Farhah Muhammad 1 , Fatanah Mohamad Suhaimi 2 , Mohd Zulfakar Mazlan 3
Author affiliations:
Background: Ketum (Mitragyna speciosa) is easily found in Southeast Asia. It consists of primary alkaloids known as mitragynine, which result in effects similar opiods, and are also used for energy stimulant and pain relief in the form of Ketum cocktail drinks. The use of excessive Mitragyna speciosa leads to mitragynine toxicity.
Case presentation: A 22-year-old man presented with agitation, incoherent speech, and multiple generalized tonic-clonic seizures, leading to unconsciousness. Upon ICU admission, he had normal vital signs but required intubation due to a GCS of 3/15. Laboratory results showed elevated creatinine kinase, creatinine, and urea levels, with positive urine mitragynine. The patient was diagnosed with status epilepticus secondary to mitragynine toxicity, meningoencephalitis, and acute kidney injury due to rhabdomyolysis. Treatment included mechanical ventilation, sedation, fluid management, and antibiotics. Despite initial improvement and extubation, the patient was readmitted to ICU with aspiration pneumonia, underwent CPR, and ultimately succumbed to the illness after six days of readmission.
Conclusion: Mitragynine toxicity can cause seizures, rhabdomyolysis, and acute kidney injury. Close monitoring post-ICU discharge is crucial.
Keywords: Acute kidney injury; Ketum; Mitragyna speciose
Citation: Muhammad F, Suhaimi FM, Mazlan MZ. Acute kidney injury associated with mitragynine toxicity: a case report. Anaesth. pain intensive care 2026;30(2):270-273. DOI: 10.35975/apic.v30i2.3137
Received: May 09, 2025; Revised: October 26, 2025; Accepted: January 01, 2026
Ketum, also known as kratom, is a plant from the Rubiaceae family found in areas of Southeast Asia, including Thailand, Malaysia, and the Philippines.1,2 Other names for ketum include thang, thom, kakuam, biakbiak, and maeng da. Traditionally, it has been used to increase the performance of farmers while working and treat various health conditions such as diarrhea, depression, weight loss, etc.1 Ketum leaves consist of many alkaloids, and the primary alkaloid namely mitragynine, interacts with opioid receptors in the brain to produce euphoric effects.1,3
Ketum is available in various forms, such as powder, dried leaves, or tablets.1,2 Moreover, in western countries, it has been used for various purposes, including for chronic pain, mental disorders or alleviating withdrawal symptoms from prescription. It is easily accessible and sold online. It has been marketed as an alternative use of opioids.
Despite its beneficial effects, excessive use of ketum leaves, which have mitragynine, is harmful to people in various health problems, such as tachycardia, agitation, vomiting, depressed in respiration, hallucinations, seizures and coma.4 The research regarding mitragynine toxicity on acute kidney injury (AKI) remains few. Hence, this case study seeks to find the relationship between mitragynine toxicity and acute kidney injury (AKI).
A 22-year-old man was brought home at 2.30 am by his family member, exhibiting agitation and speak incoherently associated with generalized tonic-clonic (GTC) once at home and two times in an ambulance. He was unconsciousness at home. Before his illness, he was in good condition.
Upon ICU admission, the patient presented with normal temperature (36.5°C), blood pressure (135/60 mmHg), and respiratory rate (13/min). GCS was 3/15, requiring intubation. Pupils were 3 mm bilaterally. SpO2 was 100%. Urine output dropped from 50 mL/hr to 5 mL/hr. Laboratory results showed elevated creatinine kinase (2326 U/L), creatinine (198 µmol/L), and urea (7.8 mg/dL). Urine for mitragynine was positive. Renal function and muscle breakdown markers were monitored for 20 days as in Figure 1. Computed Tomography (CT) scan of the brain revealed normal findings.
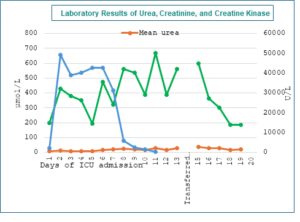
Figure 1: Laboratory results of urea, creatinine, and creatine kinase
This patient was diagnosed with status epilepticus secondary to mitragynine toxicity, meningoencephalitis, and AKI due rhabdomyolysis. This patient was initiated on Volume-Controlled (V/C) ventilation mode 6-8mL/kg tidal volume with the target plateau pressure less than 30 and driving pressure less than 15 cmH2O. He was initially sedated with 120 mg/h propofol and 80 mg/h fentanyl infusion targeted towards Richmond Agitation-Sedation Scale (RASS) score -3 for first 24 hours for cerebral protection while waiting for formal report CT brain. Additionally, 4 mg/mL Precedex was infused at 7 mL/hr.
Intravenous Sterofundin was administered at an initial rate of 80 mL/hr and gradually increased to achieve a target urine output of 1 mL/kg/hr. This balanced electrolyte solution was utilized to address hyperchloremic metabolic acidosis resulting from the excessive use of 0.9% sodium chloride solution. The Sterofundin infusion aimed to promote alkaline diuresis and correct the acid-base imbalance. Within 24-hour admission to ICU, the patient was prescribed with intravenous frusemide at 5 mg/hr to remove excess fluid and lower blood pressure through diuresis. An isotonic bicarbonate solution (NaHCO₃) was supplied at a rate of 80 mL/hour to elevate pH value by neutralizing excess hydrogen ions in the blood aim urine ph more than 6.5. The cumulative amount of input fluid and output fluid are illustrated in Figure 2. Apart from that, intravenous Ceftriaxone 2-gram 8 hourly was administered to treat empirically for meningoencephalitis. Additionally, 8 mg/50 mL of noradrenaline at 1 mL/hour was used to improve perfusion to vital organs, with the target mean arterial pressure (MAP) set at 65 mmHg.
On days 13 and 14, the patient's condition improved significantly. Urine output increased to 120 mL/hr, resolving the oliguria. The patient's Glasgow Coma Scale (GCS) score improved to 15/15, and creatinine levels decreased to 561 U/L. Consequently, the patient was extubated and transferred to the general ward. However, the patient's condition deteriorated rapidly, leading to ICU readmission due to aspiration pneumonia. Cardiopulmonary resuscitation (CPR) was performed for 4 minutes. Despite intensive care, the patient's GCS remained at 3/15 for 6 days, indicating severe neurological impairment. Ultimately, the patient succumbed to the complications and was pronounced dead.
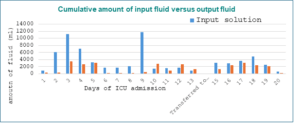
Figure 2: Cumulative amount of input fluid versus output fluid
3. DISCUSSION
This case study highlights the complications of excessive Mitragyna speciosa consumption, resulting in acute kidney injury due to rhabdomyolysis. The use of ketum cocktail drinks in the East Coast of Malaysia, is popular among farmers and drug addicts. To our knowledge, this is the first case study related to mitragynine toxicity-associated AKI. Ketum, often used for its opiod-like effects has been linked to the kidneys, prompting worries over its potential for AKI through breakdown of muscle, and toxicity in the kidneys. The toxicity of mitragynine from consuming excessive ketum was detected by toxicological analysis from urine samples.
In the early symptoms, the patient had GTC seizures due to consequences of mitragynine toxicity and led to rhabdomyolysis where protein known as myoglobin was released to blood, caused increment in serum creatinine, elevated CK and decrease in urine output. Additionally, metabolic acidosis and dehydration from mitragynine toxicity may have worsened the kidney injury.
It is important to start aggressive management to stabilize patient in early ICU admission. Intravenous fluid resuscitation with 0.9% sodium chloride alternate with Sterofundin, isotonic bicarbonate solution, was employed to sustain kidney perfusion and clearance of myoglobin. Intravenous frusemide was initiated to promote diuresis and avoid overload of urine volume. Serum creatinine and urine output were improved. Hence, this patient was discharged from ICU to the general ward, however, due to aspiration pneumonia, a common consequence in patients recovering from seizures, overdose of drug,5 and also ketum withdrawal, caused this patient condition to worsen later, resulted in death.
4. CONCLUSION
Mitragynine intoxication can manifest with seizures, rhabdomyolysis, and acute renal failure. Vigilant follow-up is essential after ICU discharge for patients with mitragynine-induced kidney damage. The rising prevalence of Mitragyna speciosa use and its potentially underrecognized renal effects underscore the need for further clinical study.
MS: Manuscript editing
MZM: Concept, Conduction of study work, Manuscript editing
Author affiliations:
- Farhah Muhammad, Advanced Medical and Dental Institute, Universiti Sains Malaysia, Bertam, 13200 Kepala Batas, Penang, Malaysia; Email: farhah_muhammad@student.usm.my
- Fatanah Mohamad Suhaimi, Advanced Medical and Dental Institute, Universiti Sains Malaysia, Bertam, 13200 Kepala Batas, Penang, Malaysia; Email: fatanah.suhaimi@usm.my
- Mohd Zulfakar Mazlan, Department of Anaesthesiology and Intensive Care, School of Medical Sciences, Universiti Sains Malaysia, 16150 Kota Bharu, Kelantan, Malaysia; Email: zulfakar@usm.my
ABSTRACT
Background: Ketum (Mitragyna speciosa) is easily found in Southeast Asia. It consists of primary alkaloids known as mitragynine, which result in effects similar opiods, and are also used for energy stimulant and pain relief in the form of Ketum cocktail drinks. The use of excessive Mitragyna speciosa leads to mitragynine toxicity.
Case presentation: A 22-year-old man presented with agitation, incoherent speech, and multiple generalized tonic-clonic seizures, leading to unconsciousness. Upon ICU admission, he had normal vital signs but required intubation due to a GCS of 3/15. Laboratory results showed elevated creatinine kinase, creatinine, and urea levels, with positive urine mitragynine. The patient was diagnosed with status epilepticus secondary to mitragynine toxicity, meningoencephalitis, and acute kidney injury due to rhabdomyolysis. Treatment included mechanical ventilation, sedation, fluid management, and antibiotics. Despite initial improvement and extubation, the patient was readmitted to ICU with aspiration pneumonia, underwent CPR, and ultimately succumbed to the illness after six days of readmission.
Conclusion: Mitragynine toxicity can cause seizures, rhabdomyolysis, and acute kidney injury. Close monitoring post-ICU discharge is crucial.
Keywords: Acute kidney injury; Ketum; Mitragyna speciose
Citation: Muhammad F, Suhaimi FM, Mazlan MZ. Acute kidney injury associated with mitragynine toxicity: a case report. Anaesth. pain intensive care 2026;30(2):270-273. DOI: 10.35975/apic.v30i2.3137
Received: May 09, 2025; Revised: October 26, 2025; Accepted: January 01, 2026
1. INTRODUCTION
Ketum, also known as kratom, is a plant from the Rubiaceae family found in areas of Southeast Asia, including Thailand, Malaysia, and the Philippines.1,2 Other names for ketum include thang, thom, kakuam, biakbiak, and maeng da. Traditionally, it has been used to increase the performance of farmers while working and treat various health conditions such as diarrhea, depression, weight loss, etc.1 Ketum leaves consist of many alkaloids, and the primary alkaloid namely mitragynine, interacts with opioid receptors in the brain to produce euphoric effects.1,3
Ketum is available in various forms, such as powder, dried leaves, or tablets.1,2 Moreover, in western countries, it has been used for various purposes, including for chronic pain, mental disorders or alleviating withdrawal symptoms from prescription. It is easily accessible and sold online. It has been marketed as an alternative use of opioids.
Despite its beneficial effects, excessive use of ketum leaves, which have mitragynine, is harmful to people in various health problems, such as tachycardia, agitation, vomiting, depressed in respiration, hallucinations, seizures and coma.4 The research regarding mitragynine toxicity on acute kidney injury (AKI) remains few. Hence, this case study seeks to find the relationship between mitragynine toxicity and acute kidney injury (AKI).
2. CASE REPORT
A 22-year-old man was brought home at 2.30 am by his family member, exhibiting agitation and speak incoherently associated with generalized tonic-clonic (GTC) once at home and two times in an ambulance. He was unconsciousness at home. Before his illness, he was in good condition.
Upon ICU admission, the patient presented with normal temperature (36.5°C), blood pressure (135/60 mmHg), and respiratory rate (13/min). GCS was 3/15, requiring intubation. Pupils were 3 mm bilaterally. SpO2 was 100%. Urine output dropped from 50 mL/hr to 5 mL/hr. Laboratory results showed elevated creatinine kinase (2326 U/L), creatinine (198 µmol/L), and urea (7.8 mg/dL). Urine for mitragynine was positive. Renal function and muscle breakdown markers were monitored for 20 days as in Figure 1. Computed Tomography (CT) scan of the brain revealed normal findings.
Figure 1: Laboratory results of urea, creatinine, and creatine kinase
This patient was diagnosed with status epilepticus secondary to mitragynine toxicity, meningoencephalitis, and AKI due rhabdomyolysis. This patient was initiated on Volume-Controlled (V/C) ventilation mode 6-8mL/kg tidal volume with the target plateau pressure less than 30 and driving pressure less than 15 cmH2O. He was initially sedated with 120 mg/h propofol and 80 mg/h fentanyl infusion targeted towards Richmond Agitation-Sedation Scale (RASS) score -3 for first 24 hours for cerebral protection while waiting for formal report CT brain. Additionally, 4 mg/mL Precedex was infused at 7 mL/hr.
Intravenous Sterofundin was administered at an initial rate of 80 mL/hr and gradually increased to achieve a target urine output of 1 mL/kg/hr. This balanced electrolyte solution was utilized to address hyperchloremic metabolic acidosis resulting from the excessive use of 0.9% sodium chloride solution. The Sterofundin infusion aimed to promote alkaline diuresis and correct the acid-base imbalance. Within 24-hour admission to ICU, the patient was prescribed with intravenous frusemide at 5 mg/hr to remove excess fluid and lower blood pressure through diuresis. An isotonic bicarbonate solution (NaHCO₃) was supplied at a rate of 80 mL/hour to elevate pH value by neutralizing excess hydrogen ions in the blood aim urine ph more than 6.5. The cumulative amount of input fluid and output fluid are illustrated in Figure 2. Apart from that, intravenous Ceftriaxone 2-gram 8 hourly was administered to treat empirically for meningoencephalitis. Additionally, 8 mg/50 mL of noradrenaline at 1 mL/hour was used to improve perfusion to vital organs, with the target mean arterial pressure (MAP) set at 65 mmHg.
On days 13 and 14, the patient's condition improved significantly. Urine output increased to 120 mL/hr, resolving the oliguria. The patient's Glasgow Coma Scale (GCS) score improved to 15/15, and creatinine levels decreased to 561 U/L. Consequently, the patient was extubated and transferred to the general ward. However, the patient's condition deteriorated rapidly, leading to ICU readmission due to aspiration pneumonia. Cardiopulmonary resuscitation (CPR) was performed for 4 minutes. Despite intensive care, the patient's GCS remained at 3/15 for 6 days, indicating severe neurological impairment. Ultimately, the patient succumbed to the complications and was pronounced dead.
Figure 2: Cumulative amount of input fluid versus output fluid
3. DISCUSSION
This case study highlights the complications of excessive Mitragyna speciosa consumption, resulting in acute kidney injury due to rhabdomyolysis. The use of ketum cocktail drinks in the East Coast of Malaysia, is popular among farmers and drug addicts. To our knowledge, this is the first case study related to mitragynine toxicity-associated AKI. Ketum, often used for its opiod-like effects has been linked to the kidneys, prompting worries over its potential for AKI through breakdown of muscle, and toxicity in the kidneys. The toxicity of mitragynine from consuming excessive ketum was detected by toxicological analysis from urine samples.
In the early symptoms, the patient had GTC seizures due to consequences of mitragynine toxicity and led to rhabdomyolysis where protein known as myoglobin was released to blood, caused increment in serum creatinine, elevated CK and decrease in urine output. Additionally, metabolic acidosis and dehydration from mitragynine toxicity may have worsened the kidney injury.
It is important to start aggressive management to stabilize patient in early ICU admission. Intravenous fluid resuscitation with 0.9% sodium chloride alternate with Sterofundin, isotonic bicarbonate solution, was employed to sustain kidney perfusion and clearance of myoglobin. Intravenous frusemide was initiated to promote diuresis and avoid overload of urine volume. Serum creatinine and urine output were improved. Hence, this patient was discharged from ICU to the general ward, however, due to aspiration pneumonia, a common consequence in patients recovering from seizures, overdose of drug,5 and also ketum withdrawal, caused this patient condition to worsen later, resulted in death.
4. CONCLUSION
Mitragynine intoxication can manifest with seizures, rhabdomyolysis, and acute renal failure. Vigilant follow-up is essential after ICU discharge for patients with mitragynine-induced kidney damage. The rising prevalence of Mitragyna speciosa use and its potentially underrecognized renal effects underscore the need for further clinical study.
- Conflict of interest
- Ethical considerations.
- Authors’ contribution
MS: Manuscript editing
MZM: Concept, Conduction of study work, Manuscript editing
8. REFERENCES
- Ulbricht C, Costa D, Dao J, Isaac R, LeBlanc YC, Rhoades J, Windsor RC. An evidence-based systematic review of kratom (Mitragyna speciosa) by the Natural Standard Research Collaboration. J Diet Suppl. 2013 Jun;10(2):152-70.,[PubMed] DOI: 3109/19390211.2013.793541 .
- Singh D, Narayanan S, Vicknasingam B. Traditional and non-traditional uses of Mitragynine (Kratom): A survey of the literature. Brain Res Bull. 2016 Sep;126(Pt 1):41-46. [PubMed] DOI: 1016/j.brainresbull.2016.05.004
- Ahmad K, Aziz Z. Mitragyna speciosa use in the northern states of Malaysia: a cross-sectional study. J Ethnopharmacol. 2012 May 7;141(1):446-50., [PubMed] DOI: 1016/j.jep.2012.03.009
- .Eggleston W, Stoppacher R, Suen K, Marraffa JM, Nelson LS. Kratom Use and Toxicities in the United States. Pharmacotherapy. 2019 Jul;39(7):775-777. [PubMed] DOI: 1002/phar.2280
- R. Sanivarapu, S. Vaqar, and J. Gibson, Aspiration Pneumonia. StatsPearls, 2024. [Online]. Available: https://www.ncbi.nlm.nih.gov/books/NBK470459/