable range in both the groups. As seen in Table 1 mean heart rates increase after intubation because of sympathetic stimulation in both the groups and returns to baseline at around 4-5 min. In both the groups, after induction of pneumoperitoneum there was rise in HR due to physiological changes associated with it.7 Though this increase was less in Group P, the difference was not significant between Group S and Group P. Propofol is known to cause a reduction in BP and HR in humans, and inhibition of sympathetic nerve activity is believed as one major mechanism underlying the propofol induced hemodynamic depression.8,9
With sevoflurane, heart rate remained almost stable throughout the surgery. The inspired concentration of sevoflurane was adjusted as necessary to maintain adequate depth of anesthesia (ranging between 1-1.5%). There was no significant episode of bradycardia or tachycardia during surgery.
Mean blood pressure, though better maintained during sevoflurane maintenance compared with propofol, this difference was not statistically significant. Propofol decreases systemic blood pressure due to decrease in cardiac output, stroke volume index and systemic vascular resistance. This action is because of relaxation of vascular smooth muscles produced by inhibition of sympathetic vasoconstrictor nerve activity. The reports state that during maintenance of anesthesia with propofol infusion there is 20-30% reduction in systolic blood pressure from the pre induction value.2,10 Increasing the infusion rate of propofol produces a slightly greater decrease in arterial blood pressure.10
Jellish et al.4 compared the effects of sevoflurane and propofol for induction and maintenance of anesthesia in adult patients. They demonstrated that sevoflurane compares favorably with propofol for both ease of induction and emergence from anesthesia.
There was no significant variation in EtCO2 and SpO2 during maintenance of anesthesia.
Emergence time from discontinuation of primary maintenance anesthesia to spontaneous respiration, spontaneous eye opening, following verbal command and speaking name by the patient were significantly lower in Group S than Group P. Larsen et al.(11) found propofol group had better early recovery profile with better cognitive function in intermediate recovery phase as compared to sevoflurane group.
Wondell C et al.12 reported that following general anesthesia, extubation is earlier in patients who received sevoflurane for maintenance than those maintained with propofol infusion. Patients regained cognitive function much earlier after sevoflurane anesthesia.
Samantaray et al.13 concluded that maintenance of anesthesia with sevoflurane is associated with a faster recovery than propofol.
Two patients (8% of total patients) of Group S had vomiting while only one patient (4% of total patients) of Group P had vomiting within 10 min of extubation. Possibly intrinsic anti emetic property of propofol15 is responsible for less incidence of post-operative nausea and vomiting in Group P.
Laparoscopic surgery is associated with greater incidence of PONV1 and sevoflurane like any other inhalational anesthetic is associated with post-operative nausea and vomiting.15 This finding was similar in many previous studies.13,7,6 SpO2 was found within normal limits throughout the surgery.
LIMITATIONS
The limitation of our study was that BIS or other monitoring device of anesthetic depth was not available, so we had to rely on standard clinical indicators (i.e. maintenance of hemodynamic stability) to titrate the maintenance anesthetics as mentioned in methods.
CONCLUSION
In conclusion, sevoflurane and propofol are comparable for maintenance of anesthesia in laparoscopic surgery. Maintenance with sevoflurane is associated with faster emergence from anesthesia while that with propofol is associated with lower incidence of PONV.
Conflict of interest: None declared.
Sources of funding: Nil.
Authors’ contribution: Both authors tool part in the concept, conduct of the study data collection and manuscript preparation.
REFERENCES
- Sood J, Kumra VP. Anaesthesia for laparoscopic surgery. Indian J Surg 2003; 65:232-40.
- Claeys MA, Gepts E, Camu F. hemodynamic changes in anaesthesia induced and maintained with propofol. Br J Anesth. 1983 Jan:60(1):3-9 .[PubMed]
- MS Khanna, V Sarha. A comparative evaluation of 1% and 2% propofol as sole intravenous anesthetic agent for short surgical procedure. J Anesth Clin. Pharmacol 2002;18(1) 87-90.
- Jellish WS, Lien CA, Fontenel HJ, Hall R.. The comparative effects of sevoflurane versus propofol in the induction and maintenance of anesthesia in adult patients. Anesth Analg. 1996 Mar;82(3):479-85. .[PubMed]
- Ozkose Z, Eecan B, Unal Y, Yardeem S, Kaymaz M, Dogulu F, et al.. Inhalational versus total intravenous anaesthesia for lumbar disc herniation: comparison of hemodynamic effects, recovery characteristics and cost. J Neuro Surg Anestehsiol. 2001 Oct;13(4):296-302. [PubMed]
- Singh SK, Kumar A, Mahajan R, Katyal S, Mann S. Comparison of recovery profile for propofol and sevoflurane anesthesia in cases of open cholecystectomy. Anaesth Essays Res. 2013 Sep-Dec;7(3):386-9. doi: 10.4103/0259-1162.123259. [PubMed] [Free full text]
- Gupta A, Stierer T, Zuckerman R, Sakima N, Parker D, Fleisher LA. Comparison of recovery profile after ambulatory anaesthesia with propofol, isoflurane, sevoflurane and desflurane: a systemic review. Anesth Analg. 2004 Mar;98(3):632-41. [PubMed]
- Ebert TJ, Muzi M, Berens R, Goff D, Kampine JP. Sympathetic responses to induction of anesthesia in humans with propofol or etomidate. Anesthesiology. 1992 May;76(5):725–33. [PubMed]
- Robinson BJ, Ebert TJ, O’Brien TJ, Colinco MD, Muzi M. Mechanisms whereby propofol mediates peripheral vasodilation in humans. Sympathoinhibition or direct vascular relaxation? Anesthesiology. 1997 Jan;86(1):64–72. [PubMed] [Free full text]
- Coats DP, Monk Cr, Prys Roberts C, Turtle M. Hemodynamic effects of the infusion of the emulsion formulation of propofol during nitrous oxide anesthesia in humans. Anesth Analg. 1987 Jan;66(1):64-70. [PubMed]
- Larsen B, Seitz A, Larsen R. Recovery of cognitive function after remifentanyl-propofol anaesthesia: a comparison with desflurane and sevoflurane anesthesia. Anaesth Analg. 2000 Jan;90(1):168-74. [PubMed]
- Wandel C, Neff S, Böhrer H, Browne A, Motsch J, Martin E. Recovery characteristics following anaesthesia with sevoflurane or propofol in adults undergoing out-patient surgery. Eur J Clin Pharmacol. 1995;48:185–8. [PubMed]
- Samantaray A, Rao M. Comparative effects of propofol infusion versus sevoflurane for maintenance of anesthesia for spine surgery. Int J Anesth. 2006;11(2). [Free full text]
- Singh SK, Kumar A, Mahajan R, Katyal S, Mann S. Comparison of recovery profile for propofol and sevoflurane anesthesia in cases of open cholecystectomy. Anaesth Essays Res. 2013 Sep-Dec;7(3):386-9. doi: 10.4103/0259-1162.123259. [PubMed] [Free full text]
- Apfel CC, Kranke P, Katz MH, Goepfert C, Papenfuss T, Rauch S, et al. Volatile anesthetics may be the main cause of early but not delayed postoperative vomiting: a randomized control trial of factorial design. Br J Aneasth. 2002 Jun;88(5):659-68. [PubMed] [Free full text]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube