*Presently working as Medical Officer at Community Health Centre, Jalore, Rajasthan (India)
**Senior Resident, Department of Anesthesiology, AIIMS, Jodhpur (India)
***Profeesor of Anesthesiology, Dr. S N Medical College, Jodhpur, Rajasthan (India)
Correspondence: Dr. Priyanka Sethi, Department of Anesthesiology, Dr. S N Medical College, Jodhpur, Rajasthan (India); Tel: +91-9352206300; E-mail: dr.priyanka_sethi@yahoo.co.in
ABSTRACT
Background: This study was done to compare the heart rate (HR), systolic blood pressure (SBP), diastolic blood pressure (DBP), mean arterial pressure (MAP), ephedrine requirement and neonatal outcome between normotensive and severe pre-eclamptic women undergoing caesarean section under spinal anaesthesia.
Methodology: We enrolled a total of 30 healthy (control group) and 30 severe pre-eclamptic (BP > 160/110 mmHg) parturients (study group) above 18 years of age, undergoing elective cesarean section in the study. After preloading with 10 ml/kg of ringer lactate solution spinal anesthesia was administered with 12.5 mg of hyperbaric bupivacaine. SBP, DBP, MAP and HR were recorded before spinal anesthesia and at every 2 min intervals after spinal anesthesia for the first 20 min, and then after every 5 min till completion of surgery. Ephedrine was administered in 5 mg bolus dose when MAP decreased more than 20% of base line. Apgar score was noted at 1 and 5 min after birth. Hemodynamic variables were also noted four hourly in post-operative period for 24 hours in both of the groups.
Results: The blood pressure records were statistically lower at all intervals throughout the study in normotensive group as compared to pre-eclamptic group. The number of episodes of hypotension was more in normotensive group as compared to pre-eclamptic group and the result was statistically significant (p < 0.05). The mean ephedrine requirement in the normotensive group (13.4 ± 7.66 mg) was significantly more (P-value0.0005) than in pre-eclamptic group (6.6 ± 6.75 mg). Apgar scores at 1 and 5 min after birth were comparable in both of the groups.
Conclusion: Pre-eclamptic patients had less hypotension after spinal anesthesia, required less ephedrine than normotensives but had comparable fetal Apgar scores.
Keywords: Spinal anesthesia; Pre-eclampsia; Cesarean section; Ephedrine; Hypotension
Citation: Khatri RK, Sethi P, Ujawal S. Perioperative hemodynamic response and vasopressor requirement during spinal anesthesia for cesarean section in healthy and severe preeclamptic parturients: a prospective cohort comparison. Anaesth Pain & Intensive Care 2014;18(2):152-56
INTRODUCTION
Pre-eclampsia is a major cause of maternal and perinatal fetal mortality in the developing countries.1 These patients have an increased rate of cesarean section due to high incidence of fetal distress and intrauterine growth restriction.
General anesthesia is considered for cesareans when regional anesthetic techniques are contraindicated, especially in patients with severe pre-eclampsia, because of increased risks associated with potential failed intubation and difficult airway.2 There are more chances of aspiration pneumonitis, exaggerated hypertensive response to laryngoscopy and intubation and enhanced sensitivity to non-depolarizing muscle relaxants (NDMR) due to interactions between magnesium and NDMRs. 3
In preeclamptic patients regional technique are considered to be relatively safety as compared to general anesthesia. In current clinical practicesepidural anesthesia is generally preferred. Spinal anesthesia has again gained some popularity. Although it is commonly believed that a sudden and extensive sympathetic blockade following spinal anesthesia will result in severe hypotension, which would lead to placental hypoperfusion and fetal asphyxia. Spinal anesthesia has recently been used as the first choice of anesthetic technique in severe pre-eclamptic patients for cesarean section,4-7 yet very few published reports regarding this use in pre-eclamptic patients are available.
Better control of the perioperative hemodynamic changes can lead to reduction in perioperative morbidity and mortality in obstetric patients 8. Our aim was to compare the hemodynamic effects of spinal anesthesia in patients with severe preeclampsia and healthy parturient posted for cesarean section and to know amount of ephedrine consumption in pre-eclamptic patients. The present study was initiated to further validate the safety of spinal anesthesia in pre-eclamptic patients.
METHODOLOGY
After approval from institutional ethics committee this prospective cohort study was conducted at a tertiary care centre in Western Rajasthan from June 2012 to March 2013. Parturients with singleton pregnancy with age18–30 years scheduled for elective cesarean section were included in our study. Written informed consent was taken from every participant. They were divided into two groups as normotensive and the severe pre-eclamptic. Severe pre-eclampsia is defined as any one of the following occurring after the 20 weeks of pregnancy: (i) severe hypertension (systolic blood pressure > 160 mmHg or diastolic blood pressure > 110 mmHg); (ii) proteinuria > 5 gm per 24 h; (iii) oliguria < 400 ml per 24 h; (iv) cerebral irritability or visual disturbances; (v) epigastric or right upper quadrant pain (liver capsule distension) or (vi) pulmonary edema.9
Antihypertensive drugs were not standardized by anesthesiologist and were left on choice of treating obstetrician. Patients in the pre-eclamptic group having signs of neuromuscular irritability and imminent eclampsia had received IV MgSO4 (4 to 6 gm initial loading dose over 20–30 min followed by a 1–2 gm/h continuous maintenance infusion) as part of seizure prophylaxis. We excluded patients in labour, ASA grade IV; patients with chronic hypertension, renal or cardiac disease, multiple gestation, diabetes or coagulopathy, platelet count < 80,000, HELLP syndrome, eclamptic patients, patients on tocolytics, patients who did not give consent; has any contraindication for spinal anesthesia, BMI >35 kg/m2, abruption placentae or placenta previa.
Ranitidine was given in both the groups a night before surgery and antihypertensive medications were continued in the pre eclamptic group. 50 mg IV ranitidine was again administered 30 min prior to surgery in both the groups. After establishing IV access with 18 G cannula preloading was done with 10 ml/kg body weight of ringer lactate solution. Fluid management up to the completion of surgery was standardised for both groups in the study. Standard monitoring was started which includes heart rate (HR), non-invasive blood pressure (NIBP), ECG and oxygen saturation (SpO2). Baseline hemodynamic variables were recorded. Baseline NIBP was measured as the mean of the three readings taken 2 min apart. Spinal anesthesia was given with 25G spinal needle at L3-L4 inter space under all aseptic precautions. All parturients were administered 12.5 mg hyperbaric 0.5% bupivacaine in sitting position. Parturients were then placed supine immediately after subarachnoid block. A wedge was placed under the right hip to prevent aortocaval compression. Surgery was started as soon as the upper level of sensory block reached T4. Infusion of ringer lactate was continued at a rate of 5 ml/kg/h. After spinal anesthesia SBP, DBP, MAP and HR were recorded every 2 min for 20 min and then every 5 min till the completion of surgery. Hypotension (defined as MAP < 20% of the baseline or in normal parturient if SBP< 100 mm Hg) was treated with 5 mg of ephedrine IV boluses, repeated at 5-min intervals if required. Bradycardia (HR < 60 beats/min) was treated with 0.6 mg atropine (maximum 1.8 mg). The total amount of ephedrine consumed was noted. After delivery, oxytocin 10 IU was started as infusion and fetus wellbeing was assessed by Apgar score at 1 and 5 min.
Statistical Analysis: We took convenient sample size of 60 subjects with 30 in each group as it was a pilot study. Descriptive statistics was used to describe frequency. Chi square test or fisher exact test, whichever applicable, was used for categorical data. Unpaired student t test and Mann–Whitney test was used for quantitative variables depending on distribution of the data. P < 0.05 was considered significant. Data were analysed in SPSS version 17.
RESULTS
Baseline demographic variables except weight, ASA grade and blood pressure were comparable in both the groups (Table 1). Mean baseline values of SBP, DBP and MBP were higher in the pre eclamptic group. The preclamptic group included more nulliparous women than in normotensive group
All patients had effective anesthesia and there was no failure. Average uterine incision and delivery time was 2.5 ± 1.4 min in healthy parturient and was 2.5 ± 1.5 min in pre-eclamptic patients. Gestational age for neonates of normotensive group was 38.0 ± 2 weeks and for precelamptic group it was 33 ± 2 weeks. This difference in gestational age was statistically significant (p<0.001).
Table 1: Demographic variables (baseline values)
|
Parameter |
Control (n=30) |
PE group (n=30) |
| Age (years) |
25 ± 3 |
24 ± 4 |
| Weight (Kg) |
61.66 ± 6.4 |
68.36 ± 7.5 |
| Height (cm) |
157.76 ± 2.4 |
158.36 ± 2.6 |
| ASA grade 1 |
17 |
0 |
| 2 |
13 |
18 |
| 3 |
0 |
12 |
| Apgar score 1 min |
7.9 ± 1.1 |
7.6 ± 1.0 |
| 5 min |
9.7 ± 0.4 |
9.4 ± 0.7 |
| Systolic blood pressure (mm Hg) |
127 ± 9 |
154 ± 14 |
| Mean diastolic blood pressure (mm Hg) |
85 ± 7 |
112 ± 19 |
| Mean blood pressure (mm Hg) |
98 ± 9 |
123 ± 14 |
| Heart rate |
93 ± 12 |
97 ± 15 |
Systolic BP, DBP and MBP decreased in both the groups after SAB. The blood pressure records were significantly lower in normotensive group as compared to pre-eclamptic group, 27(90% vs 18(60%) respectively (p < 0.05). The number of episodes of hypotension was more in normotensive group as compared to pre-eclamptic group and the result was statistically significant (p < 0.05) (Table 2). The mean ephedrine requirement (13.4 ± 7.66 mg) was significantly greater in the normotensive group as compared to pre-eclamptic group (6.6 ± 6.75mg) (p < 0.001). Fifteen (50%) patients in control and six (20%) in pre-eclampsia group had adverse effects such as nausea, vomiting or dizziness at the time of hypotension which disappeared after effective treatment with ephedrine.
Table 2: Hypotensive episodes in both groups
|
Number of hypotensive episodes |
Control group (n=30) |
PE group (n=30) |
P value |
| 0 |
3 |
12 |
<0.001 |
| 1 |
5 |
9 |
|
| 2 |
10 |
6 |
|
| 3 |
8 |
2 |
|
| 4 |
3 |
1 |
|
| 5 |
1 |
0 |
Baseline values of heart rate and SpO2 and subsequent changes in both parameters remained comparable in both groups and the differences were statistically insignificant.
The mean intra-operative crystalloid requirement in PE group was 1330 ± 744.36 ml, while in control group it was 1458.33 ± 329.86 ml (P-value > 0.05, statistically not significant).
Apgar scores at 1 and 5 min were comparable in both the groups (Table 1). In post-operative period, HR, SBP, DBP and MAP were recorded four hourly for the next 24 hours. The trend was towards higher values in pre-eclamptic group (p<0.005). There was no difference in HR values in both groups.
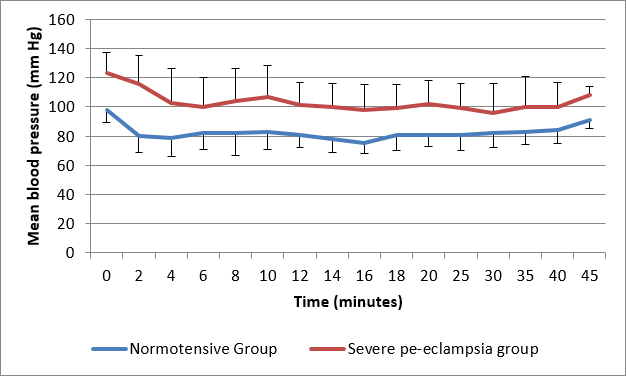
Figure 1: Comparison of mean blood pressure
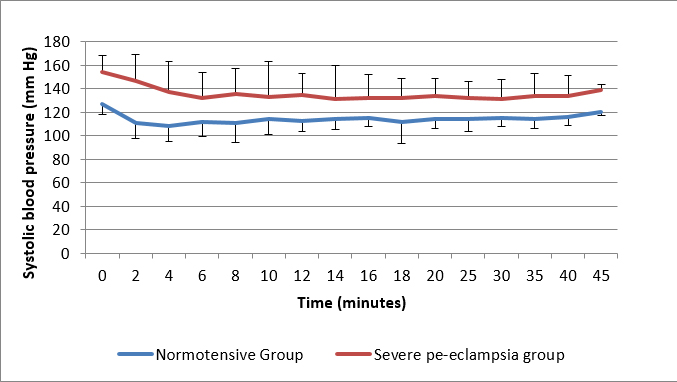
Figure 2: Comparison of systolic blood pressure
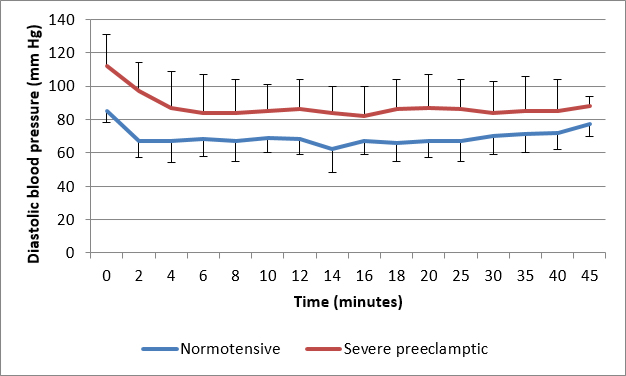
Figure 3: Comparison of diastolic blood pressure
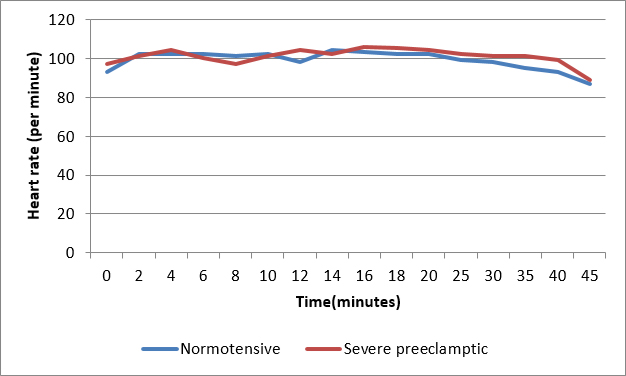
Figure 4: Comparison of heart rate
DISCUSSION
Severe pre-eclampsia is major cause of maternal and perinatal mortality and morbidity. In this study we compared the perioperative hemodynamics after spinal anesthesia along with ephedrine needed in normotensive and severe pre-eclamptic parturients undergoing cesarean section. After spinal anesthesia, NIBP decreased in both the groups from baseline but the minimum readings for SBP, DBP and MAP during the observation period were higher in the pre-eclamptic patients as compared to normotensives.
Epidural anesthesia does not produce sudden hypotension and was traditionally considered safe in patients with pre-eclampsia. However, various studies have shown that the reduction in BP is comparable with either of the two techniques.10-12 Spinal anesthesia is simple to perform, is less time consuming with faster onset and high success rate. In our study the severity of hypotension and the number of hypotensive episodes were less in pre-eclamptic group. Various researchers concluded that the risk and severity of hypotension was almost six times less in patients with severe pre-eclampsia than in healthy parturient.13-15 In our study the mean ephedrine requirement of the normotensive group (27.9 ± 11.6 mg) was significantly greater (P < 0.01) than that of the pre eclamptic group (16.4 ± 15.0 mg). Pre-eclamptic patients may also require less phenylephrine.16
Symptoms of nausea and vomiting are considered as a sensitive indicator of rapid onset hypotension than NIBP measurements.17 In our study five pre-eclamptic patients experienced vomiting in contrast to fifteen in the normotensive group. Regional anesthesia causes hypotension and bradycardia due to decreased vascular resistance and increased parasympathetic tone. Hypovolemia causes stimulation of sensory receptors in left ventricle, induces the Bezold Jarisch reflex (BJR) and results in reflex bradycardia, vasodilation and hypotension.18 Chemoreceptors are activated in response to decreased blood volume by serotonin (5HT3), which is released from activated thrombocytes. Activation of 5-HT3 receptors, which are G protein coupled, ligand-gated, fast-ion channels, and results in increased efferent vagal nerve activity producing nausea and vomiting.19,20
In normal pregnancy there is increased synthesis of prostaglandins (PGs) and nitric oxide, which act as vasodilators and there is increased dependence on sympathetic vasoconstriction for vascular tone. So sympathetic blockade is associated with sudden and excessive hypotension after spinal anesthesia. 21 In pre-eclampsia, there is increased amount of endogenous vasopressors like thromboxane and endothelin, so even after spinal anesthesia vascular tone is maintained preventing excessive fall in BP.22,23 The mean values of HR do not change significantly in both groups.6,7
We found neonatal outcome comparable and good in both the groups in respect to Apgar score at 1 and 5 min after birth which is similar to an earlier study.16 Despite of hemodynamic variability and variable requirement of ephedrine to treat it, we found comparable Apgar scores in both of the groups.
LIMITATIONS
This study was well-designed and well conducted, but with a limitation of sample size as it was a pilot study. Secondly, antihypertensive agent was not standardized because patients were enrolled one day before delivery, by that time patient was already on antihypertensive agent.
CONCLUSION
Our study adds to recent evidence suggesting that hypertensive, but well-controlled and stabilised parturients with severe pre-eclampsia have better perioperative hemodynamic stability, with reduced need of vasopressor under spinal anesthesia. However, multicentre studies with large sample size are required to determine the safety of spinal anesthesia in this setting.
Conflict of interest: The authors declare no conflict of interest related to the publication of this manuscript.
REFERENCES- Endler GC, Mariona FG, Sokol RJ, Stevenson LB. Anesthesia related maternal mortality in Michigan, 1972–1984. Am J Obstet Gynecol 1988;159:187–93. [PubMed]
- Hawkins JL, Koonin LM, Palmer SK, Gibbs CP. Anesthesia related deaths during obstetric delivery in the United States, 1979–1990. Anesthesiology 1997;86:277–84. [PubMed][Free Full Text]
- Sinatra RS, Philip BK, Naulty JS, Ostheimer GW. Prolonged neuromuscular blockade with vecuronium in a patient treated with magnesium sulfate. Anesth Analg. 1985;64:1220–2. [PubMed]
- Sharwood-Smith G H, Clark V A, Watson E. Regional anaesthesia for cesarean section in severe preeclampsia: spinal anaesthesia is the preferred choice. Int J Obstet Anesth 1999;8: 85–89. [PubMed]
- Dyer RA, Piercy JL, Reed AR, Lombard CJ, Schoeman LK, James MF. Hemodynamic changes associated with spinal anaesthesia for caesarean delivery in severe pre-eclampsia. Anesthesiology 2008;108:802-11. [PubMed][Free Full Text]
- Aya AG, Vialles N, Tanoubi I, Mangin R, Ferrer JM, Robert C, et al. Spinal anaesthesia-induced hypotension: A risk comparison between patients with severe pre-eclampsia and healthy women undergoing preterm caesarean delivery. Anesth Analg 2005;101:869-75. [PubMed]
- Santos AC, Birnbach DJ. Spinal anesthesia in the parturient with severe preeclampsia: time for reconsideration. Anesth Analg 2003;97:621-2. [PubMed]
- Turkoz A, Togal T, Gokdeniz R, I Topraks H, Esroy O. Effectiveness of intravenous ephedrine infusion during spinal anaesthesia for caesarean section based on maternal hypotension, neonatal acid-base status and lactate levels. Anaesth Intensive Care 2002;30:316-20. [PubMed]
- Hart E, Coley S. The diagnosis and management of pre-eclampsia. Contin Educ Anaesth. Crit Care Pain 2003;3: 38–42. [Free Full Text]
- Visalyaputra S, Rodanant O, Somboonviboon W, Tantivitayatan K, Thienthog S, Saengchote W. Spinal versus epidural anesthesia for caesarean delivery in severe preeclampsia: A prospective randomized, multicenterstudy. Anesth Analg 2005;101:862-8. [PubMed]
- Hood DD, Curry R. Spinal versus epidural anaesthesia for Caesarean section in severely preeclampticpatients. A retrospective survey.Anesthesiology 1999;90:1276-82. [PubMed][Free Full Text]
- Chiu IU, Mansor M, Ng KP, Chan YK. Retrospective review of spinal versus epidural anaesthesia for caesarean section in preeclamptic patients. Int J Obstet Anesth 2003;12:17-23. [PubMed]
- Aya AG, Mangin R, Vialles N, Ferrer JM, Robert C, Ripart J, et al. Patients with severe pre-eclampsia experience less hypotension during spinal anaesthesia for caesarean delivery than healthy parturients: A prospective cohort comparison. Anesth Analg. 2003;97:867–72. [PubMed]
- Dyer RA, Piercy JL, Reed AR. The role of the anaesthetist in the management of the pre-eclamptic patient. Curr Opin Anaesthesiol. 2007;20:168–74. [PubMed]
- Clark VA, Smith SG, Stewart AV. Ephedrine requirements are reduced during spinal anaesthesia for caesarean section in pre-eclampsia. Int J Obstet Anaesth. 2005;14:9–13.[PubMed]
- Saha D, Ghosh S, Bhattacharyya S, Mallik S, Pal R, Niyogi M, et al. Comparison of hemodynamic response and vasopressor requirement following spinal anaesthesia between normotensive and severe preeclamptic women undergoing caesarean section: A prospective study. J Obstet AnaesthCrit Care 2013;3:23-6. [Free Full Text]
- S Palmese, M Manzi, V Visciano, A Scibilia, A Natale. Reduced Hypotension After Subarachnoid Anaesthesia With Ondansetron Most Colloids In Parturients Undergoing Caesarean Section. A Retrospective Study.. The Internet Journal of Anesthesiology. 2012;30 Number 4. [Access Online]
- Campagna JA, Carter C. Clinical relevance of the Bezold Jarisch reflex. Anesthesiology. 2003;98:1250–60. [PubMed][Free Full Text]
- Aviado DM, Guevara Aviado D. The Bezold-Jarisch reflex: a historical perspective of cardiopulmonary reflexes. Ann N Y Acad Sci. 2001;940: 48-58. [PubMed]
- Somboonviboon W, Kyokong O, Charuluxananan S, et al. Incidence and risk factors of hypotension and bradycardia after spinal anesthesia for caesarean section. J Med Assoc Thai 2008;91: 181–87. [PubMed]
- Hashmi M. Low-pressure headache presenting in early pregnancy with dramatic response to glucocorticoids: a case report. J Med Case Rep. 2014 Apr 3;8(1):115. doi: 10.1186/1752-1947-8-115.
- Redman CW, Sargent IL. Pre-eclampsia, the placenta and the maternal systemic infl ammatory response: A review. Placenta 2003;24:S21-7. [PubMed]
- Santos AC, Birnbach DJ. Spinal anesthesia in the parturient with severe preeclampsia: time for reconsideration. Anesth Analg 2003;97:621-2. [PubMed]