Dmytro Dmytriiev, MD, PhD
Associate Professor, Department of Anesthesiology and Intensive Care, Vinnitsya National Medical University, Vinnytsia, Vinnyts'ka Oblast (Ukraine)
Correspondence: Dmytro Dmytriiev, MD, PhD, Associate Professor, Department of Anesthesiology and Intensive Care, Vinnitsya National Medical University, Pyrohova St, 56, Vinnytsia, Vinnyts'ka Oblast, Ukraine, 21000; E-mail: dmytrodmytriiev@gmail.com, http://orcid.org/0000-0001-6067-681X
ABSTRACT
Management of postoperative pain in children being under-recognized and as a result undertreated for the long period of time. Use of the precise and valid methods for the pain assessment in children is necessary for the following pain management.
Articles in English on the corresponding theme were reviewed (literature search for the period from 1978 to 2018 in PubMed, EMBASE, Cochrane, and Google Scholar). Data from 39 articles were used, key statements of these were synthesized and described in this article.
The latest methods of pain assessment have been described and summarized in this article depending on the age of a child and his/her status of consciousness and ventilation. Different scales utilize different information for the pain assessment, but the validity of them was shown in the studies. All these methods should be used in routine clinical practice and guide the pain management throughout the patient’s stay in the hospital.
In a large prospective study it was shown that the pain level depends not only on the volume of trauma after the operation, but also the localization and character of procedure, so even more traumatic operation can cause more pain. That shows a relevance of the pain management according to the score of different pain scales.
We also tried to utilize in tables recent data from guidelines on the pain management in children and group them according to the level of postoperative pain.
Keywords: Pain, Postoperative; Pain, Assessment; Children; Pain management.
Citation: Dmytriiev D. Assessment and treatment of postoperative pain in children. Anaesth Pain & Intensive Care 2018;22(3):392-400
Received: 15 Jul 2018, Reviewed: 20 Jul 2018, Corrected: 12 Sep 2018, Accepted: 22 Sep 2018
INTRODUCTION
Pain is a feeling, which motivates person to avoid damaging situations and protect impaired tissues during healing process. According to the International Association for the Study of Pain (IASP): pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.1 Adequate control of postoperative pain is not reached in more than 80% of patients in US, which depends on the performed operation, used analgesic methods. Inappropriate control of postoperative pain is associated with an increased morbidity, decreased function and quality of life, prolonged time of recovery, and longer opioid use.2
Postoperative pain in children has been a problem for a long time, as it is often undertreated due to a variety of reasons such as different reactions on noxious stimuli, focusing on the cause but not the symptom, so pain remains under treated. Many children receive inadequate pain management, so pain becomes chronic in 20% of cases.3 So, precise tools for the assessment of pain in different age categories are very important in order to choose appropriate intervention for the pain management.
We reviewed articles in English on the corresponding theme (literature search for the period from 1978 to 2018 in PubMed, EMBASE, Cochrane, Google Scholar). Data from 39 articles were used, key statements of them were synthesized and described in this article.
Precise pain assessment is very important in the pain management, as it allows choosing interventions according to the pain level. Different methods and scales have been used in children, which depend on the age and ability to self-report their feelings.
ABCs of pain management were recommended by the Agency for Health Care Policy and Research (AHCPR), which include the following statements:
Table 1: CRIES scale for the postoperative pain assessment in neonates.4
COMFORT scale includes 6 behavioral items such as alertness, calmness, muscle tone, movement, facial tension, respiratory response for ventilated/crying for nonventilated and 2 physiological items such as heart rate and mean arterial blood pressure. It can be used at the age till 3 years for the assessment of postoperative and procedural pain.5,6 COMFORT scale is represented in the Table 2.5
Table 2. COMFORT scale for the assessment on postoperative and procedural pain
CHEOPS (Children’s Hospital of Eastern Ontario Pain Scale) scale is a behavioral scale for the assessment of postoperative pain in young children. It includes the following parameters as cry, facial, child verbal, torso, touch, legs.7It can be used in children from 0 to 4 years.8 CHEOPS score ranges from 4 to 13, and additional interventions are required for the score above 6. CHEOPS is represented in the Table 3.
Table 3: CHEOPS for the pain assessment in young children
FLACC (Face, Leg, Activity, Cry, and Consolability) tool can be used for the assessment of postoperative and periprocedural pain in children from 2 months to 7 years. It is represented in the Table 4.9
Table 4: FLACC tool for the postoperative and periprocedural pain assessment
Children’s and Infant’s Postoperative Pain Scale (CHIPPS) is used for the assessment of postoperative pain in children from 0 to 5 years, where scores between 0 and 3 indicate the pain absence, and scores above 4 indicate a need for pain management. This scale is represented in the Table 5.10
Table 5: CHIPPS for the postoperative pain assessment
Neonatal Infant Pain Scale (NIPS) is used for the pain assessment in neonates. It includes facial expression, cry, breathing pattern, arms, legs, state of arousal, heart rate and O2 saturation. Score from 0 to 3 indicate absence or mild pain, 4-6 – moderate, 7-10 – severe. This scale is represented in the Table 6.11
Table 6: Neonatal Infant Pain Scale
The most reliable indicator of pain is self-report by the patient, which us usually possible in children older than 4 years. At this age different pain rating scales can be used including the following:
Faces Pain Scale by Bieri is also used for the postoperative pain assessment in children older than 5 years. Training is necessary before using this scale. Faces Pain Scale by Bieri is represented at Figure 2.

OUCHER Scale of Beyer and Wells can be used in children above 3 years. Training of the child is also necessary before performing an assessment. OUCHER Scale of Beyer and Wells is represented in Figure 3.14

Different verbal report scales have also been used. There are 4-point15 to 15-point scales,16 which include different adjectives for describing pain from mild to severe.
Visual analog scale (VAS) is usually a 100-mm long horizontal line, which has labels of ‘No pain’ near one end and ‘Most severe pain imaginable’ at the other end, which requires from patient an ability to compare their pain sensation with the length of the line. Different scales are available online and one of them is represented at Figure 4.

Another way of postoperative pain assessment in children is Parent’s Postoperative Pain Measure (PPPM), which can be used in children from 2 years. It includes 15 questions about child’s behavior and activity. An answer for each question provides 1 score up to a maximum of 15. A score of 6 and more indicates clinically relevant pain.17
Unconscious or Sedated Patients
Pain assessment is a real problem in unconscious or sedated patients. For this purpose several methods have been described:
Table 7: Behavioral Pain Scale
CPOT can be used for pain assessment in intubated and sedated patients based on facial expression, muscle tension and movement, compliance with ventilated breaths for intubated patients or vocalized pain in non-intubated patients. CPOT score of 2 and less indicates no or mild pain, scores above 2 indicates unacceptable level of pain, so further or alternative methods of analgesia should be considered. CPOT is represented at the Table 8.20
Table 8: Critical Care Pain Observation Tool
NPS is used for pain assessment in nonverbal and intubated patients. It assesses facial expression, movements, guarding, vital signs, changes in respiration. Scores of ≤ 2 indicate no pain, 3-6 – moderate pain, ≥ 6 – severe pain; analgesia is required if score is 3 or higher. This scale is represented in the Table 9.21
Table 9: Nonverbal Pain Scale
Management:
The next step after the pain has been assessed and measured is treatment. Different approaches have been used in the provision of sufficient level of analgesia in the postoperative period depending on the intensity of pain the patient has. There was one big prospective study conducted, where the patients were asked to quantify their pain after 179 different surgical interventions.22 So that pain management should be based not only on the level of trauma after the operation, but also the intensity of pain that they experienced.
The less painful surgeries were: excision of solitary lymph nodes (cervical), prepuce surgery, skull and/or brain surgery, and testicular hydrocele surgery. Moderately painful operations were: open umbilical hernia repair, nephrectomy (lap), open inguinal hernia repair; subtotal hysterectomy, spinal canal decompression, and liver resection (atypical, open).
Very painful operations were: incisional hernia repair with alloplastic material, open subtotal hysterectomy, kidney transplantation, open cholecystectomy, tonsillectomy, and complex spinal reconstruction.
For operations, which cause less degree of pain the following measures can be used for the pain management presented in Table 10.23
Table 10: Pain management for less painful operations
For operations, which cause moderate amount of pain the following measures can be used for the pain management, presented in Table 11.23
Table 11: Pain management of moderately painful operations
For operations, which cause severe pain the following can be used for the pain management, presented in Table 12.23
Table 12: Pain management of severely painful operations
CONCLUSION
Pain is an inevitable consequence of surgical interventions in children, which results in a lot of stress and discomfort not only to the patients, but also to their parents. The methods of pain assessment have been described and summarized in this article depending on the age of a child and his/her status of consciousness and ventilation. Different pain measurement tools utilize different information for the pain assessment, but their variable validity has been shown in many of the studies. All available methods should be used in routine clinical practice and guide the pain management throughout the patient’s stay in the hospital.
The pain intensity depends not only upon the level of trauma after the operation, but also the localization and character of procedure. So usually more traumatic surgeries cause more pain. That shows a relevance of the pain management according to the score of different pain scales.
We can utilize the recent guidelines for the pain management in children and group them up according to the level of postoperative pain for ready reference.
Conflict of interest: None declared by the author.
REFERENCE
Associate Professor, Department of Anesthesiology and Intensive Care, Vinnitsya National Medical University, Vinnytsia, Vinnyts'ka Oblast (Ukraine)
Correspondence: Dmytro Dmytriiev, MD, PhD, Associate Professor, Department of Anesthesiology and Intensive Care, Vinnitsya National Medical University, Pyrohova St, 56, Vinnytsia, Vinnyts'ka Oblast, Ukraine, 21000; E-mail: dmytrodmytriiev@gmail.com, http://orcid.org/0000-0001-6067-681X
ABSTRACT
Management of postoperative pain in children being under-recognized and as a result undertreated for the long period of time. Use of the precise and valid methods for the pain assessment in children is necessary for the following pain management.
Articles in English on the corresponding theme were reviewed (literature search for the period from 1978 to 2018 in PubMed, EMBASE, Cochrane, and Google Scholar). Data from 39 articles were used, key statements of these were synthesized and described in this article.
The latest methods of pain assessment have been described and summarized in this article depending on the age of a child and his/her status of consciousness and ventilation. Different scales utilize different information for the pain assessment, but the validity of them was shown in the studies. All these methods should be used in routine clinical practice and guide the pain management throughout the patient’s stay in the hospital.
In a large prospective study it was shown that the pain level depends not only on the volume of trauma after the operation, but also the localization and character of procedure, so even more traumatic operation can cause more pain. That shows a relevance of the pain management according to the score of different pain scales.
We also tried to utilize in tables recent data from guidelines on the pain management in children and group them according to the level of postoperative pain.
Keywords: Pain, Postoperative; Pain, Assessment; Children; Pain management.
Citation: Dmytriiev D. Assessment and treatment of postoperative pain in children. Anaesth Pain & Intensive Care 2018;22(3):392-400
Received: 15 Jul 2018, Reviewed: 20 Jul 2018, Corrected: 12 Sep 2018, Accepted: 22 Sep 2018
INTRODUCTION
Pain is a feeling, which motivates person to avoid damaging situations and protect impaired tissues during healing process. According to the International Association for the Study of Pain (IASP): pain is an unpleasant sensory and emotional experience associated with actual or potential tissue damage, or described in terms of such damage.1 Adequate control of postoperative pain is not reached in more than 80% of patients in US, which depends on the performed operation, used analgesic methods. Inappropriate control of postoperative pain is associated with an increased morbidity, decreased function and quality of life, prolonged time of recovery, and longer opioid use.2
Postoperative pain in children has been a problem for a long time, as it is often undertreated due to a variety of reasons such as different reactions on noxious stimuli, focusing on the cause but not the symptom, so pain remains under treated. Many children receive inadequate pain management, so pain becomes chronic in 20% of cases.3 So, precise tools for the assessment of pain in different age categories are very important in order to choose appropriate intervention for the pain management.
We reviewed articles in English on the corresponding theme (literature search for the period from 1978 to 2018 in PubMed, EMBASE, Cochrane, Google Scholar). Data from 39 articles were used, key statements of them were synthesized and described in this article.
Precise pain assessment is very important in the pain management, as it allows choosing interventions according to the pain level. Different methods and scales have been used in children, which depend on the age and ability to self-report their feelings.
ABCs of pain management were recommended by the Agency for Health Care Policy and Research (AHCPR), which include the following statements:
- Ask about pain regularly. Assess pain systematically.
- Believe the patient and family in their reports of pain and what relieves it.
- Choose pain control options appropriate for the patient, family, and setting.
- Deliver interventions in a timely, logical, coordinated fashion.
- Empower patients and their families. Enable patents to control their course to the greatest extent possible.12
- CRIES scale;
- COMFORT scale;
- CHEOPS;
Table 1: CRIES scale for the postoperative pain assessment in neonates.4
| Parameer | 0 | 1 | 2 |
| Crying | No | High pitched | Inconsolable |
| Requires O2 for Sat>95 | No | <30% | 30% |
| Increased vital signs | HR and BP + or < than preoperative | HR or BP increased < 20% than preoperative | HR or BP increased >20% than preoperative |
| Expression | None | Grimace | Grimace/Grunt |
| Sleepless | No | Wakes at frequent intervals | Constantly awake |
COMFORT scale includes 6 behavioral items such as alertness, calmness, muscle tone, movement, facial tension, respiratory response for ventilated/crying for nonventilated and 2 physiological items such as heart rate and mean arterial blood pressure. It can be used at the age till 3 years for the assessment of postoperative and procedural pain.5,6 COMFORT scale is represented in the Table 2.5
Table 2. COMFORT scale for the assessment on postoperative and procedural pain
| Parameter | Assessment | Score |
| Alertness | · Deeply asleep (eyes closed no response to changes in the environment) · Lightly asleep (eyes mostly closed, occasional responses) · Drowsy (child closes his/her eyes frequently, less responsive to the environment · Awake and alert (child responsive to the environment) · Awake and hyper-alert (exaggerated responses to environmental stimuli) |
1 . 2 3 . 4 5 |
| Calmness/ Agitation | · Calm (child appears serene and tranquil) · Slightly anxious (child shows slight anxiety) · Anxious (child appears agitated but remains in control) · Very anxious (child appears very agitated, just able to control) · Panicky (severe distress with loss of control) |
1 2 3 4 5 |
| Respiratory response (Score only in mechanically ventilated children) |
· No spontaneous respiration · Spontaneous and ventilator respiration · Restlessness or resistance to ventilator · Actively breathes against ventilator or coughs regularly · Fights ventilator |
1 2 3 4 5 |
| Crying | · Quiet breathing, no crying sounds · Occasional sobbing or moaning · Whining (monotonous sound) · Crying · Screaming or shrieking |
1 2 3 4 5 |
| Physical movement | · No movement · Occasional (three or fewer) slight movements · Frequent, (more than three) slight movements · Vigorous movements limited to extremities · Vigorous movement including torso and head |
1 2 3 4 5 |
| Muscle tone | · Muscles totally relaxed; no muscle tone · Reduced muscle tone; less resistance than normal · Normal muscle tone · Increased muscle tone and flexion of fingers and toes · Extreme muscle rigidity and flexion of fingers and toes |
1 2 3 4 5 |
| Facial tension | · Facial muscles totally relaxed · Normal facial tone · Tension evident in some facial muscles (not sustained) · Tension evident throughout facial muscles (sustained) · Facial muscles contorted and grimacing |
1 2 3 4 5 |
CHEOPS (Children’s Hospital of Eastern Ontario Pain Scale) scale is a behavioral scale for the assessment of postoperative pain in young children. It includes the following parameters as cry, facial, child verbal, torso, touch, legs.7It can be used in children from 0 to 4 years.8 CHEOPS score ranges from 4 to 13, and additional interventions are required for the score above 6. CHEOPS is represented in the Table 3.
Table 3: CHEOPS for the pain assessment in young children
| Parameter | Assessment | Score |
| Cry | · no cry · moaning · crying · screaming |
1 2 2 3 |
| Facial | · smiling · composed · grimace |
0 1 2 |
| Child verbal | · positive · none · complaints other than pain · pain complaints · both pain and non-pain complaints |
0 1 1 2 2 |
| Torso | · neutral · shifting · tense · shivering · upright · restrained |
1 2 2 2 2 2 |
| Touch | · not touching · reach · touch · grab · restrained |
1 2 2 2 2 |
| Legs | · neutral · squirming kicking · drawn up tensed · standing · restrained |
1 2 2 2 2 |
FLACC (Face, Leg, Activity, Cry, and Consolability) tool can be used for the assessment of postoperative and periprocedural pain in children from 2 months to 7 years. It is represented in the Table 4.9
Table 4: FLACC tool for the postoperative and periprocedural pain assessment
| Categories | Scoring | ||
| 0 | 1 | 2 | |
| Face | No particular expression or smile | Occasional grimace or frown, withdrawn, disinterested | Frequent to constant quivering chin, clenched jaw |
| Legs | Normal position or relaxed | Uneasy, restless, tense | Kicking, or legs drawn up |
| Activity | Lying quietly, normal position, moves easily | Squirming, shifting back and forth, tense | Arched, rigid or jerking |
| Cry | No cry (awake or asleep) | Moans or whimpers; occasional complaint | Crying steadily, screams or sobs, frequent complaints |
| Consolability | Content, relaxed | Reassured by occasional touching, hugging or being talked to, distractable | Difficult to console or comfort. |
Children’s and Infant’s Postoperative Pain Scale (CHIPPS) is used for the assessment of postoperative pain in children from 0 to 5 years, where scores between 0 and 3 indicate the pain absence, and scores above 4 indicate a need for pain management. This scale is represented in the Table 5.10
Table 5: CHIPPS for the postoperative pain assessment
| Item | Structure | Points |
| Crying | · None · Moaning · Screaming |
0 1 2 |
| Facial expression | · Relaxed/smiling · Wry mouth · Grimace (mouth and eyes) |
0 1 2 |
| Posture of the trunk | · Neutral · Variable · Rear up |
0 1 2 |
| Posture of the legs | · Neutral, released · Kicking about · Tightened |
0 1 2 |
| Motor restlessness | · None · Moderate · Restless |
0 1 2 |
Neonatal Infant Pain Scale (NIPS) is used for the pain assessment in neonates. It includes facial expression, cry, breathing pattern, arms, legs, state of arousal, heart rate and O2 saturation. Score from 0 to 3 indicate absence or mild pain, 4-6 – moderate, 7-10 – severe. This scale is represented in the Table 6.11
Table 6: Neonatal Infant Pain Scale
| Variable | Finding | Points |
| Facial expression | · Relaxed (restful face, neutral expression) · Grimace (tight facial muscles, furrowed brow, chin, jaw) |
0 1 |
| Cry | · No cry (quiet, not crying) · Whimper (mild moaning, intermittent) · Vigorous crying (loud scream, shrill, continuous. If infant is intubated, score silent cry based on facial movement |
0 1 2 |
| Breathing pattern | · Relaxed (usual pattern for this infant) · Change in breathing (irregular, faster than usual, gagging, breath holding) |
0 1 |
| Arms | · Relaxed (no muscular rigidity, occasional random movements of arms) · Flexed/extended (tense, straight arms, rigid and/or rapid extension, flexion) |
0 1 |
| Legs | · Relaxed (no muscular rigidity, occasional random leg movements) · Flexed/extended (tense, straight legs, rigid and/or rapid extension, flexion) |
0 1 |
| State of arousal | · Sleeping/awake (quiet, peaceful, sleeping or alert and settled) · Fussy (alert, restless and thrashing) |
0 1 |
| Heart rate | · Within 10% of baseline · 11-20% of baseline · >20% of baseline |
0 1 2 |
| O2 saturation | · No additional O2 needed to maintain O2 saturation · Additional O2 required to maintain O2 saturation |
0 1 |
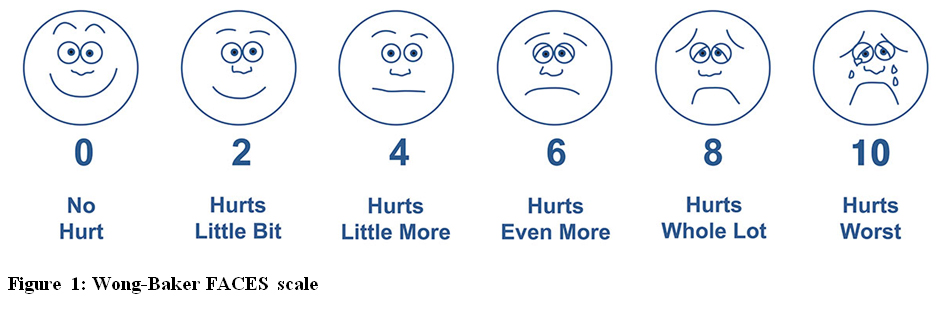
The most reliable indicator of pain is self-report by the patient, which us usually possible in children older than 4 years. At this age different pain rating scales can be used including the following:
- Wong-Baker FACES scale
- Faces scale of Bieri
- OUCHER Scale of Beyer and Wells
- Visual analog scale
- Verbal rating scale
Faces Pain Scale by Bieri is also used for the postoperative pain assessment in children older than 5 years. Training is necessary before using this scale. Faces Pain Scale by Bieri is represented at Figure 2.
OUCHER Scale of Beyer and Wells can be used in children above 3 years. Training of the child is also necessary before performing an assessment. OUCHER Scale of Beyer and Wells is represented in Figure 3.14
Different verbal report scales have also been used. There are 4-point15 to 15-point scales,16 which include different adjectives for describing pain from mild to severe.
Visual analog scale (VAS) is usually a 100-mm long horizontal line, which has labels of ‘No pain’ near one end and ‘Most severe pain imaginable’ at the other end, which requires from patient an ability to compare their pain sensation with the length of the line. Different scales are available online and one of them is represented at Figure 4.
Another way of postoperative pain assessment in children is Parent’s Postoperative Pain Measure (PPPM), which can be used in children from 2 years. It includes 15 questions about child’s behavior and activity. An answer for each question provides 1 score up to a maximum of 15. A score of 6 and more indicates clinically relevant pain.17
Unconscious or Sedated Patients
Pain assessment is a real problem in unconscious or sedated patients. For this purpose several methods have been described:
- Behavioral Pain Scale (BPS).
- Critical Care Pain Observation Tool (CPOT).
- Nonverbal Pain Scale (NVPS).
Table 7: Behavioral Pain Scale
| Variable | Finding | Point |
| Facial expression | · Relaxed · Partially tightened (e.g., brow lowering) · Fully tightened (e.g., eyelid closing) · Grimacing |
1 2 3 4 |
| Upper limb movements | · No movement · Partially bent · Fully bent with finger flexion · Permanently retracted |
1 2 3 4 |
| Compliance with mechanical ventilation | · Tolerating movement · Coughing but tolerating ventilation for most of the time · Fighting ventilator · Unable to control ventilation |
1 2 3 4 |
CPOT can be used for pain assessment in intubated and sedated patients based on facial expression, muscle tension and movement, compliance with ventilated breaths for intubated patients or vocalized pain in non-intubated patients. CPOT score of 2 and less indicates no or mild pain, scores above 2 indicates unacceptable level of pain, so further or alternative methods of analgesia should be considered. CPOT is represented at the Table 8.20
Table 8: Critical Care Pain Observation Tool
| Variable | Finding | Point |
| INTUBATED | ||
| Compliance with ventilator | · Tolerating ventilator or movement · Coughing but tolerating · Fighting ventilator |
0 1 2 |
| NOT INTUBATED | ||
| Vocalization | · Talking in normal tone or no sound · Sighing, moaning · Crying out, sobbing |
0 1 2 |
| Facial expression | · Relaxed, neutral · Tense · Grimacing |
0 1 2 |
| Body movements | · Absence of movements · Protection · Restlessness |
0 1 2 |
| Muscle tension | · Relaxed · Tense, rigid · Very tense or rigid |
0 1 2 |
NPS is used for pain assessment in nonverbal and intubated patients. It assesses facial expression, movements, guarding, vital signs, changes in respiration. Scores of ≤ 2 indicate no pain, 3-6 – moderate pain, ≥ 6 – severe pain; analgesia is required if score is 3 or higher. This scale is represented in the Table 9.21
Table 9: Nonverbal Pain Scale
| Variable | Finding | Point |
| Face | No particular expression or smile Occasional grimace, tearing, frowning, wrinkled forehead Frequent grimace, tearing, frowning, wrinkled forehead |
0 1 2 |
| Activity (movement) | Lying quietly, normal position Seeking attention through movement or slow, cautious movement Restless, excessive activity and/or withdrawal reflexes |
0 1 2 |
| Guarding | Lying quietly, no positioning of hands over areas of the body Splinting areas of the body, tense Rigid, stiff |
0 1 2 |
| Physiology (vital signs) | Baseline vital signs unchanged Change in SBP >20 mmHg or HR >20 bpm Change in SBP >30 mmHg or HR >25 bpm |
0 1 2 |
| Respiratory | Baseline RR / SpO₂ synchronous with ventilator RR >10 bpm over baseline, 5% decrease SpO₂ or mild ventilator asynchrony RR >20 bpm over baseline, 10% decrease SpO₂ or severe ventilator asynchrony |
0 1 2 |
Management:
The next step after the pain has been assessed and measured is treatment. Different approaches have been used in the provision of sufficient level of analgesia in the postoperative period depending on the intensity of pain the patient has. There was one big prospective study conducted, where the patients were asked to quantify their pain after 179 different surgical interventions.22 So that pain management should be based not only on the level of trauma after the operation, but also the intensity of pain that they experienced.
The less painful surgeries were: excision of solitary lymph nodes (cervical), prepuce surgery, skull and/or brain surgery, and testicular hydrocele surgery. Moderately painful operations were: open umbilical hernia repair, nephrectomy (lap), open inguinal hernia repair; subtotal hysterectomy, spinal canal decompression, and liver resection (atypical, open).
Very painful operations were: incisional hernia repair with alloplastic material, open subtotal hysterectomy, kidney transplantation, open cholecystectomy, tonsillectomy, and complex spinal reconstruction.
For operations, which cause less degree of pain the following measures can be used for the pain management presented in Table 10.23
Table 10: Pain management for less painful operations
| Levels | Intraoperative | Postoperative |
| Basic level | · Rectal NSAID or if not available rectal paracetamol.24,25 | · IV fentanyl or morphine · Oral NSAIDs and/or oral paracetamol in adequate dosing during the entire postoperative period.24,25 |
| Intermediate level | · Rectal NSAID or if not available rectal paracetamol | · IV fentanyl or morphine · IV nalbuphine.29 · Oral NSAIDs and/or paracetamol in adequate dosing during the entire postoperative period |
| Advanced level | · IV ketorolac (if available) or rectal NSAID.26
· IV loading dose of paracetamol.27 |
· IV fentanyl or morphine · IV nalbuphine · Oral NSAIDs and/or paracetamol in adequate dosing during the entire postoperative period |
For operations, which cause moderate amount of pain the following measures can be used for the pain management, presented in Table 11.23
Table 11: Pain management of moderately painful operations
| Levels | Intraoperative | Postoperative | ||
| Basic level | · Rectal NSAID or if not available rectal paracetamol.24,25 | · IV fentanyl or morphine · Oral NSAIDs and/or oral paracetamol in adequate dosing during the entire postoperative period.24,25 |
||
| Intermediate level | · Rectal NSAID or if not available rectal paracetamol · Caudal blockade with long-acting local anesthetics w or w/o clonidine if available.30 |
· IV fentanyl or morphine · IV nalbuphine.29 · Oral NSAIDs and/or paracetamol in adequate dosing during the entire postoperative period |
||
| Advanced level | · IV ketorolac (if available) or rectal NSAID.26
· IV loading dose of paracetamol.27 · Ultrasound-guided peripheral blocks, TAP, paravertebral or ultrasound-guided caudal blocked with long-acting local anesthetics combined with appropriate adjunct).31-33 |
· IV fentanyl or morphine · IV nalbuphine · Oral NSAIDs and/or paracetamol in adequate dosing during the entire postoperative period |
||
For operations, which cause severe pain the following can be used for the pain management, presented in Table 12.23
Table 12: Pain management of severely painful operations
| Level | Intraoperative | Postoperative |
| Basic level | · Intravenous fentanyl in divided doses · Rectal NSAID or if not available rectal paracetamol after induction of anesthesia or oral paracetamol or NSAID as a part of premedication.34 · Local wound infiltration by the surgeon of a long acting local anesthetic.35,36 |
· Intravenous fentanyl or morphine · Oral NSAIDs and/or oral paracetamol in adequate dosing during the entire postoperative period.24,25 · Intravenous or oral tramadol or other suitable agent.37 |
| Intermediate level | · Intravenous fentanyl in divided doses · Rectal NSAID or if not available rectal paracetamol after induction of anesthesia or oral paracetamol or NSAID as a part of premedication.34 · Local wound infiltration by the surgeon of a long acting local anesthetic.35,36 · Loading dose of tramadol or other suitable agent if available: nalbuphine, piritramide before the end of anesthesia. |
· Intravenous fentanyl or morphine · Oral NSAIDs and/or paracetamol in adequate dosing during the entire postoperative period · IV or oral tramadol or other suitable agent |
| Advanced level | · Intravenous fentanyl in divided doses or remifentanil infusion · Rectal NSAID or if not available rectal paracetamol after induction of anesthesia or oral paracetamol or NSAID as a part of premedication.34 · Loading dose of tramadol or other suitable agent if available: nalbuphine, piritramide before the end of anesthesia. |
· Intravenous fentanyl or other suitable agent · IV/oral paracetamol or IV/oral NSAID.38 · IV or oral tramadol or other suitable agent · Consider patient controlled regional anesthesia or IV-PCA if needed.39 |
CONCLUSION
Pain is an inevitable consequence of surgical interventions in children, which results in a lot of stress and discomfort not only to the patients, but also to their parents. The methods of pain assessment have been described and summarized in this article depending on the age of a child and his/her status of consciousness and ventilation. Different pain measurement tools utilize different information for the pain assessment, but their variable validity has been shown in many of the studies. All available methods should be used in routine clinical practice and guide the pain management throughout the patient’s stay in the hospital.
The pain intensity depends not only upon the level of trauma after the operation, but also the localization and character of procedure. So usually more traumatic surgeries cause more pain. That shows a relevance of the pain management according to the score of different pain scales.
We can utilize the recent guidelines for the pain management in children and group them up according to the level of postoperative pain for ready reference.
Conflict of interest: None declared by the author.
REFERENCE
- International association for the study of Pain. IASP Taxonomy. Available at http://www.iasp-pain.org/Education/Content.aspx?ItemNumber=1698#Pain. Accessed at: June 18,2018.
- Gan TJ. Poorly controlled postoperative pain: prevalence, consequences, and prevention. J Pain Res. 2017;10:2287-2298. DOI: 2147/JPR.S144066 [PubMed]
- Mathews L. Pain in children: neglected, unaddressed and mismanaged. Indian J Palliat Care. 2011;17(Suppl):S70-S73. DOI: 4103/0973-1075.76247 [PubMed]
- Krechel SW, Bildner J. CRIES: a new neonatal postoperative pain measurement score. Initial testing of validity and reliability. Paediatr Anaesth. 1995;5(1):53-61. DOI: 1111/j.1460-9592.1995.tb00242.x [PubMed]
- Ambuel B, Hamlett KW, Marx CM, Blumer JL. Assessing distress in pediatric intensive care environments: the COMFORT scale. J Pediatric Psychol. 1992;17(1):95-109. [PubMed]
- van Dijk M, de Boer JB, Koot HM, Tibboel D, Passchier J, Duivenvoorden HJ. The reliability and validity of the COMFORT scale as a postoperative pain instrument in 0 to 3-year-old infants. Pain. 2000;84(2-3):367-377. [PubMed] [Free Full Text]
- McGrath PJ, Johnson G, Goodman JT, et al. CHEOPS: a behavior scale for rating postoperative pain in children. In: Fields H, Dubner R, Cervero F, editors. Advances in pain research and therapy. New York: Raven Press; 1985. pp. 395–402.
- Mitchell P. Understanding a young child's pain. Lancet. 1999; 354(9191):1708. DOI: 1016/S0140-6736(05)76696-4 [PubMed]
- Merkel SI, Voepel-Lewis T, Shayevitz JR, Malviya S. The FLACC: a behavioral scale for scoring postoperative pain in young children. Pediatr Nurs. 1997;23(3):293-7. [PubMed]
- Büttner W, Finke W. Analysis of behavioural and physiological parameters for the assessment of postoperative analgesic demand in newborns, infants and young children: a comprehensive report on seven consecutive studies. Paediatr Anaesth. 2000;10(3):303-18. [PubMed]
- Lawrence J, Alcock D, McGrath P, Kay J, MacMurray SB, Dulberg C. The development of a tool to assess neonatal pain. Neonatal Netw. 1993;12(6):59-66. [PubMed]
- Jacox A, Carr DB, Payne R, et al. Clinical Practice Guideline Number 9: Management of Cancer Pain. Rockville, MD: Agency for Health Care Policy and Research, US Department of Health and Human Services; 1994. AHCPR publication 94-0592.
- Wong DL, Baker CM. Pain in children: comparison of assessment scales. Pediatr Nurs. 1988;14(1):9-17. [PubMed] [Free Full Text]
- Beyer JE, Wells N. The assessment of pain in children. Pediatr Clin North Am. 1989;36(4):837–854. [PubMed]
- Seymour RA. The use of pain scales in assessing the efficacy of analgesics on postoperative dental pain. Eur J Clin Pharmacol. 1982;23(5):441-4. [PubMed]
- Gracely RH, McGrath P, Dubner R. Validity and sensitivity of ratio scales of sensory and affective verbal descriptors: manipulation of affect by diazepam. Pain. 1978;5(1):19-29. [PubMed]
- Chambers CT, ReidGJ, McGrath PJ, Finley GA. Development and preliminary validation of a postoperative pain measure for parents. Pain. 1996;68(2-3):307-313. [PubMed]
- Payen JF1, Bru O, Bosson JL , Lagrasta A, Novel E, Deschaux I, et al. Assessing pain in critically ill sedated patients by using a behavioral pain scale. Crit Care Med. 2001;29(12):2258-63. [PubMed]
- Ahlers SJ, van der Veen AM, van Dijk M, Tibboel D, Knibbe CA. The use of the behavioral pain scale to assess pain in conscious sedated patients. Anesth Analg. 2010;110(1):127-33. DOI: 1213/ANE.0b013e3181c3119e [PubMed]
- Gélinas C, Fortier M, Viens C, Fillion L, Puntillo Kl. Pain assessment and management in critically ill intubated patients: a retrospective study. Am J Crit Care. 2004;13(2):126-35. [PubMed] [Free Full Text]
- Odhner M, Wegman D, Freeland N, Steinmetz A, Ingersoll GL. Assessing pain control in nonverbal critically ill adults. Dimens Crit Care Nurs. 2003;22(6):260-7. [PubMed]
- Gerbershagen HJ, Aduckathil S, van Wijck AJM, Peelen LM, Kalkman CJ, Meissner W. Pain intensity on the first day after surgery: a prospective cohort study comparing 179 surgical procedures. Anethesiology. 2013;118(4):934-44. DOI: 1097/ALN.0b013e31828866b3 [PubMed]
- Vittinghoff M, Loonnqvist PA, Mossetti V, Heschl S, Simic D, Colovic V, et al. Postoperative pain management in children: guidance from the pain committee of the european society for paediatricanaesthesiology (espa pain management ladder initiative). Pediatr Anesth. 2018;28(6):493-506. DOI: 1111/pan.13373 [PubMed]
- Pierce CA, Voss B. Efficacy and safety of ibuprofen and acetaminophen in children and adults: a meta-analysis and qualitative review. Ann Pharmacother. 2010;44(3):489-506. DOI: 1345/aph.1M332 [PubMed]
- Walther-Larsen S, Aagaard GB, Friis SM, Petersen T, Møller-Sonnergaard J, Rømsing J. Structured intervention for management of pain following day surgery in children. Pediatr Anesth. 2016;26(2):151-157. DOI: 1111/pan.12811 [PubMed]
- Hong J-Y, Won Han S, Kim WO, Kil HK. Fentanyl sparing effects of combined ketorolac and acetaminophen for outpatient inguinal hernia repair in children. J Urol. 2010;183(4):1551-5. DOI: 1016/j.juro.2009.12.043 [PubMed]
- McNicol ED, Ferguson MC, Haroutounian S, Carr DB, Schumann R. Single dose intravenous paracetamol or intravenous propacetamol for postoperative pain. Cochrane Database Syst Rev. 2016;(5):CD007126. DOI: 1002/14651858.CD007126.pub3 [PubMed]
- Duedahl TH, Hansen EH. A qualitative systematic review of morphine treatment in children with postoperative pain. Paediatr Anesth. 2007;17:756-74. DOI: 1111/j.1460-9592.2007.02213.x [PubMed]
- Schnabel A, Reichl SU, Zahn PK, Pogatzki-Zahn E. Nalbuphine for postoperative pain treatment in children. Cochrane Database Syst Rev. 2014;(7):CD009583. DOI: 1002/14651858.CD009583.pub2 [PubMed]
- Amminnikutty CM, Karthik A, Kodakkat AK. Postoperative analgesia in pediatric herniotomy - comparison of caudal bupivacaine to bupivacaine infiltration with diclofenac suppository. Anesth Essays and Res. 2016;10(2):250-4. DOI: 4103/0259-1162.172332 [PubMed]
- Weintraud M, Lundblad M, Kettner SC, Willschke H, Kapral S, Lönnqvist PA, et al. Ultrasound versus landmark-based technique for ilioinguinal-iliohypogastric nerve blockade in children: the implications on plasma levels of ropivacaine. Anesth Analg. 2009;108(5):1488-92. DOI: 1213/ane.0b013e31819cb1f3 [PubMed]
- Sahin L, Sahin M, Gul R, Saricicek V, Isikay N. Ultrasound-guided transversus abdominis plane block in children: a randomised comparison with wound infiltration. Eur J Anaesthesiol. 2013;30(7):409-414. DOI: 1097/EJA.0b013e32835d2fcb [PubMed]
- Bhalla T, Sawardekar A, Dewhirst E, Jagannathan N, Tobias JD. Ultrasound-guided trunk and core blocks in infants and children. J Anesth. 2013;27(1):109-123. DOI: 1007/s00540-012-1476-5 [PubMed]
- El-Fattah AM, Ramzy E. Pre-emptive triple analgesia protocol for tonsillectomy pain control in children: double-blind, randomised,controlled, clinical trial.J Laryngol Otol. 2013;127(4):383-391. DOI: 1017/S0022215113000364 [PubMed]
- Ecoffey C. Safety in pediatric regional anesthesia. Paediatr Anesth. 2012;22(1):25-30. DOI: 1111/j.1460-9592.2011.03705.x [PubMed]
- Ju NY, Cui GX, Gao W. Ropivacaine plus dexamethasone infiltration reduces postoperative pain after tonsillectomy and adenoidectomy.Int J Pediatr Otorhinolaryngol. 2013;77(11):1881-5. DOI: 1016/j.ijporl.2013.08.037 [PubMed]
- Schnabel A, Reichl SU, Meyer-Frießem C, Zahn PK, Pogatzki-Zahn E. Tramadol for postoperative pain treatment in children. Cochrane Database Syst Rev. 2015;(3):CD009574. DOI: 1002/14651858.CD009574.pub2 [PubMed]
- Southworth S, Peters J, Rock A, Pavliv L. A multicenter, randomized, double-blind, placebo- controlled trial of intravenous ibuprofen 400 and 800 mg every 6 hours in the management of postoperative pain. Clin Ther. 2009;31(9):1922-35. DOI: 1016/j.clinthera.2009.08.026 [PubMed]
- Morton NS, O’Brien K. Analgesic efficacy of paracetamol and diclofenac in children receiving PCA morphine. Br J Anaesth.1999; 82(5):715-7. [PubMed] [Free Full Text]