Anastasios Petrou1, Alexandros Mavrodontidis2, Georgios Karfakis3, Petros Tzimas1, Antonia Liarmakopoulou4, Georgios Papadopoulos5
1Assistant professor; 5Professor
Department of Anesthesiology & Intensive Care, Faculty of Medicine, School of Health Sciences, University of Ioannina, Ioannina, Hellas
2Staff Orthopedic, Department of Orhtopaedics, University Hospital of Ioannina, Ioannina, Hellas
3Resident in Anesthesiology; 4Staff Anesthetist
Department of Anesthesiology, University Hospital of Ioannina, Ioannina, Hellas.
Correspondence: Anastasios Petrou, Department of Anesthesiology, Faculty of Medicine, School of Health Sciences, University of Ioannina, PO BOX: 1186, 45100, Ioannina, Hellas; Tel: +302651009419; Cell: +30697278149; E-mail: apetrou@cc.uoi.gr
ABSTRACT
Calcific tendonitis is a common painful syndrome of the shoulder region that affects mainly women of 40 to 60 years of age. It usually remains asympatomatic at the early stages and in some patients, but produces severe and sometimes protracted pain during the resolution phase. Complex regional pain syndrome (CRPS) and the “frozen shoulder” syndrome are the main entities that need to be considered in the differential diagnosis of the syndrome. Although there are specific criteria to diagnose any of these painful syndromes but occasionally some of these may co-exist and make diagnosis and appropriate treatment quite a challenging task.
We present a case with bilateral calcific tendonitis of the shoulders, complicated with causalgia and reflex sympathetic dystrophy (RSD) syndrome that make the two arms of the CRPS. After failure of the conservative treatment (e.g., non-steroidal anti-inflammatory medications, opioids, physiotherapy, intra-articular steroids) to treat both pain and causalgia, we applied repetitive trials of electroacupuncture together with auricular acupuncture and one trial of intravenous regional anesthesia. The patient gradually responded to treatment and regained normal, painless mobility of the shoulders. She returned to normal life activities after five years of debilitating pain in both of her shoulders.
We believe that electroacupuncture deserves further clinical research in painful musculoskeletal disorders like calcific tendonitis.
Key words: Electroacupuncture; Auricular acupuncture; Complex regional pain syndrome; Reflex sympathetic dystrophy; Calcific tendonitis; Intravenous regional anesthesia
Citation: Petrou A, Mavrodontidis A, Karfakis G, Tzimas P, Liarmakopoulou A, Papadopoulos G. Calcific tendonitis and reflex sympathetic dystrophy in a patient with bilateral frozen shoulder syndrome. Anaesth Pain & Intensive Care 2017;21(2):255-259
Received: 24 Apr 2017, Reviewed: 29 Apr 2017, Accepted: 28 Jun 2017
INTRODUCTION
Calcific tendonitis of the shoulder is a common, painful disorder that arises out of deposition of calcium into the rotator cuff tendons, affecting mainly the supraspinatus tendon and rarely the infraspinatus and the subscapularis tendons.1-4 It has a mean prevalence of 2.7% in asymptomatic patients and mainly affects women in 4th to 6th decades of age and people with sedentary life.5,6
Calcific tendonitis may present with painful but diverse pathological profiles such as adhesive capsulitis, rupture of the rotator cuff tendons, osteolysis of the humeral head curvature and ossifying tendonitis. When symptomatic, after an initial obscure and mostly painless stage, the disease produces severe pain that affects the shoulder area and leads to restricted arm movements.5,7 It usually does not radiate to the elbow joint or the hand. Adhesive capsulitis, also known as frozen shoulder syndrome, is quite often accompanied by protracted periods of pain and immobility.5
CRPS type 1, consist of the so called RSD entity that is thought to derive from excessive sympathetic reaction of a joint and the peri-articular tissues to traumatic or other triggers, like prolonged immobilization. CRPS is characterized by prolonged or excessive pain and changes in skin color, temperature, and/or swelling in the affected area. Type 2 CRPS refers to causalgia syndrome that is derived from partial nerve injury. Typically type 1 CRPS is confirmed not to be associated with nerve injury as is the case for type 2 CRPS 8.
We present a case of a middle aged woman with bilateral frozen shoulder syndrome and calcific tendonitis complicated with long standing RSD of the arm that was treated with acupuncture and intravenous regional anesthesia (IVRA).
CASE REPORT
A 50 years old woman presented in our pain clinic with bilateral frozen shoulder and calcific tendonitis. The diagnosis was set by an orthopedic surgeon based on the painful symptoms that started three years earlier in the right shoulder and two months back in the left shoulder.
At presentation in the pain clinic, the patient was quite anxious and un-willing to provide a detailed history or to co-operate fully in the initial examination. She reported a Visual Analogue Scale (VAS) score of 7 out of 10 in both shoulders. The pain also radiated to the elbows and was intolerable (VAS: 10) during typical arm movements. It was accompanied by intense causalgia (reported again at VAS 10) and prevented her from a peaceful sleep at night during the last months. Consequently the patient was much depressed and reported a score of 18 on the Beck Depression Inventory (BDI) 9.
Even the slightest movement of the arms or digital palpation of the shoulder and scapula produced severe pain. All the corresponding muscles of the upper arms were atrophic while both hands were cold and cyanotic. On digital palpation, the examiner identified multiple trigger points at the scapular and arm muscles.
Arm movements were severely decreased. Abduction (right and left arm respectively) was measured at 60o and 80o, frontal elevation at 70o and 80o while internal rotation could just reach the thighs for both arms.
In the past, the patient received three trials of intra-articular cortisone injections on each shoulder that resulted to insignificant improvement. Non-steroidal anti-inflammatory medications, weak opioids and physiotherapy also failed to produce good outcomes.
We radiologically confirmed the diagnosis of calcific tendonitis together with a clinical confirmation of CRPS of indiscriminate type, as the patient had causalgia together with RSD.
The patient consented to the application of electroacupuncture therapy. We followed a standard electroacupuncture protocol with needling at the GB34, LI4, TW5 , LI15, TW14, GB21, Chien Chen, SI9, SI12, S37, S38 acupuncture points, bilaterally (Figures 1-4). The electrical current was applied for 60 seconds at each point (2Hz – 180 mA) and the trial was repeated every 4 days.10
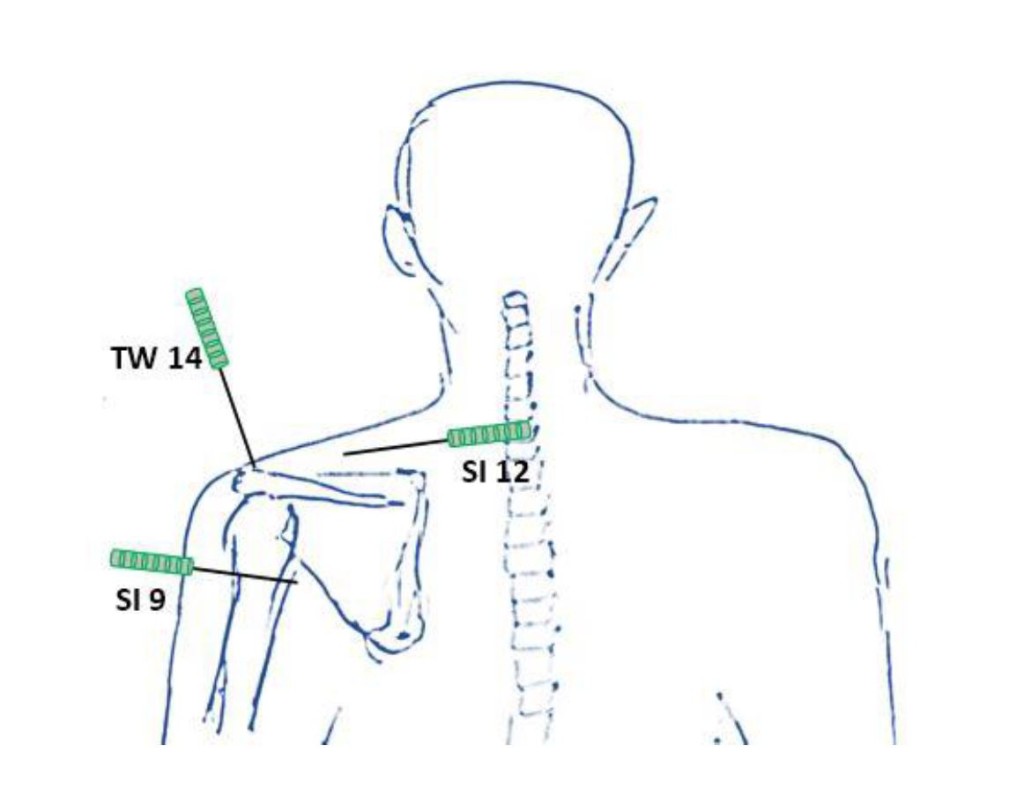
Figure 1: Acupuncture points at the shoulders (back)
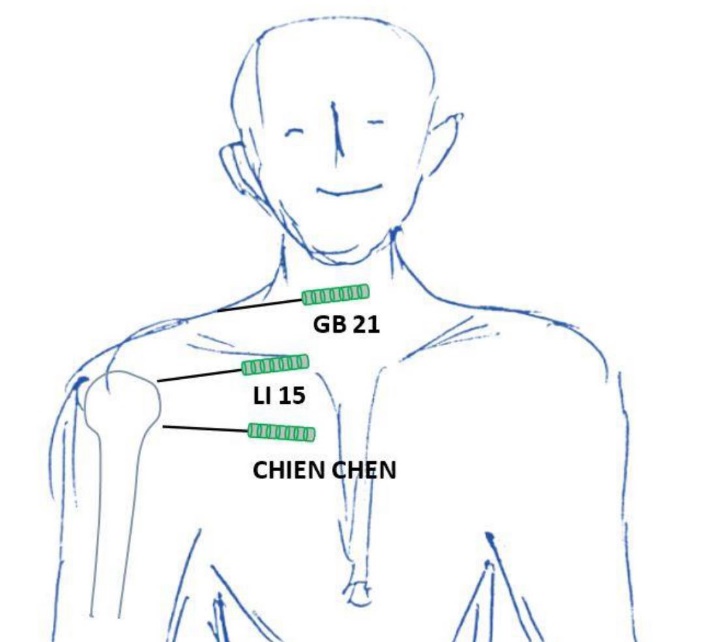
Figure 2: Acupuncture points at the shoulders (front)
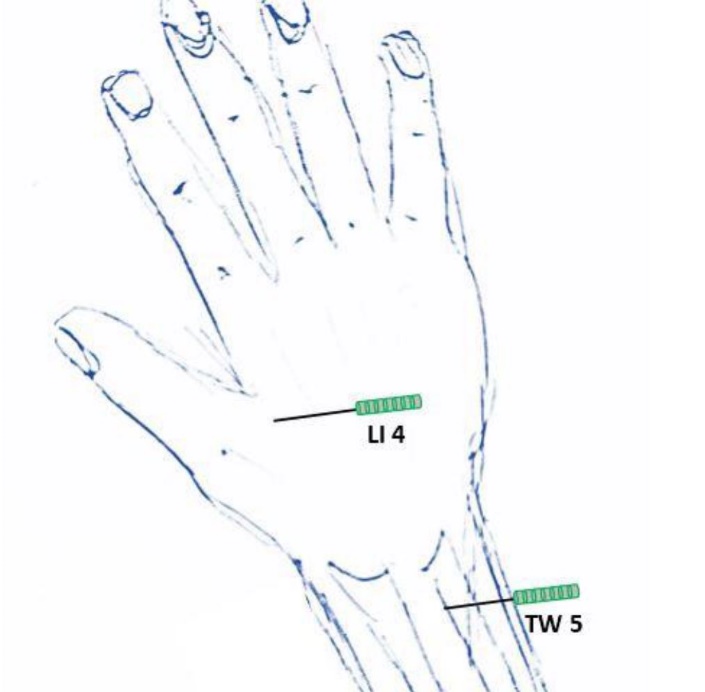
Figure 3: Acupuncture points at the hands (back)
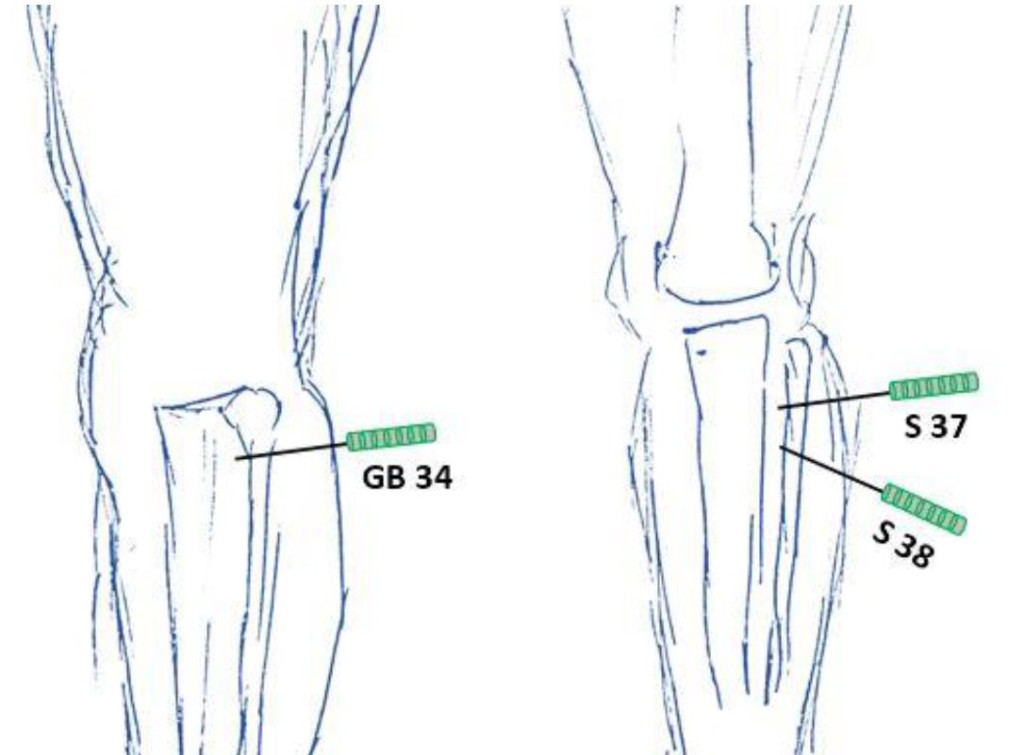
Figure 4: Acupuncture points at the legs (lateral & frontal)
In addition to the above electroacupuncture protocol we applied auricular acupuncture for CPRS treatment at the Shenmen, Sympathetic I & II (Figure 5) with semi-transparent, semi-permanent needles on every other electroacupuncture session (i.e., every 8 days).
Finally trigger points were identified and treated with electroacupuncture (as above) in combination with injections of 1 ml of inj lidocaine 2% on each point. We also advised the patient to attempt pendular movements of the arms as far as possible.
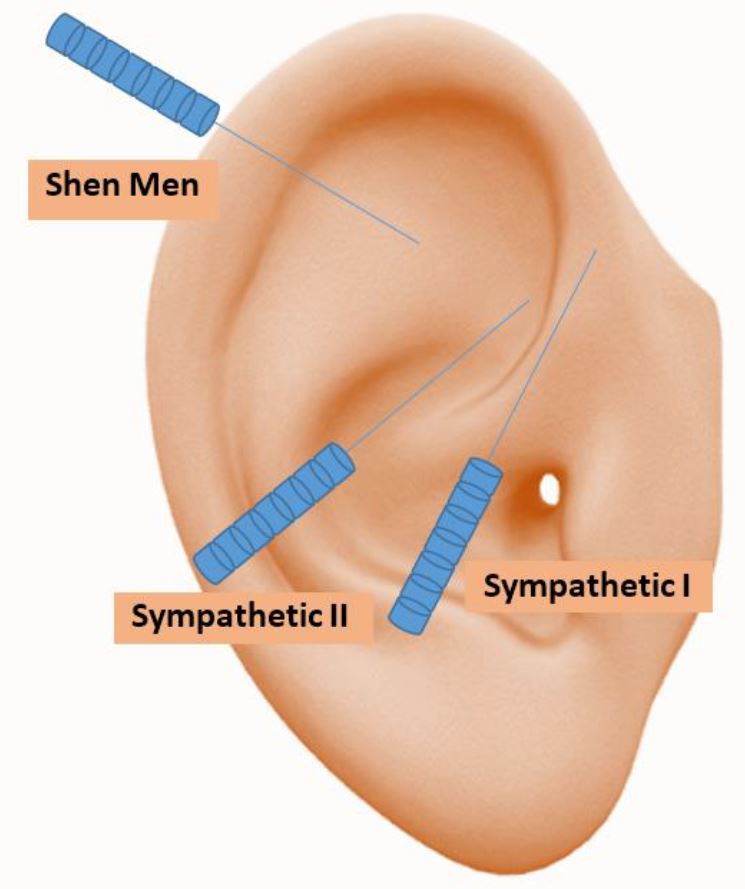
Figure 5: Auricular acupuncture points
After 10 electroacupuncture sessions the patient eventually reported satisfactory reduction of the pain (VAS: 3, both at rest and on movements) at the shoulder region together with a reduction of the causalgia feeling to a VAS of 5.
On clinical examination, the hands gradually regained normal warmth and color and the arm movements reached to 120o and 130o in abduction (right and left arm respectively), 130o and 140o in frontal elevation and in the internal rotation the patient could reach the L5 spine on her back.
As she continued to feel quite stressed and demanded more plausible results, we proposed a stellate ganglion blockade that she declined. So, we discussed the option of regional intravenous anesthesia treatment that she accepted. The trials included the infusion of 20 ml of inj lidocaine 0.2% together with 125 mg of methylprednisolone (in 20 ml), making a total volume of 40 ml.11-13
We noticed that the patient implicitly raised her right arm to 170o of abduction after the inflation of the fist cuff to 220 mmHg. After two IVRA trials the patient reported complete abolition of causalgia in both shoulders and restored abduction and frontal elevation to 180o.
She remains pain free and scored 5 at BDI on repetitive testing even 18 months after her treatment.
DISCUSSION
Adhesive capsulitis, as a complication of calcific tendonitis5,14-16 is thought to result from protracted immobilization of the shoulder joint, due to pain from the calcium deposits. Some of these cases become painless as the range of movement of the shoulder joint deteriorates significantly with time.17 It can also result from systemic diseases like coronary artery disease, hyper- or hypothyroidism, diabetes mellitus and cancer.18-23 It is still unclear if it is a result of or a trigger of inflammation of the surrounding tissues.
It seems that a considerable number of patients with frozen shoulder syndrome present significant decreases in bone density in the affected joint and it has been proposed that this could be an important consideration for therapeutic intervention.24
In the presented case, the diagnosis of CRPS was based on the extreme sensitivity of the shoulder region, the deterioration of free movement of the joint, the reported causalgia and the radiologic findings of calcific tendonitis and adhesive capsulitis.
Frozen shoulder syndrome and RSD have a few common radiologic features. They both present calcific deposits in radiologic evaluation and enhanced radionuclide deposition at the affected tissues.24
Since 1979, the World Health Organization has endorsed acupuncture as a potentially useful mode of treating musculoskeletal pain. Electroacupuncture is usually welcomed by the patients, because it carries very low risk and in combination with exercise, contributes significantly to rehabilitation and restoration of normal functionality of the shoulder, as in the currently presented case.25,26
We applied a combination of auricular and somatic acupuncture to treat CRPS. This intervention resulted in approximately 50% decrease in pain intensity and significant improvement in the range of abduction at the right arm, but it was still unsatisfactory to the patient. IVRA with lidocaine and methylprednisolone was chosen to be the final therapy for this complex pain with good results.
There are only scarce evidence in the literature on the effectiveness of IVRA on CRPS. Poplawski Z et al. have published a series of 16 patients with post-traumatic algodystrophy of the extremities that were followed for 5 years (in mean). The application of IVRA with local anesthetics and corticosteroids in 28 affected hands or feet, resulted in significant improvement in 75% of cases.11 They concluded that the most decisive factor for a successful treatment was the elapsed time between the start of symptoms and the application of therapy to be less than six months.
Zyluk A et al. reported similar results with the application of IVRA in combination with physiotherapy in a smaller series of 36 patients that were followed for 12 months.12
CONCLUSION
So, IVRA is considered a simple, safe and cost-effective technique that offers similar results with other, more established analgesic techniques. As the mechanism of action is not completely understood in the case of CRPS we believe that this technique deserves further investigation in chronic pain syndromes.
Conflict of Interest: None of the author have any conflict of interest by any means with the content of the present case report.
Authors’ Contribution
AP, PT, AL: literature search, drafting, review and final preparation of manuscript
AM, GK, GP: literature search, drafting and final review of manuscript
REFERENCES
1Assistant professor; 5Professor
Department of Anesthesiology & Intensive Care, Faculty of Medicine, School of Health Sciences, University of Ioannina, Ioannina, Hellas
2Staff Orthopedic, Department of Orhtopaedics, University Hospital of Ioannina, Ioannina, Hellas
3Resident in Anesthesiology; 4Staff Anesthetist
Department of Anesthesiology, University Hospital of Ioannina, Ioannina, Hellas.
Correspondence: Anastasios Petrou, Department of Anesthesiology, Faculty of Medicine, School of Health Sciences, University of Ioannina, PO BOX: 1186, 45100, Ioannina, Hellas; Tel: +302651009419; Cell: +30697278149; E-mail: apetrou@cc.uoi.gr
ABSTRACT
Calcific tendonitis is a common painful syndrome of the shoulder region that affects mainly women of 40 to 60 years of age. It usually remains asympatomatic at the early stages and in some patients, but produces severe and sometimes protracted pain during the resolution phase. Complex regional pain syndrome (CRPS) and the “frozen shoulder” syndrome are the main entities that need to be considered in the differential diagnosis of the syndrome. Although there are specific criteria to diagnose any of these painful syndromes but occasionally some of these may co-exist and make diagnosis and appropriate treatment quite a challenging task.
We present a case with bilateral calcific tendonitis of the shoulders, complicated with causalgia and reflex sympathetic dystrophy (RSD) syndrome that make the two arms of the CRPS. After failure of the conservative treatment (e.g., non-steroidal anti-inflammatory medications, opioids, physiotherapy, intra-articular steroids) to treat both pain and causalgia, we applied repetitive trials of electroacupuncture together with auricular acupuncture and one trial of intravenous regional anesthesia. The patient gradually responded to treatment and regained normal, painless mobility of the shoulders. She returned to normal life activities after five years of debilitating pain in both of her shoulders.
We believe that electroacupuncture deserves further clinical research in painful musculoskeletal disorders like calcific tendonitis.
Key words: Electroacupuncture; Auricular acupuncture; Complex regional pain syndrome; Reflex sympathetic dystrophy; Calcific tendonitis; Intravenous regional anesthesia
Citation: Petrou A, Mavrodontidis A, Karfakis G, Tzimas P, Liarmakopoulou A, Papadopoulos G. Calcific tendonitis and reflex sympathetic dystrophy in a patient with bilateral frozen shoulder syndrome. Anaesth Pain & Intensive Care 2017;21(2):255-259
Received: 24 Apr 2017, Reviewed: 29 Apr 2017, Accepted: 28 Jun 2017
INTRODUCTION
Calcific tendonitis of the shoulder is a common, painful disorder that arises out of deposition of calcium into the rotator cuff tendons, affecting mainly the supraspinatus tendon and rarely the infraspinatus and the subscapularis tendons.1-4 It has a mean prevalence of 2.7% in asymptomatic patients and mainly affects women in 4th to 6th decades of age and people with sedentary life.5,6
Calcific tendonitis may present with painful but diverse pathological profiles such as adhesive capsulitis, rupture of the rotator cuff tendons, osteolysis of the humeral head curvature and ossifying tendonitis. When symptomatic, after an initial obscure and mostly painless stage, the disease produces severe pain that affects the shoulder area and leads to restricted arm movements.5,7 It usually does not radiate to the elbow joint or the hand. Adhesive capsulitis, also known as frozen shoulder syndrome, is quite often accompanied by protracted periods of pain and immobility.5
CRPS type 1, consist of the so called RSD entity that is thought to derive from excessive sympathetic reaction of a joint and the peri-articular tissues to traumatic or other triggers, like prolonged immobilization. CRPS is characterized by prolonged or excessive pain and changes in skin color, temperature, and/or swelling in the affected area. Type 2 CRPS refers to causalgia syndrome that is derived from partial nerve injury. Typically type 1 CRPS is confirmed not to be associated with nerve injury as is the case for type 2 CRPS 8.
We present a case of a middle aged woman with bilateral frozen shoulder syndrome and calcific tendonitis complicated with long standing RSD of the arm that was treated with acupuncture and intravenous regional anesthesia (IVRA).
CASE REPORT
A 50 years old woman presented in our pain clinic with bilateral frozen shoulder and calcific tendonitis. The diagnosis was set by an orthopedic surgeon based on the painful symptoms that started three years earlier in the right shoulder and two months back in the left shoulder.
At presentation in the pain clinic, the patient was quite anxious and un-willing to provide a detailed history or to co-operate fully in the initial examination. She reported a Visual Analogue Scale (VAS) score of 7 out of 10 in both shoulders. The pain also radiated to the elbows and was intolerable (VAS: 10) during typical arm movements. It was accompanied by intense causalgia (reported again at VAS 10) and prevented her from a peaceful sleep at night during the last months. Consequently the patient was much depressed and reported a score of 18 on the Beck Depression Inventory (BDI) 9.
Even the slightest movement of the arms or digital palpation of the shoulder and scapula produced severe pain. All the corresponding muscles of the upper arms were atrophic while both hands were cold and cyanotic. On digital palpation, the examiner identified multiple trigger points at the scapular and arm muscles.
Arm movements were severely decreased. Abduction (right and left arm respectively) was measured at 60o and 80o, frontal elevation at 70o and 80o while internal rotation could just reach the thighs for both arms.
In the past, the patient received three trials of intra-articular cortisone injections on each shoulder that resulted to insignificant improvement. Non-steroidal anti-inflammatory medications, weak opioids and physiotherapy also failed to produce good outcomes.
We radiologically confirmed the diagnosis of calcific tendonitis together with a clinical confirmation of CRPS of indiscriminate type, as the patient had causalgia together with RSD.
The patient consented to the application of electroacupuncture therapy. We followed a standard electroacupuncture protocol with needling at the GB34, LI4, TW5 , LI15, TW14, GB21, Chien Chen, SI9, SI12, S37, S38 acupuncture points, bilaterally (Figures 1-4). The electrical current was applied for 60 seconds at each point (2Hz – 180 mA) and the trial was repeated every 4 days.10
Figure 1: Acupuncture points at the shoulders (back)
Figure 2: Acupuncture points at the shoulders (front)
Figure 3: Acupuncture points at the hands (back)
Figure 4: Acupuncture points at the legs (lateral & frontal)
In addition to the above electroacupuncture protocol we applied auricular acupuncture for CPRS treatment at the Shenmen, Sympathetic I & II (Figure 5) with semi-transparent, semi-permanent needles on every other electroacupuncture session (i.e., every 8 days).
Finally trigger points were identified and treated with electroacupuncture (as above) in combination with injections of 1 ml of inj lidocaine 2% on each point. We also advised the patient to attempt pendular movements of the arms as far as possible.
Figure 5: Auricular acupuncture points
After 10 electroacupuncture sessions the patient eventually reported satisfactory reduction of the pain (VAS: 3, both at rest and on movements) at the shoulder region together with a reduction of the causalgia feeling to a VAS of 5.
On clinical examination, the hands gradually regained normal warmth and color and the arm movements reached to 120o and 130o in abduction (right and left arm respectively), 130o and 140o in frontal elevation and in the internal rotation the patient could reach the L5 spine on her back.
As she continued to feel quite stressed and demanded more plausible results, we proposed a stellate ganglion blockade that she declined. So, we discussed the option of regional intravenous anesthesia treatment that she accepted. The trials included the infusion of 20 ml of inj lidocaine 0.2% together with 125 mg of methylprednisolone (in 20 ml), making a total volume of 40 ml.11-13
We noticed that the patient implicitly raised her right arm to 170o of abduction after the inflation of the fist cuff to 220 mmHg. After two IVRA trials the patient reported complete abolition of causalgia in both shoulders and restored abduction and frontal elevation to 180o.
She remains pain free and scored 5 at BDI on repetitive testing even 18 months after her treatment.
DISCUSSION
Adhesive capsulitis, as a complication of calcific tendonitis5,14-16 is thought to result from protracted immobilization of the shoulder joint, due to pain from the calcium deposits. Some of these cases become painless as the range of movement of the shoulder joint deteriorates significantly with time.17 It can also result from systemic diseases like coronary artery disease, hyper- or hypothyroidism, diabetes mellitus and cancer.18-23 It is still unclear if it is a result of or a trigger of inflammation of the surrounding tissues.
It seems that a considerable number of patients with frozen shoulder syndrome present significant decreases in bone density in the affected joint and it has been proposed that this could be an important consideration for therapeutic intervention.24
In the presented case, the diagnosis of CRPS was based on the extreme sensitivity of the shoulder region, the deterioration of free movement of the joint, the reported causalgia and the radiologic findings of calcific tendonitis and adhesive capsulitis.
Frozen shoulder syndrome and RSD have a few common radiologic features. They both present calcific deposits in radiologic evaluation and enhanced radionuclide deposition at the affected tissues.24
Since 1979, the World Health Organization has endorsed acupuncture as a potentially useful mode of treating musculoskeletal pain. Electroacupuncture is usually welcomed by the patients, because it carries very low risk and in combination with exercise, contributes significantly to rehabilitation and restoration of normal functionality of the shoulder, as in the currently presented case.25,26
We applied a combination of auricular and somatic acupuncture to treat CRPS. This intervention resulted in approximately 50% decrease in pain intensity and significant improvement in the range of abduction at the right arm, but it was still unsatisfactory to the patient. IVRA with lidocaine and methylprednisolone was chosen to be the final therapy for this complex pain with good results.
There are only scarce evidence in the literature on the effectiveness of IVRA on CRPS. Poplawski Z et al. have published a series of 16 patients with post-traumatic algodystrophy of the extremities that were followed for 5 years (in mean). The application of IVRA with local anesthetics and corticosteroids in 28 affected hands or feet, resulted in significant improvement in 75% of cases.11 They concluded that the most decisive factor for a successful treatment was the elapsed time between the start of symptoms and the application of therapy to be less than six months.
Zyluk A et al. reported similar results with the application of IVRA in combination with physiotherapy in a smaller series of 36 patients that were followed for 12 months.12
CONCLUSION
So, IVRA is considered a simple, safe and cost-effective technique that offers similar results with other, more established analgesic techniques. As the mechanism of action is not completely understood in the case of CRPS we believe that this technique deserves further investigation in chronic pain syndromes.
Conflict of Interest: None of the author have any conflict of interest by any means with the content of the present case report.
Authors’ Contribution
AP, PT, AL: literature search, drafting, review and final preparation of manuscript
AM, GK, GP: literature search, drafting and final review of manuscript
REFERENCES
- Balke M, Bielefeld R, Schmidt C, Dedy N, Liem D. Calcifying tendinitis of the shoulder: midterm results after arthroscopic treatment. Am J Sports Med. 2012;40:657-661. doi: 10.1177/0363546511430202. [PubMed] [Free full text]
- Cho NS, Lee BG, Rhee YG. Radiologic course of the calcific deposits in calcific tendinitis of the shoulder: does the initial radiologic aspect affect the final results? J Shoulder Elbow Surg. 2010;19:267-272. J Shoulder Elbow Surg. 2010 Mar;19(2):267-72. doi: 10.1016/j.jse.2009.07.008. [PubMed]
- Depalma AF, Kruper JS. Long-term study of shoulder joints afflicted with and treated for calcific tendinitis. Clin Orthop. 1961;20:61-72. [PubMed]
- Lippmann RK. Observations concerning the calcific cuff deposit. Clin Orthop. 1961;20:49-60. [PubMed]
- Merolla G, Dave AC, Paladini P, Campi F, Porcellini G. Ossifying tendinitis of the rotator cuff after arthroscopic excision of calcium deposits: report of two cases and literature review. J Orthop Traumatol. 2015;16:67-73. [Free full text]
- Bosworth BM. Calcium deposits in the shoulder and subacromial bursitis: a survey of 12,122 shoulders. JAMA. 1941;116:2477-2482.
- Bayam L, Ahmad MA, Naqui SZ, Chouhan A, Funk L. Pain mapping for common shoulder disorders. Am J Orthop (Belle Mead NJ). 2011;40:353-358. [PubMed]
- Galer BS, Schwartz L, Allen RJ. Complex regional pain syndromes - Type I: reflex sympathetic dystrophy, and type II: causalgia. In: Loeser JD, Butler SH, Chapman CR, Turk DC, editors. Bonica's Management of Pain. Third ed. Philadelphia: Lippincott, Williams & Wilkins; 2001. p. 388-411.
- Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4:561-571. [PubMed] [Free full text]
- Richards D. Simple Health Maintenance. 2nd ed. St Georges, SA: Superior Health Products PTY Ltd; 1991. 172 p.
- Poplawski ZJ, Wiley AM, Murray JF. Post-traumatic dystrophy of the extremities. J Bone Joint Surg Am. 1983;65:642-655. [PubMed]
- Zyluk A. Results of the treatment of posttraumatic reflex sympathetic dystrophy of the upper extremity with regional intravenous blocks of methylprednisolone and lidocaine. Acta Orthop Belg. 1998;64:452-456.
- Soucacos PN, Diznitsas LA, Beris AE, Malizos KN, Xenakis TA, Papadopoulos GS. Clinical criteria and treatment of segmental versus upper extremity reflex sympathetic dystrophy. Acta Orthop Belg. 1998;64:314-321. [PubMed]
- Rokito AS, Loebenberg MI. Frozen shoulder and calcific tendonitis. Curr Opin Orthop. 1999;10:294-304. doi: 10.1097/00001433-199908000-00008. [Free full text]
- Neviaser TJ. Adhesive capsulitis. Orthop Clin North Am. 1987;18:439-443. [PubMed]
- Chen SK, Chou PH, Lue YJ, Lu YM. Treatment for frozen shoulder combined with calcific tendinitis of the supraspinatus. Kaohsiung J Med Sci. 2008;24:78-84. doi: 10.1016/S1607-551X(08)70101-3. [PubMed] [Free full text]
- Noel E. Treatment of calcific tendinitis and adhesive capsulitis of the shoulder. Rev Rhum Engl Ed. 1997;64:619-628. [PubMed]
- Minter WT, 3rd. The shoulder-hand syndrome in coronary disease. J Med Assoc Ga. 1967;56:45-49. [PubMed]
- Wohlgethan JR. Frozen shoulder in hyperthyroidism. Arthritis Rheum. 1987;30:936-939. [PubMed]
- Cheville AL, Tchou J. Barriers to rehabilitation following surgery for primary breast cancer. J Surg Oncol. 2007;95:409-418. [PubMed]
- Bowman CA, Jeffcoate WJ, Pattrick M, Doherty M. Bilateral adhesive capsulitis, oligoarthritis and proximal myopathy as presentation of hypothyroidism. Br J Rheumatol. 1988;27:62-64. [PubMed]
- Ogilvie-Harris DJ, Myerthall S. The diabetic frozen shoulder: arthroscopic release. Arthroscopy. 1997;13:1-8. [PubMed]
- Arkkila PE, Kantola IM, Viikari JS, Ronnemaa T. Shoulder capsulitis in type I and II diabetic patients: association with diabetic complications and related diseases. Ann Rheum Dis. 1996;55:907-914. [PubMed] [Free full text]
- Muller LP, Muller LA, Happ J, Kerschbaumer F. Frozen shoulder: a sympathetic dystrophy? Arch Orthop Trauma Surg. 2000;120:84-87. [PubMed]
- Lathia AT, Jung SM, Chen LX. Efficacy of acupuncture as a treatment for chronic shoulder pain. J Altern Complement Med. 2009;15:613-618. doi: 10.1089/acm.2008.0272. [PubMed] [Free full text]
- Cheing GL, So EM, Chao CY. Effectiveness of electroacupuncture and interferential eloctrotherapy in the management of frozen shoulder. J Rehabil Med. 2008;40:166-170. [PubMed] [Free full text]