Yvon F. Bryan, MD*, Sung M. Kim, BS*, Kathleen N. Johnson (undergraduate), Katherine Schroeder, BA, Mohsin Shafi, BA, Sung T. Kim, BS, Joseph May, BS, Barbara Thomas, BA
*Dr. Bryan and Ms. Kim are co-first authors as they both contributed equally and substantially to the manuscript.
Department of Anesthesiology, Wake Forest School of Medicine, Winston-Salem, North Carolina, USA
My best wishes and kind regards to your family and friends,Correspondence: Yvon F. Bryan, MD, Department of Anesthesiology, Wake Forest School of Medicine, Medical Center Boulevard, Winston-Salem, NC 27157-1009 (USA); Phone: 336-716-4283; Fax: 336-716-8190; Email: ybryan@wakehealth.edu
ABSTRACT
Objective: Cornelia de Lange syndrome (CdLS) is characterized by multiple anatomic malformations, which may affect airway and anesthetic management. The study’s objective was to collect information from families of CdLS patients regarding their perception of their airway and anesthesia experiences and associated complications. This would allow anesthesiologists to evaluate the families’ perspective in order to create a better approach to treating patients.
Methodology: A web-based, 24 question survey was solicited via the CdLS Foundation’s quarterly newsletter (circulation 4,000) It was followed up, via phone, Skype, and e-mail, with questions targeting intubation, ventilation, oxygenation, aspiration, and complications during surgery and procedures requiring sedation. A paper version of the survey was distributed to families and caregivers of the patients at the 2014 CdLS Foundation National Family Conference. The focus of the survey was to obtain the families’/caregivers’ perception related to airway and anesthetic management experiences and perspectives regarding overall clinical care.
Results: We received 70 survey responses (52 web, 18 paper). 23 of the CdLS patients were adults, while 47 were pediatric patients. Fifty-one respondents (72.9%) reported difficulty breathing due to anatomical reasons. Compared to adults, pediatric CdLS patients were reported to have more airway complications with a significantly higher incidence of oxygen desaturation (19.2% vs. 0.0%). Cardiac arrest occurred in 12.8% of pediatric CdLS patients. Thirty-one (44.3%) respondents reported complications caused by the anesthetic or analgesic medication. The most commonly reported complication was unfavorable emergence from anesthesia (52.9%). Upon follow up, we found that a large number of parents did not complete responses due to their lack of understanding or awareness. The perspectives from both caregivers and families illustrated the need to develop patient centered approach for patients with CdLS.
Conclusion: Our study found that CdLS patients experienced extensive problems during airway and anesthetic management. In addition, certain complications were found more frequently in pediatric patients such as, cardiac arrest and difficult intubation. We found that the families were very involved and knowledgeable about their children’s care. However, there was still a lack of awareness in certain areas of airway and anesthetic management. The value of their perspective highlighted the need for a more focused patient centered care for CdLS patients and their families.
Key words: Cornelia de Lange syndrome; Survey; Parents; Perception; Perspective; Airway; Anesthesia
Citation: Bryan YF, Kim SM, Johnson KN, SchroederK, Shafi M, KimST, May J, Thomas B. Survey of anesthetic and airway management in children and adults with Cornelia de Lange syndrome: parents’ perceptions and perspectives. Anaesth Pain & Intensive Care 2017;21(4): 420-426
Presented in part at the 2013 Annual meeting of the International Anesthesia Research Society and at the 6th Cornelia de Lange Syndrome Scientific and Educational Symposium in 2014
INTRODUCTION
Cornelia de Lange syndrome (CdLS), also known as Brachmann de Lange syndrome, is a heterogeneous developmental disorder that affects 1 in 10,000 to 30,000 births.1 The signs associated with this congenital disease vary in severity and are multisystem: craniofacial, central nervous system, cardiac, gastrointestinal, genitourinary, and musculoskeletal. Clinical characteristics include microbrachycephaly, cleft palate, congenital diaphragmatic hernias, cardiac septal defects, gastro-esophageal reflux, pyloric stenosis, and hirsutism.2 Due to these multiple abnormalities, airway and anesthetic management poses a challenge throughout the patient’s lifetime.3,4
Few CdLS patients will survive their early years due to aspiration-related problems, infections, and skeletal and gastrointestinal anomalies; those who manage to surpass into adulthood will need to undergo multiple diagnostic procedures and surgeries to correct structural malformations and gastrointestinal pathologies.5 However, the limited information detailing the airway and anesthetic management of CdLS patients predominantly describes the pediatric population, and not that of adults. These patients are more likely to present with unpredictable responses to anesthetic interventions, which may be compounded with varying autistic and self-harming tendencies.1 The limited case studies available are also inconsistent regarding which preoperative medications should be administered to CdLS patients. Most anesthetic agents have been used for induction, such as ketamine, as well as sevoflurane and N2O.6,7 Patients’ reactions to certain medications have been unpredictable; therefore, which agents to be avoided is still unknown.
Additionally, some airway features, specifically micrognathia, restricted mouth opening, receding chin, and stiff neck may hinder visualization of the vocal cords during laryngoscopy and endotracheal tube (ETT) placement among all CdLS patients.1 Various techniques have been used for airway management, such as direct laryngoscopy with a Macintosh laryngoscope, blind nasotracheal intubation, fiberoptic bronchoscopic intubation using either a wired ETT, or a laryngeal mask airway as a conduit or guided wire through the trachea.6,8-11 Tracheostomy has been performed in cases where there was difficulty visualizing the vocal cords. Although progress has been made in understanding the genetic components of this disorder, the published literature related to airway and anesthetic management is limited to a few case reports. Our aim was to survey parents of CdLS patients to identify their perception of their children’s airway and anesthetic management experiences. We aim to describe the families’ perspective and point of view. This would allow us to better identify the families’ concerns and point of view during airway and anesthetic management in their children, leading to patient-centered care for patients with CdLS.12,13
METHODOLOGY
A web-based survey was posted on the Wake Forest School of Medicine’s Department of Anesthesiology’s website. An invitation to participate in the survey was published in the Cornelia de Lange Syndrome Foundation newsletter which is distributed quarterly to approximately 4,000 families, caregivers, and healthcare professionals. There were no exclusion criteria. The study was approved by the Wake Forest University Health Sciences Institutional Review Board in 2009 as part of a study on the pediatric difficult airway (IRB # 00010253 approved on 10/27/2009). Responses were received and analyzed from July through September 2012, and a grant was awarded by the Foundation to perform additional skype/telephone interviews which were supplemented by a paper survey distributed at the biennial Cornelia de Lange Syndrome Foundation National Family Conference in June 2014. Written consent was obtained from the parents for pictures shown in Figure 1.
The survey consisted of 24 questions related to three main categories: the perception, understanding, and apprehension involved in airway and anesthetic management, and satisfaction with patient care (supplementary material available online). Airway management questions were asked about their perception of any difficult anatomic features, devices used for airway management, problems encountered during laryngoscopy and intubation, and other related complications. Additional questions highlighted their understanding of what happened during anesthetic techniques used for dental, nonsurgical, and surgical procedures. Phone and skype interviews were conducted in order to gain the perspective of the families in regards to concerns and suggestions for overall clinical care of their children.
Statistical analysis:
Data were entered into Microsoft Office Excel 2010 (Microsoft Corporation, Redmond, Washington, USA). Descriptive statistics [mean, standard deviation (SD), and range] were used to characterize the database. 95% confidence intervals are also reported. Chi-squared tests were used to find group differences for categorical variables. P-values < 0.05 were considered statistically significant.
RESULTS
Demographics:
A total of 70 parents or caregivers of pediatric and adult patients (47 pediatric and 23 adult) with CdLS reported their experiences related to diagnostic procedures (imaging, auditory, and other evaluations), dental, and surgical procedures (Table 1).
CdLS patients have distinct anatomic features that may affect airway management (see Table 1 and Figure 1).
Table 1: Demographic and anatomic characteristics
| Parameters | Pediatric
(n=47) |
Adult
(n=23) |
| Age (y) (mean ± SD) | 7.6 ± 5.3 | 28.7 ± 8.4 |
| Age (y) [mean (range)] | 16.3 (0.8 – 17.0) | 30.0 (19.0 – 49.0) |
| Airway Features* Small mouth High arched palate Cleft palate Prominent upper central incisors Receding or short chin Short and/or stiff neck Hypoplastic larynx |
25 (53.2) 18 (38.3) 7 (14.9) 3 (6.4) 17 (36.2) 11 (23.4) 2 (4.3) |
15 (65.2) 14 (60.9) 3 (13.0) 1 (4.4) 8 (34.8) 3 (13.0) 2 (8.7) |
Figure 1: Spectrum of observable facial features in patients with Cornelia de Lange syndrome (CdLS).
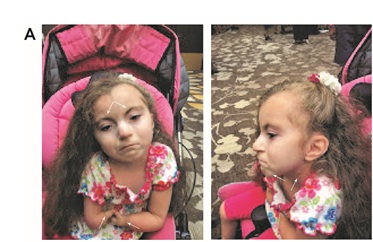

A) Many facial features (left arrows, hirsutism and micromelia; right arrows, micrognathia and short neck)
B) Several facial features (left arrow, small mouth opening; right arrow, short thyromental distance;
C) Fewer facial features
Overall, 72.9% (95% CI = 60.9-82.8%) of the cohort reported that they observed difficulty breathing with sedation, general anesthesia, and/or due to anatomical reasons. However, no significant difference was found in the prevalence of these anatomic features between the pediatric and adult groups (χ2test, 1 degree of freedom [df]; α=0.05). There were 15 (31.9%, 95% CI = 19.1-47.1%) pediatric and 4 (14.8%, 95% CI = 49.5-38.8%) adult patients who had none of the mentioned airway abnormalities, and 27 (57.5%, 95% CI = 42.2-71.7%) pediatric and 15 (55.6%, 95% CI = 42.7-83.6%) adult patients who had at least two of the listed airway abnormalities.
Airway Complications from the Parents’ Perception
Difficult intubations were more frequent in the pediatric group than in the adult group. Similarly, more minor and major airway complications were reported by parents in the pediatric group than in the adult group (Table 2, p < 0.05).
Table 2: Airway complications reported by parents*
| Airway Complications | Pediatric
(n=47) |
Adult
(n=23) |
DNS
Pediatric |
DNS
Adult |
| Difficult intubation† | 13 (27.7) | 0 (0.0) | 19 (40.4) | 8 (34.8) |
| Procedure canceled due to airway | 3 (6.4) | 2 (8.7) | 18 (38.3) | 5 (21.7) |
| Tracheotomy required | 4 (8.5) | 0 (0.0) | 14 (29.8) | 6 (26.1) |
| Smaller endotracheal tube required | 20 (42.6) | 6 (26.1) | 3 (6.4) | 1 (4.4) |
| Difficult Airway Complication Types Reported by Parents
None‡ Minor (O2 problems) Major (unable to place breathing tube) Long-term consequences (laryngeal damage, paralysis, etc.) |
36 (76.6) 9 (19.2) 5 (10.6) 0 (0.0) |
23 (100.0) 0 (0.0) 0 (0.0) 0 (0.0) |
*All data are shown as N (%)
†significantly different between children and adults (p=0.0016)
‡significantly different between children and adults (p=0.0048)
Additional airway problems consisted of aspiration and pneumonia (Table 3). There were no differences in the frequency of aspiration or pneumonia between the pediatric and adult groups.
Airway Issues Related to Age from the Parents’ Perception
Of the total cohort, 18 (25.7%, 95% CI = 16.0-37.6%) patients believed their child’s airway improved with age. Four of the 18 reported (22.2%, 95% CI = 6.4-47.6%) an improvement in airway management since the patients had a tracheostomy placed. Twenty-four (34.3%, 95% CI = 23.3-46.6%) participants were “not sure” whether there were any improvements because the patients did not have additional surgeries or procedures that required anesthesia. In addition, 5 (7.1%, 95% CI = 2.4-15.9%) responses in the pediatric population were “not applicable” because they were too young to see a difference in their airway. There were two pediatric cases in which the responses were “yes” and “no.” For one, the patient had improved intubation in subsequent procedures, but their obstructive sleep apnea worsened. For the second it was stated that the airway improved in one procedure but worsened in another, unrelated procedure.
Anesthetic problems were more frequent with age in only 2 (2.9%, 95% CI = 0.3-9.9%) of the total cohort, one in each of the pediatric and adult populations.
Table 3: Aspiration and pneumonia reported by parents*
| Complications | Pediatric
(n=47) |
Adult
(n=23) |
DNS
Pediatric |
DNS
Adults |
| Pneumonia | 5 (10.6) | 0 (0.0) | 15 (31.9) | 3 (13.0) |
| Vomit/aspiration | 2 (4.3) | 2 (8.7) | 21 (44.7) | 12 (52.2) |
Table 4. Complications unrelated to airway reported by parents*
| Complications | Pediatric
(n=47) |
Adult
(n=23) |
DNS
Pediatric |
DNS
Adults |
| Problems with sedation: anesthetic medication | 20 (42.6) | 11 (47.8) | 10 (21.3) | 3 (13.0) |
| Problems during dental procedure | 6 (12.8) | 6 (26.1) | 15 (31.9) | 9 (39.1) |
| Cardiac arrest | 6 (12.8) | 0 (0.0) | 15 (31.9) | 6 (26.1) |
Anesthetic Issues from the Parents’ Perception
The reactions to the anesthetics varied in type, severity, and duration (see Table 4). Based on the parents’ perception in the pediatric population, non-airway reactions included but were not limited to: anxiety, agitation, nausea, and bradycardia. Airway complications were vomiting and gagging, airway obstruction, obstructive apnea, and respiratory distress. The parents’ perceptions in the adult population of non-airway reactions were nausea during emergence, amnesia, ventricular arrhythmias, and tachycardia. The adult population had the same airway complications as the pediatric population but written responses also included respiratory arrest and decreased oxygen saturation.
Sedatives or anesthetic medications were administered via oral, intravenous, inhalation, or both intravenous and inhalation. A combination of intravenous and inhalational drug administration was used in approximately 40% of the population. A commonly reported concern was the difficulty of obtaining venous access to administer medication due to small veins.
The success of resuscitation attempts for those who experienced cardiac arrest was not surveyed. The cause of cardiac arrest (medication-related, comorbidity of the patient, or a combination) could not be determined.
Emergence and Post-procedure Issues from the Parents’ Perception
The nature of emergence was categorized into “well” (calm and aware of surrounding), “not well” (disoriented, crying, kicking, and screaming), or “both.” “Both” was used in instances when the CdLS patients would wake-up well on specific emergences and not well on others (Table 5).
Table 5: Emergence and post-procedural issues reported by parents*
| Emergence and post-procedural issue | Pediatric
(n=47) |
Adult
(n=23) |
DNS
Pediatric |
DNS
Adults |
| Breathing problems after procedure | 19 (40.4) | 6 (26.1) | 19 (40.4) | 6 (17.4) |
| Desaturation/obstruction after procedure† | 24 (51.1) | 2 (8.7) | 10 (21.3) | 9 (39.1) |
| Problems Related to Timing: Post-Procedural Prior to leaving hospital After leaving hospital |
37 (78.7) 2 (4.3) |
19 (82.6) 1 (4.4) |
8 (17.0) |
3 (13.0) |
| Nature of Emergence Well Not Well Both |
18 (38.3) 24 (51.1) 3 (6.4) |
9 (39.1) 10 (43.5) 0 (0.0) |
2 (4.3) |
4 (17.4) |
*Data shown as N (%)
†significantly different between children and adults (p=0.0013)
Family and/or Caregiver Satisfaction
Thirty-three patients (25 pediatric; 8 adults) representing 47.1% of the total cohort were “very satisfied” with the provided airway management, and 25 patients (14 pediatric; 11 adults) representing 35.7% of the total cohort were “satisfied.”
There were 5 pediatric and 2 adult participants who were “dissatisfied” with the provided airway management. Though the adult cohort did not provide any explanations, the pediatric cohort responders made the following comments to improve airway management: 1) know the anesthetics and post-procedural medications the patient can handle, and 2) CdLS procedures should be treated in child-specific specialty clinics.
Of the total cohort, 60 (85.7%) were either “very satisfied” or “satisfied” with the overall care management.
Perspectives from Parents from Phone/Skype Interviews
Overall, despite some complications, the parents were satisfied with these difficult cases because of adequate communication and precautions taken by the medical staff. Parents preferred speaking on the phone with the actual anesthesiologists who would be performing the case on the day of procedure, rather than a nurse or another anesthesiologist not involved. The consensus regarding future recommendations from “dissatisfied” parents was to have an experienced anesthesiologist with the appropriate skill and necessary equipment, specifically needed for CdLS patients. Additionally, parents found it helpful to be present during the anesthetic induction and immediately following emergence for the safety of their child and for medical team members.
DISCUSSION
Because there is no recommended technique or protocol for CdLS patients due to the variation in the severity of the disease and anatomical abnormalities, we aimed to identify common airway and anesthetic challenges in CdLS patients based on the parents’ perception. Our survey found that CdLS patients experienced extensive problems during airway management. Due to a large number of adult patients with CdLS, we were able to obtain additional information on airway management in adults. There is very little information in the literature on the differences in airway and anesthetic management in children and adults.
The only statistically significant differences in this study were that the pediatric population had a significantly higher prevalence of difficult intubation, airway complications, and oxygen desaturations when compared to the adult population. There was a statistically significant difference in the frequency of desaturation or obstruction of the airway post-procedure. The literature suggests there is an increased incidence of difficulty securing the airway in pediatric CdLS patients compared to adult CdLS patients,5 which our survey substantiates. In several cases, the procedure was canceled due to the inability to adequately secure the airway with the available equipment. In addition, smaller tubes were frequently required; physicians should be aware of this when planning anesthetic/sedation for a patient with CdLS. In this study, bronchospasm, respiratory depression, and laryngotracheal trauma were reported in cases that required smaller tubes and/or procedures that needed to be cancelled. In addition, some patients experienced bradycardia and arrhythmias.
Whether these events were the direct result of intubation attempts or the predisposition of CdLS patients was not investigated. Many parents were keenly aware of specific anesthetic techniques their children received and how their availability varied between institutions, which led to cancellation of their cases. Regarding tracheostomy, many parents stated that they were performed for airway-related issues, but we could not elaborate on the percentage that was required urgently or electively. In these cases, as well as those that experienced cardiac arrest, smaller tubes were required or the airway was unable to be managed with endotracheal intubation. Regarding the incidence of cardiac arrest, it is not possible to know the reason for occurrence or whether the problems with intubations were related to the need for smaller endotracheal tubes. A study by Torres et al. suggests adult CdLS patients have prominent abnormalities, such as hyperactivity, autistic behavior, and/or intellectual disability. Their prominent upper central incisors, oral malformations, and small mouth, may cause extreme difficulty in examining them during their pre-anesthetic assessment.8 Patients that experienced complications during dental procedures had an anatomical abnormality which caused intubation to be difficult due to airway obstruction or small nasal passageway.
Regarding emergence in patients with CdLS, there was variation in the quality of emergence. Some reported excellent wake-up while others had high incidence of emergence agitation—very variable and unsure whether it was related to the medications, anesthetic techniques, and/or paradoxical unpredictable responses.14 In addition, delayed emergence has also been reported, although we did not survey this in our study.15 The many different medications, doses, and techniques that may have been used for the patients, further make it difficult to discern the cause of poor emergence from anesthesia.
Often, CdLS patients present with unpredictable responses and are difficult to manage in the clinical setting. The parents tend to have the best understanding of their child’s condition and how they may react during their anesthetics based on their past experiences, which is why obtaining their perspective was our other main objective. The most frequent comment provided by the parents was that every individual who will interact with CdLS patients should have proper experience before handling such cases, especially if the CdLS patient has self-harming and aggressive tendencies and if they are not able to communicate effectively. Additionally, the medical history of each case should be thoroughly explored beforehand to determine which medication, methods of sedation, and anesthetic techniques would be best tolerated. They also suggested having procedures performed at child specialty facilities to theoretically reduce the likelihood of procedures being cancelled due to inexperienced staff or lack of necessary equipment.
Although our survey relied on knowledge from the families and was not based on medical records, this addressed one of the goals of our study, which was to focus on both the perception and perspective of the parents and determine where the lack of understanding lies. We realize that there is a knowledge gap and there is still a lot of teaching that needs to be done to reduce the caregivers’ apprehension of airway and anesthetic management. This prompted the development of recommendations for questions that families should ask regarding the airway and anesthetic management of their children (available at http://www.cdlsusa.org/docs/publications/anesthesia/BestPracticesFamilies-Anesthetic.pdf). Additionally, the comments provided by the participants may have referred to procedures performed in the 1980s or 1990s when the standard of care and equipment was not equivalent to current standards.
This study provided insight into commonly identified complications in both the pediatric and adult populations. This study was unique in that it described the family’s perception and perspective and a new outlook on the airway and anesthetic management of their children.
LIMITATIONS
There were several limitations in this study. Due to the nature of the survey and the inability to advertise the survey among those affected by CdLS, the sample size, and availability of answers were limited. Additionally the survey was in English and North American, so many non-English speaking families and caregivers were missed and not included. Participants may not have had full details of the procedure and medications used (either because the physicians did not inform them or because they could not comprehend), and thus were unable to provide adequate comments which resulted in the large number of “did not state.”
CONCLUSION
Airway and anesthetic management in Cornelia de Lange syndrome is challenging and should be patient-specific. Certain complications were found more frequently in pediatric patients such as, cardiac arrest and difficult intubation. We found that the families were very involved and knowledgeable about their children’s care. However, there was still a lack of awareness in certain areas of airway and anesthetic management. The families’ viewpoint is important to examine as it may lead to more patient-centered care for children and adults with this syndrome. Further investigation of airway and anesthetic techniques specific to this syndrome is warranted to improve care. The development of specific airway and anesthetic techniques related to issues with intubation, oxygenation, ventilation, and to decrease the risk of aspiration, as well as other complications is key to successful care in all patients with Cornelia de Lange syndrome.
Acknowledgments: The Cornelia de Lange Foundation, especially Marie Concklin-Malloy and Deridre Summa.
Conflict of interest: Funded in part by a grant (YFB) from the Cornelia de Lange Syndrome Foundation, Avon, Connecticut, USA. The Cornelia de Lange Syndrome Foundation had no role in the design, conduct, interpretation, writing, or submission of this study/manuscript.
Authors’ Contribution:
YB &MS: Design of study, survey analysis, manuscript preparation
SK & KJ: Data and statistical analysis, manuscript preparation
KS & JM: Design of survey, data analysis
SK: Data and statistical analysis
BT: Design of survey
REFERENCES
- Washington V, Kaye AD. Anesthetic management of patients with Cornelia de Lange Syndrome. Middle East J Anesthesiol. 2010 Oct;20(6):773-778. [PubMed]
- Boyle MI, Jespersgaard C, Brondum-Nielsen K, Bisgaard AM, Tumer Z. Cornelia de Lange Syndrome. Clin Genet. 2015 Jul;88(1):1-12. doi: 10.1111/cge.12499 [PubMed] [Free full text]
- Kline AD, Calof AL, Lander AD, Gerton JL, Krantz ID, Dorsett D, et al. Clinical, developmental and molecular update on Cornelia de Lange Syndrome and the cohesin complex: Abstracts from the 2014 scientific and educational symposium. Am J Med Genet A. 2015 Jun;167(6):1179-1192. doi: 10.1002/ajmg.a.37056 [PubMed]
- Schroeder K, May J, Thomas BW, Bryan YF. Airway and anesthetic management in patients with Cornelia de Lange syndrome: Different concerns for children and adults. International Anesthesia Research Society Annual Meeting. Anesth Analg. 2013:S-282. [PubMed] [Free full text]
- Corsini LM, De Stefano G, Porras MC, Galindo S, Palencia J. Anaesthetic implications of Cornelia de Lange syndrome. Paediatr Anaesth. 1998;8(2):159-161. [PubMed]
- Hirai T, Nitahara K, Higa K, Iwakiri S, Shono S, Katori K. [Anesthetic management of an infant with Cornelia de Lange Syndrome]. Masui. 2006 Apr;55(4):454-456. [PubMed]
- Mizuno J, Ichiishi N, In-nami H, Hanaoka K. Anesthetic management in a patient with Cornelia de Lange Syndrome. Masui. 2004 Aug;53(8):921-924. [PubMed]
- Torres MD, Calvo E, Fernandez Espla F, Gilsanz F. Anesthetic management of an adult patient with Cornelia de Lange Syndrome. Minerva Anestesiol. 2010 Mar;76(3):229-231. [PubMed]
- Tsukazaki Y, Tachibana C, Satoh K, Fukada T, Ohe Y. [A patient with Cornelia de Lange Syndrome with difficulty in orotracheal intubation]. Masui. 1996 Aug;45(8):991-993. [PubMed]
- Vestergaard L, Dey N, Winding R. Anesthetic considerations in a patient with Cornelia de Lange Syndrome. J Anaesthesiol Clin Pharmacol. 2015 Jul-Sep;31(3):419-420. doi: 10.4103/0970-9185.161732. [PubMed] [Free full text]
- Yokoyama T, Tomoda M, Nishiyama T, Matsuda T, Fujimoto S, Hanaoka K, et al. [General anesthesia for a patient with Cornelia de Lange Syndrome]. Masui. 2000 Jul;49(7):785-787. [PubMed]
- Barry MJ, Edgman-Levitan S. Shared decision making--pinnacle of patient-centered care. N Engl J Med. 2012 Mar 1;366(9):780-781. doi: 10.1056/NEJMp1109283 [PubMed] [Free full text]
- Epstein RM, Street RL Jr. The values and value of patient-centered care. Ann Fam Med. 2011 MarApr;9(2):100-103. [PubMed] [Free full text]
- Stevic M, Milojevic I, Bokun Z, Simic D. Unpredictable drug reaction in a child with Cornelia de Lange Syndrome. Int J Clin Pharm. 2015 Feb;37(1):1-3. [PubMed]