
Maria Rosaria Spoto, MD1, Paola Zito, MD1, Andrea Forastieri Molinari, MD1,
Giovanni Capretti, MD2, Francesca Gavazzi, MD2, Cristina Ridolfi, MD2,
Stefania Grimaldi, MD1, Samantha Pesce3, Paola Allavena3, Alessandro Zerbi, MD2
1Department of Anesthesiology and Intensive Care
2Pancreatic Surgery Section – Department of Surgery
3Department of Immunology and Inflammation
Humanitas Clinical and Research Center, via Manzoni 56, Rozzano (MI) – (Italy)
Correspondence: Giovanni Capretti, MD, Pancreatic Surgery – Department of Surgery, Humanitas Clinical and Research Center, via Manzoni 56, Rozzano (MI) – (Italy); E-mail: g.l.capretti@gmail.com
ABSTRACT
Introduction: Few data support the use of thoracic epidural analgesia (TEA) in pancreatic surgery. Recent evidence suggested that the use of continuous wound local anesthetic infusion (CWI) could be a reliable and effective procedure in different types of surgeries. The aim of this study was to determine if CWI could be an alternative to TEA in pancreatic surgery.
Methodology: Eighty consecutive patients that received a subcostal incision for pancreatic resection from April 2012 to February 2013 in our institute were randomized into two groups to receive either postoperative TEA or CWI. Patients with contraindications to epidural analgesia or any drugs in the protocol, not able to comply with the protocol or use a PCA device were excluded. Rescue analgesia was provided to all patients via patient-controlled analgesia (PCA) which delivered boluses of morphine. Postoperative pain levels where considered as primary end point, and evaluated with Verbal Numeric Scale (VNS). As secondary end points, we studied consumption of morphine, postoperative complications, length of stay, resumption of complete bowel function, and time to mobilization. Circulating cytokines and chemokines were evaluated in 20 patients to assess the effects on the inflammatory response.
Results: None of the two techniques demonstrated advantages in terms of static and dynamic postoperative pain control (VNS). Median morphine consumption was not significantly different in TEA [12 mg (IQR 9-23)] and in CWI group [15 mg (IQR 10-29)] (p = 0.527). There was no significant difference between the two groups with regards to secondary endpoints. The median length of stay was comparable in CWI and TEA group [10 (IQR 9-16) vs 12 (IQR 8-15,5)] days; (p = 0.481). Similar levels of inflammatory mediators were found. In the TEA group 13% of the patients experienced hypotension; no such cases where observed in CWI group.
Conclusions: Our study failed to demonstrate a superiority of TEA compared to CWI in management of postoperative pain after pancreatic surgery.
Keywords: Epidural analgesia; Local anaesthesia; Postoperative pain; Pancreatectomy
Citation: Spoto MR, Zito P. MolinariAF, Capretti G, Gavazzi F, Ridolfi C, Grimaldi S, Pesce S, Allavena P, Zerbi A. A randomized clinical trial to compare the efficacy of continuous local anesthetic wound infusion with thoracic epidural analgesia in post-operative pain control after pancreatic surgery. Anaesth Pain & Intensive Care 2015;19(4):429-436
INTRODUCTION
Pain management after pancreatic surgery is a fundamental requirement, especially in the contest of an enhanced recovery after surgery protocol. Thoracic epidural analgesia (TEA) has shown a greater efficiency in postoperative pain control than systemic opioids administered by patient controlled analgesia (PCA) during major open abdominal surgery.1 The use of opioids alone as postoperative analgesia may delay functional recovery and prolong the length of stay.2 However, in some clinical circumstances such as coagulopathies, thrombocytopenia and previous spine surgery TEA is contraindicated.2-4 Furthermore, in reported experience, epidural analgesia can fail to achieve satisfactory pain control in up to 25% of patients,3-4 sometimes need to be discontinued due to hypotension and can rarely lead to serious complications.2-4 While multiple studies report favorable outcomes with TEA during major abdominal surgery, there are limited data to support its use in pancreatic surgery, and on the other hand, there are some critical appraisals.5
An alternative and rational approach could be the continuous surgical wound site infusion of local anesthetics (CWI).6 The reduction of parietal and peritoneal nociceptive inputs by use of CWI could also inhibit the visceral component of postoperative pain.7 This may reduce postoperative paralytic ileus8 and chronic post-surgical pain.9 Local anesthetics also possess an anti-inflammatory effect,10 and these may attenuate the release of neuropeptides from peripheral nerve endings and change local wound level of cytokines after tissue injury.11
The aim of our study was to evaluate the superiority of CWI or TEA in control of postoperative pain, reducing the need for IV morphine, and improving functional recovery of patients after pancreatic surgery.
The level of circulating cytokines in the two groups was also assessed to detect if the two techniques exerted a different anti-inflammatory effect.
METHODOLOGY
Data collection and Anesthetic Techniques
Data were collected from 80 consecutive patients who underwent pancreatic surgery at our centre from April 2012 to January 2013 and received either TEA or CWI. It was a randomized, parallel, prospective, open label, controlled clinical trial, approved by the Independent Ethics Committee of Istituto Clinico Humanitas. Randomization was done using numbered sealed envelopes. The randomization sequence was generated with the support of statistics software by a third person not involved in the study, who also prepared the envelopes. All patients were enrolled after signing the informed consent and randomized before the start of surgery. Patients of both sexes, 18 years of age and older, ASA physical status I – III and candidates for pancreatic surgery were eligible to be included. All procedures were performed through subcostal incisions (extended right for pancreaticoduodenectomies, left for distal pancreatectomies).
Exclusion criteria were; a contraindication to epidural analgesia, subjects not being able to comply with the protocol or use a PCA device, preoperative chronic pain syndrome, patients allergic to any drugs used in the protocol or refusal to give informed consent to participate. Before starting anesthesia, both groups of patients received 4 mg of dexamethasone for prophylaxis of postoperative nausea and vomiting (PONV). General anesthesia was induced with propofol 1% (1.5–2.5 mg/kg) and fentanyl (1–3 μg/kg); cisatracurium (0.15 mg/ kg) was used for tracheal intubation. Maintenance was achieved with a balanced technique using sevoflurane and subsequent boluses of cisatracurium. Before induction of anesthesia in the TEA patients, an epidural thoracic catheter (Epidural system 18G/16G catheter-Portex-Smiths Medical) was inserted between thoracic segments 7-8 using midline approach. After an aspiration test, a test dose of lidocaine (40-60 mg) was given to verify the proper placement of catheter and an
initial volume of ropivacaine 0.35 % (6 ml) was administered to the epidural space identifying the level of analgesia by cold perception. To maintain intraoperative analgesia, a bolus (4-6 ml) of ropivacaine 0.35% was given according to clinical signs. At the end of surgery, the epidural catheter was connected to an elastomeric pump delivering a continuous infusion of ropivacaine 0.2% 7 ml/h as postoperative analgesia. When the post-operative epidural infusion was associated with hypotension (systolic blood pressure < 90 mmHg) not related to other pathophysiological mechanisms, we applied the following stepwise protocol: 500 ml bolus of crystalloids, decrease in ropivacaine infusion rate by 2 ml/h and colloid bolus or vasoactive drugs (ephedrine) as needed. Persistent hypotension required discontinuation of epidural infusion.
For patients in CWI group, after closure of the peritoneal layer, the surgeon inserted a 22.5 cm 19- gauge multi-hole catheter (Painfusor®; Baxter-Plan 1 Health, Amaro, Italy). The catheter was positioned between the previously closed parietal peritoneum and the underside of the transversalis fascia, along the full length of the wound to ensure a uniform distribution. Before closing the surgical wound, a 10 ml bolus of ropivacaine 0.75 % was administered through the catheter that was then connected to an elastomeric pump delivering ropivacaine 0.2% infusion at a flow rate of 10 ml/h.
Morphine was use as rescue therapy in both group for the first 72 hours, administration was provided by PCA devices set to deliver a bolus of 1 mg/dose, with a 15 min lockout time and maximum dose of 30 mg per day.
All patients also received 1000 mg of paracetamol every 6 hours.
The catheters were removed 72 hours after the procedure.
Protocol study
Primary endpoint was dynamic pain levels during the first two days after surgery. Postoperative pain level was evaluated using the Verbal Numeric Scale
(VNS), ranging from 0 to10. We assessed pain at rest (static) and at coughing (dynamic) at T12, 24, 48 and 72 hours postoperatively. Values were recorded by dedicated nurses not aware of the details of the study. Secondary endpoints were; number of daily boluses of morphine requested and administrated,
time of bowel activity resumption, incidence of PONV, length of hospital stay (LOS), side effects including hypotension, motor or sensory block, symptoms of systemic toxicity related to absorption of local anesthetic.
All patients were treated according to the enhanced recovery protocol practiced in our centre for pancreatic surgery. Discharge criteria were established a priori.
Nociceptive and inflammatory mediator collection and assay
As a pilot trial, we analysed circulating cytokines IL-1,TNF, IL-6, chemokines CCL2 and IL-8 and the pro-inflammatory mediator Pentraxin 3 (PTX3) in a cohort of 20 consecutive pancreaticoduodenectomy (the Whipple procedure) cases, 10 treated with TEA and 10 with CWI. We performed blood tests at T0 (preoperative), T+24 and 48 hours and postoperative day 7 (D7). Methods used were Sandwich and Multi-Plex ELISA.12-14
Sample Size and Statistical Analysis
The sample size of the study population was assessed on the primary endpoint, the evaluation of postoperative VNS comparing two treatments. Retrospective data indicated that
VNS mean value for epidural analgesia during the first two postoperative days after pancreatic resections was 3.05 ± 1 at rest and 3.78 ± 1 during coughing or mobilization. The total sample size calculation, to observe a reduction of 20% of VNS during coughing was 80, with an alpha error of 0.05, and a power of 90%. Continuous variables were reported as mean, standard deviation (SD) and range; categorical as absolute value and percentage. T-test and Mann-Whitney test were used for comparative analysis of quantitative data; Chi-square and Fischer’s exact test for categorical variables. P-value < 0.05 was considered statistically significant.
All analyses were conducted using Stata 11(StataCorp LP, Texas, USA) with the support of an external statistician.
RESULTS
Of the 40 patients enrolled in the TEA group, three were excluded for dislocation of the epidural catheter, persistent hypotension and paresthesia. One patient in the CWI group was excluded due to dislocation of the catheter.
The demographic and surgical characteristics of the two samples were similar (Table 1).
At time T0, when the patients were observed in the PACU, median pain scores at coughing were 0.5 [IQR 0-3] in TEA vs 1.5 [IQR 0-3] in CWI group. The static and dynamic assessment of pain by VNS, during the following 72 hours, showed no statistically significant differences in the two groups and pain control after surgery was satisfactory over time (Figure 1). In both groups the majority of patients maintain a VNS less than 3 at discharge from the PACU and during ward observation (Table2).
The mean difference in VNS scores from T0 to T12between TEA and CWI groups was 0.39 points (95% CI from -0.59 to 1.37 ) at rest and 0.22 points (95% CI from -0.88 to 1.31) after movement (Figure 1). At T12 and T24, the increase of morphine boluses overall required by patients was statistically significant (P < 0.001) (Figure 2).
Table 1: Characteristics of study population and operative data
| Parameters | TEA (n=40) | CWI (n=40) | P value |
| Sex, M/F | 22/18 | 24/16 | 0.863 |
| Age (years) | 64 ± 13 | 65 ± 10 | 0.647 |
| ASA PS I/II/III | 3/24/13 | 4/26/10 | 0.907 |
| Type of surgery, n (%) | |||
| Pancreaticoduodenectomy | 30 (75) | 31 (77) | 0.792 |
| Ampullectomy | 2 (5) | 2 (5) | 1.000 |
| Distal pancreatectomy | 8 (20) | 7 (17) | 0.774 |
| Type of incision, n (%) | |||
| Left subcostal | 10 (25) | 9 (23) | 0.792 |
| Extended right subcostal | 30 (75) | 31 (77) | 0.792 |
| Duration of surgical procedure, min | 406 ± 138 | 389 ± 110 | 0.895 |
| Blood loss (ml) | 360 ± 260 | 311 ± 275 | 0.964 |
| Volume of fluids (ml) | |||
| Crystalloid | 4000 [4000-5000] | 4000 [4000-4500] | 0.789 |
| Colloid | 600 [300-600] | 200 [200-600] | < 0.001 |
| Intraoperative fentanyl (µg) | 150 [150-250] | 400 [400-600] | < 0.001 |
| Intraoperative ropivacaine (mg) | 52 ± 8 | ||
groups are assessed with Chi Square test with Fisher’s correction, or Mann Whitney test.
ASA = American Society of Anesthesiologist physiological status; CWI = Continuous Wound Infiltration; TEA= Thoracic Epidural Analgesia; PPPD = Pancreatoduodenectomy.
Data are described as absolute value (%), mean and standard deviation or median [interquartile range]. Difference between TEA and CWI
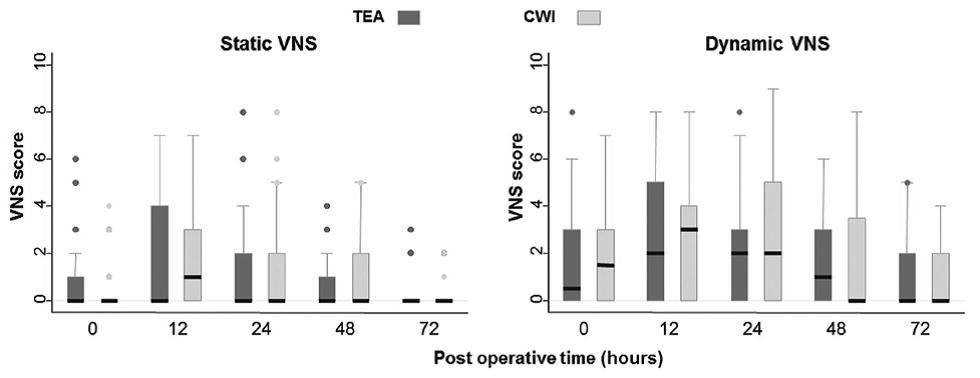
Figure 1: Visual numeric scale scores in the groups at 0-12-24-48-72 h after surgery. A: Static pain score. B: Dynamic pain score.
(Data are represented with box and whisker plots: the median is represented by the bold black line and the interquartile interval is represented as limits of the box. The whiskers are limited from the upper adjacent value, defined as the largest observation that is less than or equal to the third quartile plus 1.5*IQR (interquartile range). Likewise, the lower adjacent value is defined as the smallest observation that is greater than or equal to the first quartile minus 1.5*IQR. Outliers are represented as points outside these limits)
Table 2: Pain scores and morphine consumption
| TEA (n=37) | CWI (n=39) | P value | |
| Static VNS, (%) | |||
| T0 | 2 (5.4) | 1 (2.6) | 1.000 |
| T12 | 10 (27) | 6 (15.4) | 0.403 |
| T24 | 3 (8.1) | 5 (12.8) | 0.475 |
| T48 | 2 (5.4) | 2 (5.1) | 1.000 |
| T72 | 0 | 0 | |
| Dynamic VNS, (%) | |||
| T0 | 5 (13.5) | 7 (17.9) | 0.754 |
| T12 | 14 (37.8) | 13 (33.3) | 1.000 |
| T24 | 7 (18.9) | 14 (35.9) | 0.073 |
| T48 | 8 (21.6) | 9 (23.1) | 0.784 |
| T72 | 2 (5.4) | 1 (2.6) | 1.000 |
| Morphine Consumption | |||
| T0 | 1 (0-7) | 0.5 (0-5) | 0.374 |
| T12 | 4.5 (0-12) | 4 (0-25) | 0.199 |
| T24 | 5 (0-25) | 5 (0-28) | NS0.399 |
| T48 | 2.5 (0-30) | 2 (0-17) | NS0.302 |
| T72 | 0 (0-10) | 0 (0-10) | NS0.470 |
The mean difference in VNS scores from T0 to T12between TEA and CWI groups was 0.39 points (95% CI from -0.59 to 1.37 ) at rest and 0.22 points (95% CI from -0.88 to 1.31) after movement (Figure 1). At T12 and T24, the increase of morphine boluses overall required by patients was statistically significant (P < 0.001) (Figure 2).
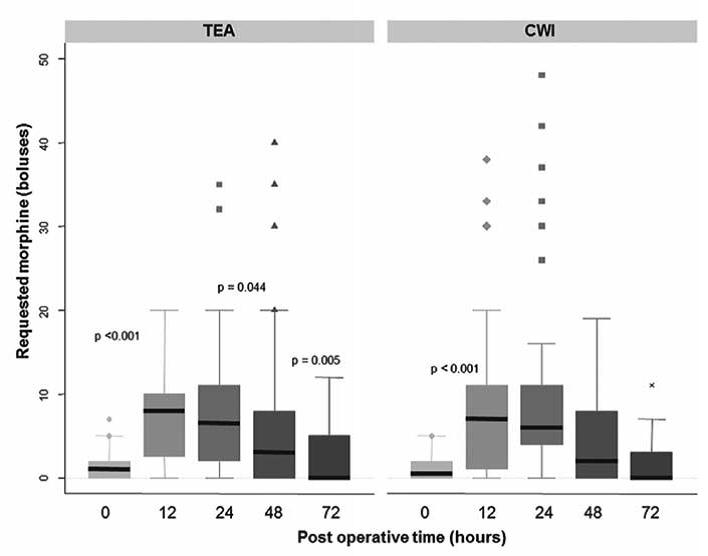 Figure 2: Postoperative opioid analgesic requested boluses of morphine (mg) using patient-controlledanalgesia (PCA)
Figure 2: Postoperative opioid analgesic requested boluses of morphine (mg) using patient-controlledanalgesia (PCA)
Although median daily morphine consumption was 12 mg [IQR 19-23] in the TEA group and 15 mg [IQR 10-29] in the CWI, with no statistically significant difference (p = 0.527). Also morphine consumption between the time intervals wasn’t statistically different in the two groups (Table 2). No patient in either group needed additional therapy for PONV, nor did they show symptoms of systemic toxicity related to the absorption of local anesthetic. In the first postoperative 72 hours, 13% of TEA patient’s demonstrated hemodynamic instability unrelated to surgical complications. No hypotension in the CWI group was observed. The two groups are comparable for the time of first flatus, postoperative day 4 [3-5] vs 3 [3-5] and time of first bowel motion, day 6 [5-6] vs 6 [5-8] for TEA and CWI respectively. Median LOS was 12 days [IQR 9-16] for TEA patients and 10 days [IQR 8-15.5] for patients in CWI group. The only significant difference between the two groups was related to the time that patients spent out of bed in the first two postoperative days, longer in the epidural group (Figure 3).
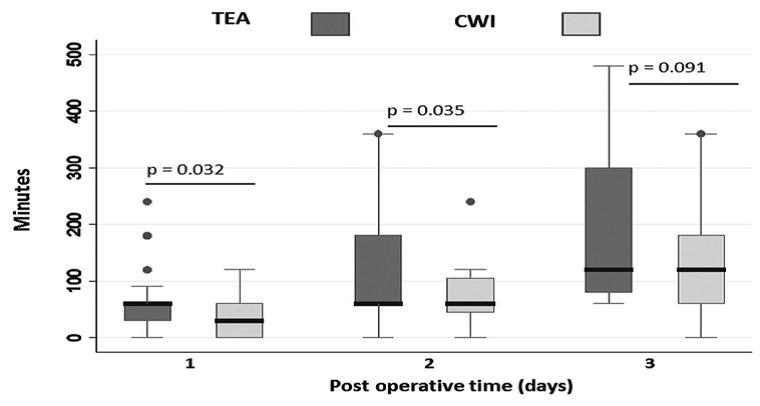 Figure 3: Time (min) spent out of bed during mobilization at postoperative days 1, 2 and 3
Figure 3: Time (min) spent out of bed during mobilization at postoperative days 1, 2 and 3
(Data are represented with box and whisker plots: the median is represented by the bold black line and the interquartile interval are represented as limits of the box. The whiskers are limited from the upper adjacent value, defined as the largest observation that is less than or equal to the third quartile plus 1.5*IQR (interquartile range). Likewise, the lower adjacent value is defined as the smallest observation that is greater than or equal to the first quartile minus 1.5*IQR. Outliers are represented as points outside these limits. Difference between TEA and CWI groups were assessed with Mann-Witney test)
All patients experienced a sharp increase in the pattern of cytokines at T 24 hr, due to major surgical stress, which already started to decrease at T 48 hr and usually returned to baseline levels at post-operative day (POD) 7. More specifically, PTX3 levels in the two groups of patients peaked at T 24 hr with a mean of 62 ± 12 ng/ml in the CWI group and 108 ±11 ng/ml in the TEA. Although a trend to lower PTX3 was apparent in the CWI group, the values did not reach statistical significance (p = 0.1). At later time points: T 48 hr and POD 7, the values were very similar in the two groups (Figure 4).
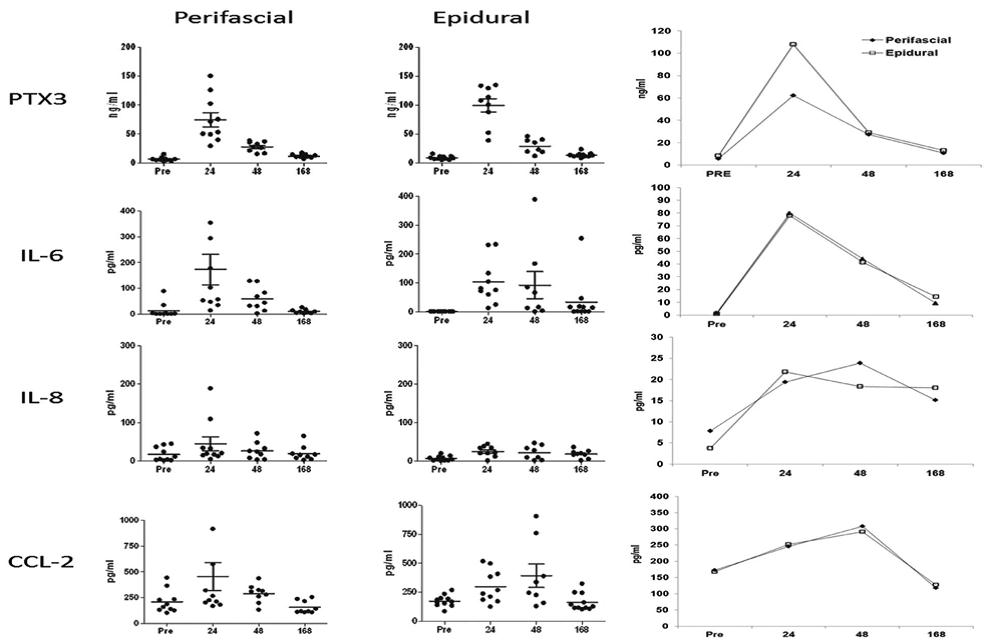
Figure 4: Plasma levels of PTX3, IL-6, IL-8, CCL2 measured by ELISA in perifascial and epidural patients at different time points after surgery
(Data are presented as individual patients (left) and as median values ± SD (n=10 each group). PTX3 and IL-6 peaked at 24 hr; IL-8 and CCL2 peaked at 48 hr. The two groups were similar as inflammatory response elicited (Student’s T test analysis), but a trend to lower PTX3 levels was noted in patients receiving subfascial analgesia)
Likewise the IL-6 levels and pro-inflammatory chemokines CCL2 and IL-8 did not differ in the two patient groups (Figure 4). Levels of TNF and IL-1 were barely detectable in blood (1-5 pg/ml) and were not modulated after surgery. Overall, with two different analgesic treatments, we observed a similar inflammatory response after surgery.
DISCUSSION
Epidural analgesia has been recognized as the “gold standard” of analgesic modalities during major abdominal surgery. TEA has also the benefit, by sympathetic blocking, of attenuating stress response to surgery which will moderate systemic inflammation during and after surgery.15 Nevertheless, several studies have argued against the use of TEA in patients undergoing pancreatoduodenectomies concluding that epidural patients observed better
pain control than patients treated with intravenous analgesia but higher rates of major gastrointestinal complications such as pancreatic fistulae.7,16 Further analyses have demonstrated that the hemodynamic instability occurring frequently during perioperative epidural analgesia17 was poorly tolerated in pancreatoduodenectomy and detrimental for anastomoses’ healing.5 Recent evidence suggests that the use of CWI is a therapeutic option as part of multimodal analgesia in different type of surgery.11,18-20
Administration of local anesthetic into the wound hold an inhibitory effect on NMDA receptors.21,22 which contribute to reduce nociceptive input to the central nervous system and seems to reduce the release of inflammatory mediators.23 Therefore, several clinical trials have been conducted to assess the benefits of CWI.24 The findings have been highly variable, depending on the dose of anesthetic and the depth of catheter placement.10 25. We chose the preperitoneal catheter location based on the results of previous studies.8,10 In our study, pain scores were similar between the groups and no statistically significant differences were found. This finding is supported by other reports in which CWI ensures analgesia comparable to the epidural approach after major abdominal surgery.26,27 Mobilization in both groups occurred on the first day. Regarding the time of stay out of bed, we noted that this was longer in the TEA group despite a similarity in pain scores. These findings were comparable to those of Revie and colleagues,28 who found no correlation between scores for dynamic pain and number of steps taken in the first 48 h after surgery. Indeed, this time may be affected also by the presence of lines and tubes, psychological factors and patient expectations. The time to bowel recovery was reduced in CWI group, probably as a direct effect of local anaesthetic on the peritoneal membrane29 or a systemic anti-inflammatory effect of local anesthetic.30 The length of hospital stay was a little shorter in the CWI analgesia group. With regard to the search of cytokine levels in our small sample, our results showed that the two treatment groups had similar levels of inflammatory mediators. Even if lower levels of PTX3 was observed in CWI group, the lack of a clear systemic anti-inflammatory effect of the local anesthetic could be due to the huge inflammatory response caused by major surgery as is the case for pancreatic interventions. As both groups received treatment with local anesthetic,we cannot exclude that an untreated control group would have experienced a greater inflammatory response.
CONCLUSION
Until now epidural analgesia has been the main, if not the only, technique considered in enhance recovery protocols. We conclude that none of the two techniques (CWI and TEA) is superior to the other on pain control after pancreatic surgery. We observed a similar inflammatory response after surgery for the two groups. CWI is an attractive alternative to epidural analgesia in postoperative pain management after pancreatic surgery because it does not affect hemodynamics, has fewer side effects and doesn’t have any serious complication as epidural analgesia.
Authors’ contribution:
MRS: Study design, data analysis, writing the paper
PZ.: Data collection, writing the paper
AM: Study design, data analysis, writing the paper
GC: Data analysis, reviewing the paper
FG: Patient recruitment, data collection
CR: Patient recruitment, data collection
SG: Patient recruitment, data collection
SP: Design the study, sample analysis, writing the paper
PA: Design the study, sample analysis, writing the paper
AZ: Design the study, writing the paper, reviewing the paper
REFERENCES
- Liu SS, Carpenter RL, Mackey DC, Thirlby RC, Rupp SM, Shine TS, et al. Effects of perioperative analgesic technique on rate ofrecovery after colon surgery. Anesthesiology. 1995 Oct;83(4):757-65. [Pub Med][Free full text]
- Kehlet H, Dahl j. Anaesthesia, surgery, and challenges in postoperative recovery. Lancet2003; 362:1921-8. [Pub Med][Free full text]
- Ready I. Acute pain: lessons learned from 25000 patients. RegAnesth Pain Med 1999;24:499-505. [Pub Med]
- Wang SC, Chang YY, Chang KY, Hu JS, Chan KH, Tsou MY. Comparison of three different concentrations of ropivacaine for postoperative patient controlled thoracic epiduralanalgesia after upper abdominal surgery. ActaAnaesthesiol Taiwan 2008;46(3):100-5. [Pub Med][Free full text] doi: 10.1016/S1875-4597(08)60002-8.
- Pratt WB,Steinbrook RA,Maithel SK,Vanounou T,Collery MP,Vollmer CM. Epiduralanalgesia for pancreatoduodenectomy: a critical appraisal. J. Gastrointest. Surg. 2008;12:1207-20. [Pub Med][Free full text] doi: 10.1007/s11605-008-0467-1. Epub 2008 Feb 9.
- Kehlet H, Liu S. Continuous local anesthetic wound infusion to improve postoperative outcome. Anesthesiology 2007;107:369-71. [Pub Med][Free full text]
- Xu J. Brennan TJ. Guarding pain and spontaneous activity of nociceptors after skin versusskinplus deeptissue incision. Anesthesiology 2010;112(1):153-64. [Pub Med][Free full text] doi: 10.1097/ALN.0b013e3181c2952e.
- Beaussier M, El’Ayoubi H, Schiffer E, Rollin M, Parc Y, Mazoit JX, et al. Continuous preperitoneal infusion ofropivacaine provides effective analgesia and accelerates recovery after colorectal surgery: arandomized, double-blind, placebo-controlled study. Anesthesiology. 2007 Sep;107(3):461-8. [Pub Med][Free full text]
- Kehlet H, Jensen TS,Woolf Cj. Persistent postsurgical pain:risk factors and prevention. Lancet 2006;367:1618-25. [Pub Med][Free full text]
- HollmannmW, Durieux ME. Local anesthetics and the inflammatory response. Anesthesiology 2000;93(3):858-75. [Pub Med][Free full text]
- Forastiere E, Sofra M, Giannarelli D, Fabrizi I, Simone G. Effectiveness of continuouswound infusion of 0.5% ropivacaine by On-Q pain relief system for postoperative painmanagement after open nephrectomy. Br J Anaesth 2008;101(6):841-7. [Pub Med][Free full text] doi: 10.1093/bja/aen309.
- Garlanda C, Bottazzi B, Bastone A, Mantovani A. Pentraxins at the crossroads betweeninnate immunity, inflammation, matrix deposition, and female fertility. Ann Rev Immunol.2005;23:337-66. [Pub Med][Free full text]
- Bottazzi B, Doni A, Garlanda C, Mantovani A. An integrated view of humoral innate imunity: pentraxins as a paradigm. Annu Rev Immunol. 2010;28:157-83. [Pub Med][Free full text] doi: 10.1146/annurev-immunol-030409-101305.
- Germano G, Frapolli R, Simone M, Tavecchio M, Erba E, Pesce S, et al. Antitumor and anti-inflammatory effects of trabectedin on human myxoidliposarcoma cells. Cancer Res 2010Mar 15;70(6):2235-44. [Pub Med][Free full text] doi: 10.1158/0008-5472.CAN-09-2335. Epub 2010 Mar 9.
- Clark AK, Staniland AA, Malcangio M. Fractalkine/CX3CR1 signalling in chronic pain andinflammation. Curr Pharm Biotechnol 2011 Oct;12(10):1707-14. [Pub Med][Free full text]
- Kawasaki T. Ogata M, Kawasaki C, Okamoto K, Sata T. Effects of epidural anaesthesia onsurgical stress-induced immunosuppression during upper abdominal surgery. Br J Anaesth2007;98(2):196-203.
- Bertoglio S, Fabiani A, De Negri P, Corcione A, Merlo D, Cafiero F, et al. The postoperativeanalgesic efficacy of preperitoneal continuous wound infusion compared to epiduralcontinuous infusion with local anesthetics after colorectal cancer surgery: a randomizedcontrolled multicenter study. AnesthAnalg 2012;115(6):1442-50.
- Moraca RJ, Sheldon DG, Thirlby RC. The role of epidural anesthesia and analgesia insurgical practice. Ann Surg 2003;238:663-73. [Pub Med][Free full text]
- Choi DX, Shoeniger LO. For patients undergoing pancreatoduodenectomy epiduralanesthesia and analgesia improves pain but increases rates of intensive care unit admissionsand alterations in analgesics. Pancreas 2010;39:492-7.
- Liu S, Carpenter RL, Neal JM. Epidural anesthesia and analgesia. Anaesthesiology 1995;82:1474-506. [Pub Med][Free full text]
- Carvalho B, Clark D, Angst M. Local and systemic release of cytokines, nerve growth factor, prostaglandin E2 and substance P in incisional wounds and serum followingcaesarean delivery. J of Pain 2008;9(7):650-7.
- Borgeat A, Aguirre T. Update on local anesthetics. CurrOpinAnesthesiol 2010;23:466-71. [Pub Med][Free full text] doi: 10.1097/ACO.0b013e328339eef2.
- Beloeil H, Mazoit JX. Effet des anesthésiqueslocaux sur la réponseinflammatoire postopératoire. AnnalesFrançaisesd’Anesthésie et de Réanimation 2009;28:231-7. [Pub Med][Free full text] doi: 10.1016/j.annfar.2008.12.021. Epub 2009 Mar 17.
- Gupta A, Favaios S, Perniola A, Magnuson A, Berggren I. A meta-analysis of the efficacyof wound catheters for postoperative pain management. Acta AnaesthScand 2011;55(7):785-96. [Pub Med][Free full text] doi: 10.1111/j.1399-6576.2011.02463.x. Epub 2011 May 25.
- Bianconi M, Ferraro L, Ricci R, Lamoli G, Antonelli T, Bighetti G, et al.The pharmacokinetics and efficacy of ropivacaine continuous wound instillation after spinefusion surgery. AnesthAnalg 2004;98:166-72. [Pub Med][Free full text]
- Russel S, Frohlich E, Du Plessis P. The effects of incisional bupivacaine infusions on postoperative opioid consumption and pain scores after total abdominal hysterectomy. SouthAfr J AnaethAnalg 2011;17(3):250-3.
- Ventham NT, Hughes M, O’Neill S, Johns N, Brady AR, Wigmore ST. Wound infiltrationversus epidural analgesia for postoperative pain following abdominal surgery. Br J Surg2013;100(10):1280-9[Pub Med][Free full text]
- Revie E J, Mckeown D, Wilson J, Garden J, Wigmore S. Randomized clinical trial of localinfiltration plus patient-controlled opiate analgesia vs epidural analgesia following liverresection surgery. HPB 2012;14:611-8.
- Holte K, Khelet H. Postoperative ileus: a preventable event. Br J Surg 2000; 87(11):1480-93[Pub Med][Free full text]
- Koppert W, Weigand M, Neumann F, Sittl R, Shettler J, Smelz M, Hering W. Perioperativeintravenous lidocaine has preventive effects on postoperative pain and morphineconsumption after major abdominal surgery. AnesthAnalg 2004;98:1050- 5[Pub Med][Free full text]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube