Roshdi R. Al-metwalli*
*Associate Professor, Department of Anesthesiology and Intensive Care, University of Dammam, Al-Khobar (Saudi Arabia)
Correspondence: Roshdi R. Al-metwalli, University of Dammam, King Fahad Hospital, PO Box 40081, Al-Khobar, Post Code 31952 (Saudi Arabia); Tel: 00966 38 98 2219; Fax: 00966 8966770; E-mail: rmetwalli@yahoo.com
ABSTRACTAim:To evaluate the use of perfusion index for diagnosis of abnormal collateral hand circulation (CHC), in comparison with the modified Allen test and pulse oximetry using Doppler ultrasonography as a reference test.
Methodology: Forty two (84 hands) healthy volunteers were randomly selected for our study. Adequacy of the collateral hand circulation during occlusion of the radial artery was assessed in each hand using four tests by four expert investigators, one for each test: (I) Modified Allen test (2) Perfusion index (3) Pulse oximetry, and (4) Doppler ultrasonography being the standard test.
Results: The Doppler ultrasonography (the standard test) diagnosed abnormal CHC in 3 hands (3.5%). The modified Allen test showed abnormal CHC in 16 hands (19%), with sensitivity100%, specificity 78% and positive predictive value 18.7% when compared with the standard Doppler ultrasonography. Also pulse oximetry method indicated abnormal CHC in 4 hands (4.7%) with sensitivity100% specificity 98% and 75% positive predictive value. ROC analysis showed that > 65.7% reduction in the perfusion index diagnosed abnormal CHC with 100% sensitivity, 98.8% specificity and 75.5% positive predictive value using Doppler ultrasonography as a reference test.
Conclusion: Using Doppler ultrasonography as a reference test, perfusion index is a reliable objective test for diagnosis and prediction of abnormal CHC, with high sensitivity, specificity, and accepted positive predictive value.
Keywords: Perfusion index; Modified Allen test; Collateral circulation; Doppler ultrasonography
Citation:Al-metwalli RR. Perfusion Index as an Objective Alternative to the Allen Test, with Flow Quantification and Medico legal Documentation. Anaesth Pain & Intensive Care 2014;18(3):245-249
INTRODUCTIONAllen test (AT)1 is the simplest and most practical method to assess collateral hand circulation (CHC) before radial artery (RA) cannulation and serial arterial blood sampling.2-4 It is also routinely used for selecting patients for radial artery harvesting,5-7 either for coronary artery bypass grafting8 or for the construction of a radio cephalic arteriovenous fistula for hemodialysis.9 Nevertheless, it is a subjective and not a quantifiable test, with high false positive results10 and without clearcut-off points between positive and negative tests.11 In addition, the consequences of a false-negative AT may be severe after RA harvesting12 and even catheterization,13 in terms of both clinical outcome and medico-legal issues. A peripheral perfusion index (PI), which is the ratio between the pulsatile and non-pulsatile component of the pulse oximetry signal, has been found to be a reliable indicator of peripheral perfusion.14There was, however, as far as we know, no previous study which used PI to assess CHC. The present study was designed to evaluate the changes in PI as an objective, noninvasive assessment of CHC, in comparison to the standard Doppler ultrasonography test, as well as the modified Allen test (MAT) and the pulse oximetry test.
METHODOLOGY
Following our institutional ethics committee approval and obtaining written informed consent, forty two healthy (operating room’s staff) volunteers, 22 males and 20 females, age range 23 to 44 years, were randomly selected. Both dominant and non-dominant (84) hands were studied. Colleagues with a history of peripheral vascular diseases, previous radial artery cannulation in either hand, or trauma to the upper limbs were excluded. They were advised not to smoke or consume caffeine 3 hours prior to the examination. They were examined at room temperature (20° to 22°C) and asked to rest supine for 10 minutes with their head and shoulders comfortably elevated, with their forearms and hands positioned at the level of the heart, and to remove or loosen any tight clothing from around their arms. Adequacy of the CHC during occlusion of the radial artery was assessed in each hand using four tests by four independent expert investigators. Each investigator was assigned to perform only one of these four tests and was blinded to the other investigators findings. The first hand tested (right or left) was randomly assigned.
Modified Allen's test (MAT): The subjects were instructed not to hyperextend their fingers or wrist. The examiner applied three digits (index, middle and ring fingers) compression to both the radial and ulnar arteries at the wrist, and the subject was asked to clench and relax his hand three times to exsanguinate the palm. The hand was then slowly opened to a neutral position, and the examiner removed pressure from the ulnar artery. The time taken (in seconds) for the blanched hand to return to its normal color, was recorded. If it took longer than 10 seconds, the test was considered positive (abnormal CHC).
Pulse oximetry guided Allen’s test (POAT): The pulse oximetry sensor [LNCS adult adhesive sensors connected to Masimo SET”Radical [TM] pulse oximeters; Masimo Corp. Irvine. CA] was fixed to tip of the thumb of the selected hand. Baseline O2 saturation was noted. While conducting the above procedure the radial and ulnar arteries compressions were sustained until the oxygen saturation reading fell to zero. The pressure on the ulnar artery was then released and the time for the oxygen saturation to return to the baseline value was recorded. Failure of the oxygen saturation to return to baseline within 10 seconds indicated a positive test (abnormal CHC).
Perfusion Index Test (PI): With the pulse oximetry sensor still fixed to the thumb of the same hand, another independent investigator recorded the baseline perfusion index (PI) value (the ratio between the pulsatile and non-pulsatile component of the pulse oximetry signal), and repeated the same technique used above for Allen’s test examination. He recorded the PI value at 10 seconds after pressure on the ulnar artery was released (the same cut-off point between negative and positive Allen test) and calculated the percentage reduction from its baseline value.
Doppler ultrasonography study: The flow in the dorsal digital thumb artery (TA) located at the ulnar side of the base of the thumb was examined using Doppler ultrasound digital probe (Bidop® 3 Vascular Ultrasound Doppler, Koven Technology, Inc. Canada ). Doppler probe was placed over the expected anatomic position of TA and aligned with it at an angle of less than 60°. By moving the probe from side to side across the vessel, the center of the artery could be located readily by a characteristic noise produced at the frequency of the pulse rate. When a steady state was achieved, the RA was firmly compressed. Complete disappearance of both the Doppler tracing (waves) and the characteristic noise, indicated zero flow and positive test (abnormal CHC).
Our primary outcome was to evaluate the efficacy and reliability of PI changes as a new objective test, in diagnosis and prediction of abnormal CHC, when it is compared with MAT and POAT using Doppler ultrasonography test as reference test.
Statistics:
We assumed that PI changes will have 30% increase in the prediction ability (PPV) to diagnose abnormal CHC than the previously recorded prediction value of MAT (42%)15 . At a significance level of 0.05 with power of 80%, a total of 78 volunteers were required. Receiver Operating Characteristic (ROC) curve was analyzed using Doppler ultrasonography study as reference, to determine the percentage reduction of PI which represent the cut-off point or criterion value which discriminated between normal and abnormal CHC, and to derive the sensitivity, specificity, positive & negative predictive values using, MedCalc version 12 (MedCalc Software bvba, Mariakerke, Belgium ). On the other hand both MAT and the POAT were evaluated by applying the criteria for the assessment of diagnostic tests ( sensitivity, specificity, positive and negative predictive values, and diagnostic accuracy) (16,17) using Doppler ultrasonography study as reference.
RESULTS
Twenty two males and 20 females (mean age 35.2 years, range 23 to 44 years) were studied (84 hands). The following are the summary of the results of four tests.
Doppler ultrasound test (reference test): Three hands (3.5%) had zero flow in the dorsal digital TA during radial artery compression, and were judged to have an abnormal CHC (bilateral in one male volunteer and unilateral in anther male volunteer).
MAT: Sixty eight hands (81%) had normal ulnar collateral circulation with the mean time for revascularization = 4.1±3.5 sec and 16 hands (19%) had abnormal CHC with mean revascularization time = 12.0±1.9 sec. When compared with the Doppler ultrasound, this test had 100% sensitivity, 78% specificity and 18.7% positive predictive value (Table 1).
Table 1: Comparison of Allen's test with Doppler ultrasound (Gold standard)|
Doppler ultrasound outcome |
Predictive value |
||
|
Condition Positive (Abnormal) |
Condition Negative (Normal) |
||
| MAT +ve |
3 |
13 |
18.7% PPV |
| MAT -ve |
0 |
68 |
100% NPV |
|
Sensitivity: 100% |
Specificity: 83.9% |
84.5% DA |
|
MAT= Modified Allen’s test. PPV= Positive predictive Value.
NPV= Negative predictive Value. DA= Diagnostic accuracy
POAT: Four hands (4.7%) had abnormal CHC (failed to restore their baseline oxygen saturation within 10 sec after the release of ulnar artery compression). When compared with the reference test (Dopplerultrasound), this test had 100% sensitivity, 98% specificity and 75% positive predictive value (Table 2).
Table 2: Comparison of Pulse oximetry with Doppler ultrasound (Gold standard)|
Doppler ultrasound outcome |
Predictive value |
||
|
Condition Positive (Abnormal) |
Condition Negative (Normal) |
||
|
POAT +ve |
3 |
1 |
75% PPV |
|
POAT -ve |
0 |
80 |
100% NPV |
|
Sensitivity: 100% |
Specificity: 98.7% |
98.8% DA |
|
POAT= Pulse oximetry guided Allen’s test. PPV= Positive predictive Value.
NPV= Negative predictive Value. DA= Diagnostic accuracy
PI: ROC analysis of PI changes using Doppler study as reference showed that; 65.7% reduction in PI (after 10 sec radial artery compression) represents the cut-off point or criterion value above which abnormal CHC was diagnosed. This test has 100% sensitivity, 98.8% specificity, 75.5% and 100% positive and negative predictive values respectively (Figure 1).
Figure 1: ROC curve comparing percentage reduction in perfusion index with the standard Doppler ultrasound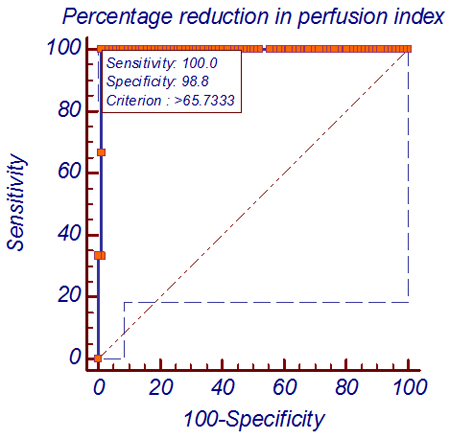
DISCUSSION
This is the first prospective, randomized, controlled study which usedPI to diagnose abnormal CHC .We reported that the PI is a relative value with a wide normal range [median= 2.75 with interquartile range (IQR) =1.4-4.3] which confirmed the results of Lima et al14 [median PI of 1.4 with (IQR) = 0.3-3].This means that there is no absolute normal PI value, but each patient has his unique PI.
Using (ROC) curve analysis and Doppler ultrasonography as a reference test, our study showed that, 65.7% reduction in PI (after 10 sec radial artery compression) represents the cut-off point or criterion value above which abnormal CHC was diagnosed. In comparison to the same reference test this test was analogous to POAT with high sensitivity, specificity and positive predictive values. , and was superior to MAT regarding specificity, and positive predictive values. (Table 1, 2. Fig.1)
In our study when we compared the MAT with the standard Doppler ultrasonography test, we found the MAT had a sensitivity of 100%, specificity of 84%, and very low PPV (18.7 %) i.e., 81.3% of all abnormal MAT results in our study were incorrect. These results are similar to several previous studies 15,18,19. Its high sensitivity, confirm its reliability as a screening test for the selection of patients for RA interventions. In the other hand its low PPV validate the major argument against its routine use for evaluation of CHC.4,20,21 From the available literature, there is no consensus regarding the MAT cut-off point (time for revascularization) and was varied between 5 and 15 sec in different reports.22-25 Accordingly the incidence of positive (abnormal) MAT was also varied between 1% and 27%.22-25 We chose to set the MAT cut-off point to 10 sec as midway between the reported ranges and therefore our incidence (19 %) was within the reported values.
In the present study, we used Doppler ultrasonography as the "gold standard" test for evaluation of CHC, because the reliability of Doppler ultrasonography for identifying patients with an abnormal CHC has already been demonstrated by previous anatomical,26 arteriographic,27 and clinical studies by Kamienski10 Mozersky28 and Ruengsakulrach et al19. There are no established standard criteria for Doppler ultrasound findings that define abnormal hand collateral perfusion which vary from study to study, depending on which vessels are scanned.10,19,29-33 In our present study we chose to test the flow in the dorsal digital thumb artery based on the conclusion of Ruengsakulrach et al19 (no flow in the dorsal digital thumb artery with radial artery occlusion is the sole absolute contraindication for radial artery harvest). Furthermore, our results were similar to their outcomes regarding the comparison with MAT (Table 1).
In comparison with the standard Doppler ultrasonography, our results clearly showed that POAT has been found to have the same sensitivity (100%) as the MAT but, has higher specificity (98.7% vs 83.9%), PPV (75% vs. 18.7% ) and D. accuracy (98.8% vs. 84.5% ). Our results confirm the results of Johnson et al,6 and many other previous studies,11,34-38 who validated the reliability of an oxygen saturation monitor for safe harvesting of radial artery. Controversially, G. David et al reported falsely normal results with the use the pulse oximeter Allen's test and concluded that, pulse oximeter do not seem to be accurate in assessing hand collateral circulation . This controversially, could be explained by the difference in the study methodologies and /or the difference in the reference test. Furthermore, because blood flows as low as 4%–9% of baseline are associated with normal pulse oximetry values. Thereafter; the return of baseline pulse oximetry saturation after release of RA occlusion may not ensure adequate tissue perfusion and could over diagnose normal hand circulation.39 Despite this theoretical concern,35 the Modified Allen’s Test using pulse oximetry has been used for selection of patients for radial artery harvest with no instance.11,34-38
LIMITATIONSOne of the limitation to our study was that all subjects enrolled in the study were normal healthy volunteers, who had healthy peripheral vessels which may react differently (after RA compression) than the vessels of critically ill patients who are the ones generally requiring RA intervention. Thus a study on this high risk population is warranted. A second limitation was that PI is a dynamic parameter (like ECG) which fluctuates with sudden internal or external stress, which should always be eliminated as much as possible.
CONCLUSIONUsing Doppler ultrasonography as reference test, > 65.7% reduction in perfusion index after 10 second radial artery compression provides a reliablequantifiable diagnosis of abnormal CHC, with sensitivity, specificity, and positive predictive value higher than MAT but comparable to POAT. Furthermore; as PI is incorporated with pulse oximetry in the same monitor, the use of both facilities to evaluate CHC, will add additional confirmation and medico legal documentation.
Acknowledgments:We thank all members of the Department of Anesthesia in King Fahad Hospital, Al-Khobar, Saudi Arabia, with special thanks to Dr. A Khider, Dr. A Sidiqui, Dr. M Shafi and Mr. A Taha for their encouragement and help in the clinical work.
REFERENCES- Allen EV. Thromboangitis obliterans: methods of diagnosis of chronic occlusive arterial lesions distal to the wrist with illustrative cases. Am J Med Sci 1929; 178:237-44
- Hug CC. Monitoring. In: Miller RD (Ed). Anesthesia. New York: Churchill Livingstone 1986:411.
- Ream AK. Monitoring techniques and concepts, In: Ream AK, Fogdall RP (Eds). Acute cardiovascular management; anesthesia and intensive care. Philadelphia, JB Lippineon, 1982: 139.
- Wilkins RG. Radial artery, cannulation and ischaemic damage: a review. Anaesthesia 1985; 40: 896-9. [PubMed]
- Hlozek CC, Zacharias WM, Mizener KA. RN First assistants expand their perioperative role. AORN J. 1998;67:560-6. [PubMed]
- Johnson WH, Cromartie RS, Arrants JE, Wuamett JD, Holt JB . Simplified method for candidate selection for radial artery harvesting. Ann Thorac Surg 1998; 65:1167. [PubMed]
- Sajja LR, Mannam MG, Sompalli S.. Is Allen’s test not reliable in the selection of patients for radial artery harvest? Ann Thorac Surg 2002; 74:296. [PubMed]
- Meharwal ZS, Trehan N. Functional status of the hand after radial artery harvesting: results in 3,977 cases. Ann Thorac Surg 2001;72:1557–61. [PubMed]
- Shibahara T, Noma H, Ichinohe T, Kaneko Y. Blood flow monitoring by pulse oximetry during a forearm flap elevation. Bull Tokyo Dent Coll 1999;40:181–5. [PubMed]
- Kamienski RW, Barnes RW. Critique of the Allen test for continuity of the palmar arch assessed by Doppler ultrasound. Surg Gynecol Obstet 1976;142:861-4. [PubMed]
- Greenhow DE. Incorrect performance of Allen’s test—ulnar artery follow erroneously presumed inadequate. Anesthesiology 1972;37:356–7. [PubMed][Free Full Text]
- Nunoo M J. An unexpected complication after harvesting of the radial artery for coronary artery bypass grafting. Ann Thorac Surg 1998;66:929-31. [PubMed]
- Baker RJ, Chunprapaph B, Nyhus LM. Severe ischemia of hand following radial artery catheterization. Surgery 1976;80:449-57. [PubMed]
- Lima AP, Beelen P, Bakker J. Use of a peripheral perfusion index derived from the pulse oximetry signal as a noninvasive indicator of perfusion.Crit Care Med. 2002;30:1210-3. [PubMed]
- Vaghadia H, Schechter MT, Sheps SB, Jenkins LC. Evaluation of a postocclusive reactive circulatory hyperaemia (PORCH) test for the assessment of ulnar collateral circulation. Can J Anaesth 1988;35:591–8. [PubMed]
- Sheps SB, Schechler MT. Assessment of diagnostic tests. JAMA 1984;252:2418-22. [PubMed]
- Schechler MT, Sheps SB. Diagnostic testing revisited: Pathways through uncertainly. Can Med Assoc J 1985;13:755-60. [PubMed][Free Full Text]
- Mangano DT, Hickey RF. Ischemic injury following uncomplicated radial artery catheterization. Anesth Analg 1979;58:55–7. [PubMed]
- Ruengsakulrach P, Brooks M, Hare DL, Gordon I, Buxton BF. Preoperative assessment of hand circulation by means of Doppler ultrasonography and the modified Allen test. J Thorac Cardiovasc Surg 2001;121:526–31. [PubMed]
- Slogoff S, Keats AS, Arlund C. On the safety of radial artery cannulation. Anesthesiology 1983;59:42–7. [PubMed][Free Full Text]
- McGregor A. The Allen test: an investigation of its accuracy by fluorescein angiography. J Hand Surg 1986;12:82–5. [PubMed]
- Campeau L. Percutaneous radial artery approach for coronary angiography. Cathet Cardiovasc Diagn 1989;16:3–7. [PubMed]
- Bedford RF, Wollman H. Complications of percutaneous radial artery cannulation: an objective prospective study in man. Anaesthesiology 1973;38:228–36. [PubMed][Free Full Text]
- Benit E, Vranckx P, Jaspers L, Jackmaert R, Poelmans C, Coninx R. Frequency of a positive modified Allen’s test in 1,000 consecutive patients undergoing cardiac catheterization. Cathet Cardiovasc Diagn 1996;38:352–4. [PubMed]
- Peters KR, Chapin JW. Allen’s test: positive or negative. Anesthesiology 1980;53:85.
- Coleman SS, Anson BJ. Arterial patterns in the hand based upon a study of 650 specimens. Surg Gynecoi Obstet 1961; 113: 409-24. [PubMed]
- Bolas P, Katsogiannis A, Katswtis P, Karaitianos J. Comparative study of evaluation of digital arterial circulation by Doppler ultrasonic tracing and hand arteriography. J Cardiovas Surg 1980; 21: 455-62. [PubMed]
- Mozersky D J, Buckley C J, Hagood CO, Capps WF, Dannemiller FJ. Ultrasonic evaluation of the palmar circulation : a useful adjunct to radial artery cannulation. AmJ Surg 1973; 126:810- 12. [PubMed]
- Doscher W, Viswanathan B, Stein T, Margolis IB. Physiologic anatomy of the palmar circulation in 200 normal hands. J Cardiovasc Surg (Torino) 1985;26:171–4. [PubMed]
- Doscher W, Viswanathan B, Stein T, Margolis IB. Hemodynamic assessment of the circulation in 200 normal hands. Ann Surg 1983;198:776–9. [PubMed]
- Pola P, Serricchio M, Flore R, Manasse E, Favuzzi A, Possati GF. Safe removal of the radial artery for myocardial revascularization: a Doppler study to prevent ischemic complications to the hand. J Thorac Cardiovasc Surg 1996;112:737–44. [PubMed]
- Agrifoglio M, Dainese L, Pasotti S, Galanti A, Cannata A, Roberto M, Parolari A, Biglioli P. Preoperative assessment of the radial artery for coronary artery bypass grafting: is the clinical Allen test adequate? Ann Thorac Surg 2005;79:570–2. [PubMed]
- Kochi K, Orihashi K, Sueda T. The snuffbox technique: a reliable color Doppler method to assess hand circulation. J Thorac Cardiovasc Surg 2003;125:821–5. [PubMed]
- Cheng EY, Lauer KK, Stummel KA, et al. Evaluation of palmar circulation by pulse oximetry. J Clin Monit 1989;5:1–3. [PubMed]
- Fuhrman TM, Pippin WD, Talmage LA, et al. Evaluation of collateral circulation of the hand. J Clin Monit 1992;8:28–32. [PubMed]
- Rozenberg B, Rozenberg M, Birkhan J. Allen’s test performed by pulse oximeter. Anaesthesia 1988:515–6. [PubMed]
- Nowak GS, Moorthy SS, McNiece WL. Use of pulse oximetry for assessment of collateral arterial flow. Anaesthesiology 1986;64:527. [PubMed][Free Full Text]
- Pillow K, Herrick IA. Pulse oximetry compared with Doppler ultrasound for assessment of collateral blood flow to the hand. Anaesthesia 1991;46:388–90. [PubMed]
- Lawson D, Norley I, Korbon G, Loeb R, Ellis J. Blood flow limits and pulse oximeter signal detection. Anesthesiology 1987;67:599–603. [PubMed][Free Full Text]