
Suman Arora*, Kulbhushan Saini**, Neerja Bhardwaj***
*Additional Professor; ***Professor,
Dept of Anesthesiology & Intensive care, Post Graduate Institute of Medical Education & Research (PGIMER), Chandigarh (India)
**Senior Resident,
Cardiac Anesthesia, AIIMS, New Delhi (India)
Correspondence: Dr. Suman Arora, Department of Anesthesiology & Intensive Care, Post Graduate Institute of Medical Education & Research (PGIMER), Chandigarh-160012 (India); E-mail: drsumanarora@hotmail.com
ABSTRACT
Objective: To evaluate and compare the efficacy of orally administered midazolam, clonidine and dexmedetomidine with regard to preoperative sedation, effect on parental separation, acceptance of face mask and recovery profile in children.
Methodology: This was a prospective, randomized, double blind clinical trial, conducted in a tertiary care hospital, in which 80 children in the age group of 1–4 years were included. The study population was divided into three groups and each group was premedicated with one of the three oral premedicants. Patients in Group-M received 0.5 mg/kg of oral midazolam 30 min before the surgery, Group-C received 4 µg/kg of oral clonidine 90 min before the surgery and Group-D received 4 µg/kg of oral dexmedetomidine 60 min before the surgery mixed in honey. In the waiting area sedation score, parental separation score, mask acceptance at induction were measured on 4 point scales. In the PACU, children were monitored for NIBP, ECG, SpO2 and Steward Recovery Score every 15 min for 2 hours. Nausea, vomiting, shivering or other complications if any and time taken to achieve Steward Score of 6 was noted. The statistical analysis was carried out using Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, version 15.0 for Windows).
Results: All the three groups had comparable sedation. Parental separation was easy for children in Group-M (96.6%) and Group-D (93.6%) while it was significantly low in Group-C (63.5%) (p=0.001). Significantly higher number (96.6%) of children in Group-M showed satisfactory mask acceptance in comparison to Group-C (45.8%) and Group-D (25.9%) (p<0.001). Recovery from anaesthesia was significantly faster in Group-M when compared with Group-C and Group-D (p<0.001).
Conclusion: Despite effective preoperative sedation (>90%) with the two alpha-2-agonists, clonidine and dexmedetomidine, parental separation and mask induction was not satisfactory as compared to midazolam.
Key words: Midazolam; Dexmedetomidine; Clonidine; Premdication; Sedation
Citation:Arora S, Saini K, Bhardwaj N. A comparative evaluation of midazolam, clonidine and dexmedetomidine as oral premedicants in children: A double blind randomized clinical trial. Anaesth Pain & Intensive Care 2014;18(4):355-60
INTRODUCTION
Increasing attention has been focused on paediatric premedication as it provides sedation, anxiolysis, reduction of emotional trauma and also facilitates smooth induction.[1-4] Oral midazolam with its rapid onset (20 min) and short duration of action has found favour among anesthesiologists but it is far from an ideal premedicant, having undesirable side effects like hiccoughs, cognitive impairment, amnesia, long term behavioural disturbances and respiratory depression.[5-8] Clonidine and dexmedetomidine, selective, centrally acting partial α-2 agonists have emerged as a potential alternative to midazolam premedication in pediatric patients. They are devoid of the negative effects seen with midazolam.[6-9] The additional benefits with α-2 agonist use includes decrease in the requirement of inhalational agent, stable hemodynamics, decrease in the incidence of postoperative nausea, vomiting, shivering, emergence delirium and opioid requirement.[10-16]. Mountain et al found oral dexmedetomidine comparable to oral midazolam for reduction in parental separation anxiety and mask acceptance.[17] Dahmani et al in a meta-analysis showed oral clonidine superior to oral midazolam in producing sedation, decreasing postoperative pain and emergence agitation.[18]. No study has compared midazolam, clonidine and dexmedetomidine in terms of desirble effects as oral premedicants.
The primary aim of the study was to compare the level of sedation produced by orally administered midazolam, clonidine and dexmedetomidine, while secondary aims were to compare the ease of separation from the parents, acceptance of face mask at inductionand postoperative recovery profile.
METHODOLOGY
This was a prospective, randomized, double blind study conducted in a tertiary care hospital after approval from the institutional ethical committee (No.MS/1270/MS/8115). Written informed consent was obtained from the persons legally responsible for the child prior to inclusion. Eighty five children of ASA status I-II between the age group of 1-4 years were enrolled in the study. Parents of five children denied consent. Eighty children were randomised into three groups using a computer generated random number chart kept in opaque envelope numbered sequentially and opened before the administration of premedication.
Subjects were submitted to general or combined (general + caudal) anesthesia for a variety of elective urogenital surgical procedures of up to 2 hours duration. Children with cardiovascular, gastrointestinal and central nervous system abnormalities or were on systemic analgesics and anticonvulsants were excluded from the study.
Patients in Group-M received 0.5 mg/kg of oral midazolam 30 min before surgery, Group-C received 4 µg/kg of oral clonidine 90 min before the surgery and Group-D received 4 µg/kg of oral dexmedetomidine 60 min before the surgery. Since oral preparations of these premedicants (except miadazolam) are not available, we used injectable preparations mixed in honey to make it palatable. These medications were administered based on the group randomization by an anesthesiologist not involved in the study. The doses and times of administration were based on previously published studies.[3,11,17]The anesthesiologist, who scored the patients behavior preoperatively, provided anesthesia care and collected the data, was blinded to the group assignment.
In the waiting area sedation was scored just before separation from parents using a 4 point scale (1 = asleep; 2 = drowsy, responds to verbal commands/gentle stimulation; 3 = awake, calm, quiet; and 4 = anxious, depressed/agitated/crying).[9] A sedation score of 1, 2 or 3 was considered as an acceptable sedation, whereas a score of 4 was considered as poor sedation.
Parental separation score was also measured on a 4 point scale (1 = asleep; 2 = good separation, awake, calm; 3 = awake, anxious, can be easily reassured; and 4 = crying, cannot be reassured).[9] A separation score of 1 or 2 was considered as an acceptable separation, whereas a score of 3 or 4 was considered difficult separation from the parents.
Mask acceptance at induction was recorded on a 4 point co-operation score [9]. Score1= asleep, calm, awake, co-operative child accepts the mask easily, 2 = Slight fear but can be reassured easily, 3 = Moderate fear and reassured with difficulty and 4 = Crying, needs restraint. A score of 1 and 2 was considered satisfactory while a score of 3 and 4 indicated unsatisfactory mask acceptance.
Induction of anesthesia was accomplished with inhalation of sevoflurane (5-8% in graded increments) in 100% oxygen and intravenous access was secured. Inj. fentanyl 1-2 μg/kg IV was administered for analgesia. Airway was secured with appropriate size endotracheal tube (ETT) using atracurium (0.5 mg/kg). Anesthesia was maintained with nitrous oxide in oxygen (FiO2 0.33) and isoflurane (1.0-1.5%), titrated according to clinical response. General anesthesia was supplemented by caudal block if indicated. Intraoperatively patients were monitored with electrocardiogram (ECG), pulse oximetry (SpO2), non-invasive blood pressure (NIBP) and end tidal carbon dioxide (EtCO2). At the end of surgery nitrous oxide and isoflurane were discontinued and residual neuromuscular blockade was reversed with neostigmine (0.05 mg/kg) and glycopyrrolate (0.01 mg/kg). Once extubated, patients were shifted to post anesthesia care unit (PACU) for observation.
In the PACU, children were monitored for NIBP, ECG, SpO2 and Steward Recovery Score every 15 min for 2 hours.[19] Nausea, vomiting, shivering or other complications if any and time taken to achieve Steward Score of 6 was noted (Table 1).
Table 1: Steward postoperative recovery score
|
Parameter |
Score |
|
|
AWAKE |
Fully Awake |
2 |
|
Arousable |
1 |
|
|
Not responding |
0 |
|
|
VENTILATION |
Can cough or cry |
2 |
|
Breathing easily |
1 |
|
|
Airway requires attention |
0 |
|
|
MOVEMENT |
Moving purposefully |
2 |
|
Moving involuntarily |
1 |
The statistical analysis was carried out using Statistical Package for Social Sciences (SPSS Inc., Chicago, IL, version 15.0 for Windows). A total of 80 children for the three groups were required at a power of 80% and confidence interval of 95% to detect a 20% difference in sedation scores between groups (good sedation score with midazolam to be 60% vs. clonidine or dexmedetomidine 80%). Mean and medians were calculated for all quantitative variables and for measures of dispersion standard deviation and standard error was calculated. For normally distributed data means were compared by using One-way ANOVA. For skewed data and scores Kruskal Wallis test was applied. To see the difference between time-related variables, repeated measure ANOVA was applied. Qualitative or categorical variables were described as frequencies and proportions. Proportions were compared by using Chi square or Fisher’s exact test whichever was applicable. All statistical tests were two-sided and were performed at a significance level of α=0.05.
RESULTS
All the three groups were comparable with respect to gender, weight and ASA status. Children in the midazolam group were younger when compared to those in clonidine and dexmedetomidine groups (p=0.02). The mean duration of anesthesia and surgery was comparable between the three groups (Table 2).
Table 2: Demographic Data
|
Parameter |
Group-M |
Group-C |
Group-D |
P value |
| Age (years) |
2.2 ± 1.2* |
3.0 ± 1.0 |
3.0 ± 1.0 |
0.02 |
| Weight (Kg) |
12.4 ± 3.4 |
13.9 ± 3.4 |
12.9 ± 3.2 |
0.27 |
| Sex (M/F) |
25/4 |
23/1 |
27/0 |
0.09 |
| Duration of anesthesia (min) |
64.6±28.6 |
56.1±29.9 |
77.4±35.7 |
0.058 |
| Duration of Surgery (min) |
50.3±27 |
43.2±25.1 |
60.8±30.1 |
0.076 |
Values are in Mean ± SD, Gender as ratio
An acceptable and comparable sedation (score 1–3) was observed in 96.5% of children in Group-M, 91.6% in Group-C and 96.3% in Group-D respectively (Table 3). Parental separation was significantly easy (score 1 or 2) in 96.6% of children in Group-M and 93.6% in Group-D compared to 62.5% in Group-C (p=0.001) (Table 4). A greater percentage of children in Group-M had a satisfactory mask acceptance compared to Group-C and D (96.6% vs. 45.8% and 25.9% respectively) (p=0.001) (Table 5).
Table 3: Sedation scores after premedication
|
Group |
Number (%) of subjects |
Total |
|
|
Acceptable sedation |
Poor Sedation |
||
| Group-M |
28 (96.5) |
1 (3.4) |
29 (100) |
| Group-C |
22 (91.6) |
2 (8.3) |
24 (100) |
| Group-D |
26 (96.3) |
1 (3.7) |
27 (100) |
Data expressed as number (%); analysed using Chi-square test
Table 4: Parental separation score:
|
Group |
No separation problem |
Separation problem |
Total |
| Group-M |
28 (96.6)* |
1 (3.4) |
29 (100) |
| Group-C |
15 (62.5) |
9 (37.5) |
24 (100) |
| Group-D |
25 (93.6)§ |
2 (7.4) |
27 (100) |
Data expressed as number (%) of subjects; analysed using Chi-square test. P<0.001*midazolam vs clonidine, §dexmedetomidine vs clonidine
Table 5: Mask acceptance score
|
Group |
Number (%) of subjects |
Total |
|
|
Satisfactory acceptance |
Unsatisfactory / poor acceptance |
||
| Group-M |
28 (96.6)* |
1 (3.4) |
29 (100) |
| Group-C |
11 (45.8) |
13 (54.2) |
24 (100) |
| Group-D |
7 (25.9) |
20 (74.1) |
27 (100) |
Data expressed as number (%) of subjects; analysed using Chi-square test. P<0.001midazolam vs. clonidine, midazolam vs dexmedetomidine
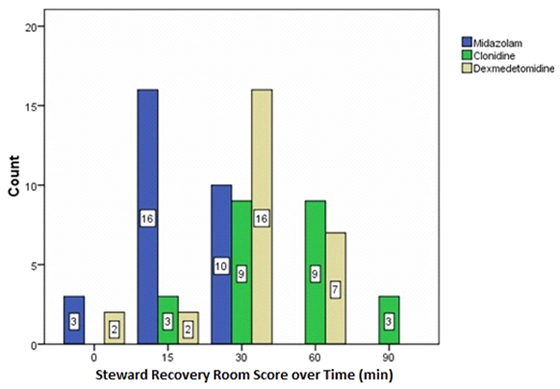
In the PACU, Steward Score of 6 was used as a criterion for discharge fitness. The score was statistically different among three groups on admission to PACU, at 15 min, 30 min (p<0.001) and 60 min postoperative (p=0.02) but it was comparable at 90 and 120 min in all the three groups. On comparison achievement of Steward recovery score 6 (recovery) was significantly earlier in Group-M (30 min) compared to Group-C and Group-D in PACU after which the scores were comparable between the groups. Between Group-C and Group-D recovery was better in Group-D compared to Group-C on admission to PACU but was comparable afterwards (Fig 1).
Figure 1: Bar graph showing Steward Recovery score 6 over time between three groups.
DISCUSSION
This study demonstrated that children receiving oral midazolam, clonidine or dexmedetomidine for premedication all had acceptable and comparable sedation scores. Parental separation and mask acceptance was significantly better when children were administered midazolam premedication compared to premedication with oral clonidine and dexmedetomidine.
The bioavailability of dexmedetomidine has been studied by Antilla et al in healthy adults [20]. However, the oral bioavailability might be very different between adults and children. So far there are no data regarding the ideal oral dose of oral dexmedetomidine or its bioavailability in children of different age groups. Though buccal administration seems to be superior to oral route but this requires patient cooperation as subjects must hold the drug in their mouth for 5 min without swallowing which seems to be impractical for small children there for we used oral route of drug administration. Zub et al first reported the safety and efficacy of intravenous preparation of dexmedetomidine as an oral premedicant in children for procedural sedation and recommended its oral dose to be 3-4 µg/kg [21]. We used 4 µg/kg of oral dexmedetomidine in our study.
The bioavailability of oral clonidine is 55% in children therefore a dose of 4-5 µg/kg is needed for premedication as compared to 2.5 µg/kg via rectal administration and even less following intravascular injection (1.25 µg/kg) [22]. Bioavailability of IM, rectal and oral midazolam is 87%, 18% and 27% respectively. Bioequivalence is present between the 0.15 mg/kg IM dose and the 0.45 mg/kg oral dose of midazolam [23].
In our study, a significant number of children who were sedated after premedication with clonidine and dexmedetomidine, started crying at the time of mask application. This may be related to the difference in the quality of sedation produced by alpha-2 agonists compared to the sedation produced by benzodiazepines. Midazolam produces sedation and anxiolysis by facilitating GABA receptor binding in the cerebral cortex, which enhances the membrane conductance of chloride ions, resulting in a change in membrane polarization that inhibits normal neuronal function. The alpha-2 adrenergic agonists increase parasympathetic outflow and decrease central sympathetic outflow from locus coeruleus in the brainstem. The decreased noradrenergic output of inhibitory neurons including the gamma amino butyric acid (GABA) system, causes sedation, anxiolysis and analgesia.[24] The alpha-2 adrenergic agonist acts on three subtypes; alpha-2a, alpha-2b and alpha-2c receptors. Alpha-2a receptor stimulation leads to sedation, analgesia and sympatholysis. Alpha-2b receptor stimulation results in vasoconstriction and possibly antishivering effect. Stimulation of alpha-2c receptor is responsible for the startle reflex, it is the response of mind and body to an unexpected stimulus, such as a loud noise, flash light or a quick movement near the face.[24]. Poor mask acceptance with alpha agonists observed in our study may be due to the stimulation of alpha 2c receptor. Alpha-2 agonists do not interact with cognitive brain function and therefore act mainly as sleep promoting agent rather than anxiolytic drug. The state of sedation produced by alpha agonists is more similar to normal tiredness or sleepiness where the child can easily be aroused to full consciousness with stimulation.
Kamal et al found oral dexmedetomidine (3 µg/kg) comparable to oral midazolam (0.5mg/Kg) with regard to pre and postoperative level of sedation but dexmedetomidine was associated with less postoperative analgesic use, less incidence of postoperative agitation, shivering and vomiting.[25] Dexmedetomidine was also associated with more haemodynamic stability.[25] Mountain et al found comparable parental separation and mask acceptance between oral dexmedetomidine (4 µg/kg) and oral midazolam (0.5 mg/kg). This difference in results compared to our study may be on account of different study population. Daabiss et al found significantly better scores for sedation, anxiolysis and acceptance of face mask in oral midazolam ketamine group (0.25 mg/kg + 2.5 mg/kg) than oral dexmedetomidine group (3 µg/kg).[26]
Our results are similar to that by Cox et al who found oral midazolam 0.5 mg/kg administered 20-30 min preoperatively, effective in reducing both separation and induction anxiety in children, with minimal effects on recovery times.[5] Fazi et al found midazolam a better premedicant than clonidine for preoperative anxiolysis and that finding is consistent with our results.[27] Trevor et al. also found the quality of induction less satisfactory after clonidine than midazolam premedication.[28] However a meta-analysis by Dahmani et alfound that premedication with clonidine, in comparison with midazolam, exhibited a superior effect on sedation at induction, decreased incidence of emergence agitation and produced a more effective early postoperative analgesia. The use of clonidine was also associated with slightly increased sedation during the first 24 postoperative hours.18] Our study also shows delayed recovery in Group-C when compared with Group-M and Group-D.
Our study showed stable hemodynamics in clonidine and dexmedetomidine premedicated children in comparison to midazolam group, which could be attributed to post synaptic activation of α-2 adrenocepters in the central nervous system that inhibit sympathetic activity and thus can decrease blood pressure and heart rate. Ramesh et al in their study also concluded that oral clonidine (3µg/kg) was effective to attenuate the hemodynamic response to endotracheal intubation.[29] We did not notice any respiratory depression with the any of the premedicant.
Limitations: Limitations of our study include the different timings of premedicant delivery and assessment of sedation score only once, just prior to parental separation which may have prevented a true blinding.
CONCLUSION
In conclusion the present study showed an effective preoperative sedation with midazolam, clonidine and dexmedetomidine when used orally as premedicant. However, mask acceptance and parental separation was better with midazolam compared to clonidine and dexmedetomidine.
REFERENCES
- Beeby DG, Morgan Hughes JO. Behaviour of unsedated children in the anaesthetic room. Br J Anaesth 1980; 52: 279-81. [PubMed][Free Full Text]
- Kain ZN, Hofstadter MB, Mayes LC, et al. Midazolam: effects on amnesia and anxiety in children. Anesthesiology 2000; 93: 676-84. [PubMed]
- Cox RG, Nemish U, Ewen A. Evidence-based clinical update: does premedication with oral midazolam lead to improved behavioural outcomes in children? Can J Anaesth 2006; 53:1213–19. [PubMed][Free Full Text]
- Lonnqvist P, Habre W. Midazolam as premedication: is the emperor naked or just half-dressed? Paediatr Anaesth 2005; 15:263–65. [PubMed]
- Bergendahl H, Lonnqvist P, Eksborg S. Clonidine in paediatric anaesthesia: review of the literature and comparison with benzodiazepines for premedication. Acta Anaesthesiol Scand 2006; 50: 135-43. [PubMed]
- Ghai B, Grandhe RP, Kumar A, Chari P. Comparative evaluation of midazolam and ketamine with midazolam alone as oral premedication. Paediatric Anesthesia 2005; 15: 554-59.[PubMed]
- Tobias JD, Berkenbosch JW. Initial experience with dexmedetomidine in paediatric-aged patients. Pediatr Anaesth 2002; 12: 171–5. [PubMed]
- Schmidt AP, Valinetti EA, Bandeira D, Bertacchi MF, Simões CM, Auler JO Jr. Effects of preanesthetic administration of midazolam, clonidine or dexmedetomidine on postoperative pain and anxiety in children. Pediatr Anaesth 2007; 17: 667-74. [PubMed]
- Inomata S, Kihara S, Yaguchi Y. Reduction in standard MAC and MAC for intubation after clonidine premedication in children. Br J Anaesth 2000; 85: 700–4. [PubMed][Free Full Text]
- Handa F, Fujii Y. The efficacy of oral clonidine premedication in the prevention of postoperative vomiting in children following strabismus surgery. Pediatr Anaesth 2001; 11: 71–4. [PubMed]
- Aantaa R, Jaakola ML, Kallio A, Kanto J. Reduction of the minimum alveolar concentration of isoflurane by dexmedetomidine. Anesthesiology 1997; 86: 1055–60. [PubMed]
- Levanen J, Makela ML, Scheinin H. Dexmedetomidine premedication attenuates ketamine-induced cardiostimulatory effects and post anaesthetic delirium. Anesthesiology 1995; 82: 1117–25. [PubMed]
- Bergendahl H, Lonnqvist P, Eksborg S, et al. Clonidine vs. midazolam as premedication in children undergoing adenotonsillectomy: a prospective, randomized, controlled clinical trial. Acta Anaesthesiol Scand 2004; 48: 1292–1300.[PubMed]
- Mountain BW, Smithson L, Cramolini M, Wyatt TH, Newman M. Dexmedetomidine as a paediatric anaesthetic premedication to reduce anxiety and to deter emergence delirium. AANA. J 2011; 79: 219-24. [PubMed]
- Dahmani S, Brasher C, Stany I et al. Premedication with clonidine is superior to benzodiazepines. A meta analysis of published studies. Acta Anaesthesiol Scand 2010; 54: 397–402. [PubMed]
- Steward DJ. A simplified scoring system for the postoperative recovery room. Can Anaesth Soc J 1975; 22: 111-13.[PubMed]
- Anttila M, Penttilä J, Helminen A, Vuorilehto L, Scheinin H. Bioavailability of dexmedetomidine after extravascular doses in healthy subjects. Br J Clin Pharmacol 2003; 56: 691–3. [PubMed][Free Full Text]
- Zub D, Berkenbosch JW, Tobias JD. Preliminary experience with oral dexmedetomidine for procedural and anesthetic premedication. Pediatr Anesth 2005; 15: 932–8. [PubMed]
- Larson P, Nordlinder A, Bergendahl HTG, Lonnqvist PA, Eksberg S, Almenrader N, et al. Oral bioavailability of clonidine in children. Pediatr Anesth 2011; 21: 335-340. [PubMed]
- Payne K, Mattheyse FJ, Liebenberg D, Dawes T. The pharmacokinetics of midazolam in pediatric patients. Eur J Clin Pharmacol 1989;37: 267 – 272. [PubMed]
- Basker S, Singh G, Jacob R. Clonidine in Paediatrics-A Review. Ind J Anaesth.2009; 53: 270-80. [PubMed][Free Full Text]
- Kamal K, Soliman D, Zakaria D. Oral dexmedetomidine versus oral midazolam as premedication in children. Ain Shams Journal of Anesthesiology 2008; 1: 1-20.
- Daabiss MA, Hashish M. Dexmedetomidine versus ketamine combined with midazolam; a comparison of anxiolytic and sedative premedication in children. BJMP 2011; 4: a441.
- Fazi L, Jantzen EC, Rose JB, Kurth CD, Watcha MF. Comparison of oral clonidine and oral midazolam as preanesthetic medications in the pediatric tonsillectomy patient. Anesth Analg 2001; 92: 56 –61. [PubMed]
- Trevor S, Upadya M, Sinha C, Kaur M. A comparison of midazolam and clonidine as an oral premedication in pediatric patients. Saudi J Anaesth 2012;6:8-11. [PubMed][Free Full Text]
- Cote CJ. Preoperative preparation and premedication. Br J Anaesth 1999; 83:16-28. [PubMed][Free Full Text]
- McMillan CO, Spahr-Schopfer IA, Sikich N, Hartley E, Lerman J. Premedication of children with oral midazolam. Can J Anaesth 1992;39: 545-50. [PubMed]
- Bergendahl H, Lonnqvist P, Eksborg S. Clonidine: an alternative to benzodiazepines for premedication in children. Curr Opin Anaesthesiol 2005; 18: 608-13. [PubMed]
- Ramesh VJ, Bhardwaj N, Batra YK. Comparative study of oral clonidine and diazepam as premedicants in children. Int J Clin Pharmacol Ther 1997; 35: 218- 21. [PubMed]



 Facebook
Facebook Twitter
Twitter GooglePlus
GooglePlus Youtube
Youtube