Baseeha Sereen V.a 1 , Swadika Natarajan 2 , Balasubramanian Arunkumar 3 , Shanu Shanmugasundaram 4 , Arbind Kumar Choudhary 5 , Panneerselvam Periasamy 6
Authors affiliations:
Background & objective: Maintaining hemodynamic stability and minimizing blood loss are critical goals in perioperative care. Clonidine, an α2-adrenergic agonist, and metoprolol, a selective β1-blocker, are frequently used to modulate cardiovascular responses during surgery. However, their comparative efficacy in reducing intraoperative blood loss and supporting postoperative recovery remains a subject of clinical interest. This study compared the efficacy of the both to facilitate the choice.
Methodology: This prospective, randomized controlled trial included 60 ASA I–II patients aged 18–60 years undergoing elective surgery under general anesthesia. Participants were randomized to receive either oral clonidine (0.15 mg, Group-C, n = 30) or metoprolol (50 mg, Group-M, n = 30) two hours before surgery. Intraoperative hemodynamic parameters, estimated blood loss, surgical field quality, and postoperative outcomes including pain score, nausea incidence, recovery time, and hospital stay were recorded and statistically analyzed.
Results: Both groups maintained stable intraoperative heart rate, blood pressure, and oxygen saturation (P > 0.05). Clonidine significantly reduced intraoperative blood loss compared to metoprolol (137 ± 14.71 mL vs. 151 ± 9.94 mL, P = 0.0002) and achieved better surgical field visibility (Good field: 70% vs. 56.7%, P = 0.041). Postoperative outcomes, including pain scores, recovery time, and hospital stay, were comparable across groups (P > 0.05).
Conclusion: Clonidine and metoprolol are both effective for intraoperative hemodynamic control and safe postoperative recovery. However, clonidine demonstrates a distinct advantage in minimizing blood loss and improving surgical field quality. These findings support its preferential use in procedures where blood conservation is crucial. Larger multicentric studies are recommended to guide patient-specific drug selection in perioperative management.
Keywords: Blood loss; Clonidine; Elective surgery; Hemodynamic stability; Hospital stay; Metoprolol; Pain scores; Postoperative recovery
Citation: Sereen V.a B, Natarajan S, Arunkumar B, Shanmugasundaram S, Choudhary AK, Periasamy P. Comparative evaluation of clonidine and metoprolol for perioperative hemodynamic stability, blood loss control, and postoperative recovery in patients undergoing elective surgery: a prospective randomized controlled study. Anaesth. pain intensive care 2026;30(2):189-199. DOI: 10.35975/apic.v30i2.3126
Received: May 13, 2025; Revised: May 17, 2025; Accepted: June 07, 2025
The surgical recovery duration represents a strenuous time in medical treatment where several elements from anesthetic drugs interact within surgical conditions and patient health complications. The development of elevated sympathetic activity increases heart rate together with blood pressure and vascular tone changes which represents essential concerns for this period. These pharmacological alterations lead to higher blood losses during operations and reduced exposure to the operating site and worsened post-surgical recovery times. Modern anesthesia practice depends heavily on medications that modify patients' blood pressure parameters. Clinicians use clonidine and metoprolol as standard perioperative medications but research continues regarding their specific effects on multiple aspects of surgical care. Surgeries activate two stress systems: the sympathetic nervous system and the hypothalamic-pituitary-adrenal (HPA) axis which causes elevated catecholamine release together with elevated systemic vascular resistance. Organizations which require crystal-clear operative fields and bloodless working environments face risks from these systemic vascular changes. Anesthesiologists look for pharmaceutical compounds which combine safety measures for patients with reliable blood pressure control and seamless postoperative recovery.
The central mechanism of clonidine action comes from stimulation of medullary α2-adrenergic receptors that decreases both sympathetic nerve signalling and norepinephrine concentration in plasma. The medication leads to heart rate reduction and decreased mean arterial pressure and decreased vascular tone. The oral administration of clonidine before surgery proved effective for improving intraoperative blood pressure stability while reducing surgical bleeding in functional endoscopic sinus surgery patients according to Puthenveettil et al. (2015).1 The research by Choudhary et al. (2024) demonstrated that clonidine administration produced better operative field views and maintained better blood pressure steady states in otolaryngology procedures.2
The sedative and analgesia-sparing qualities of clonidine help decrease opioid consumption thereby enhancing surgical anesthetic emergence while improving patient satisfaction. The clinical advantages of these effects work specifically well for patients undergoing day-care and ambulatory surgeries because they need early postoperative recovery before being discharged. The administration of clonidine before laparoscopic cholecystectomy led to decreased anesthetic requirements and better heart condition results than placebo according to Ahmed et al. (2016).3
The cardiac protective measures offered by metoprolol derive from its mechanism which blocks β1-adrenergic receptors specifically in heart muscle tissue. The pharmacodynamic properties of negative chronotropic and inotropic action decrease myocardial oxygen need which makes metoprolol a preferred medicine for patients with ischemic or arrhythmic risks in the perioperative period. More than 8,000 patients in the Devereaux et al. (2008) POISE trial underwent non-cardiac surgery and indicated that perioperative metoprolol decreased myocardial infarction occurrence. Stroke happened more frequently and patients faced increased mortality risk because hypotension and bradycardia occurred during treatment.4 The clinical application of beta-blockers in surgery now depends on patient risk level and medical history as well as specific medication requirements. The results from MaVS demonstrate that metoprolol administration effectively managed heart rate but incidents of hypotension as well as delayed recovery appeared more often in patients treated with metoprolol compared to controls.5 The interest has grown to study clonidine as an alternative agent because these studies discovered cardiovascular stability effects comparable to metoprolol with reduced complications.
Different studies measured the operation-based performance results between clonidine therapy and metoprolol treatment within controlled surgical settings. In a surgical experiment Gohil et al. (2013) documented that clonidine-treated patients presented both lower bleeding scores and superior field grading than patients who received metoprolol or diazepam treatment especially during minimally bleeding surgeries.6 The research by Meena et al. (2024) showed clonidine achieved two benefits during laparoscopic procedures because it enhanced visibility and decreased the need for volatile anesthetic drugs.7
The peripheral vasoconstriction property of clonidine which results from central sympatholysis successfully decreases surgical bleeding and suction volume during surgical interventions. Recent outcomes from Wawrzyniak et al. (2013) demonstrated that premedicating patients with clonidine produced superior operative visibility compared to control patients when using total intravenous anesthesia.8 Clonidine stands out as an ideal medication for performing successful surgeries in otolaryngology and neurosurgery departments because of its specific properties.
Postoperative benefits from clonidine treatment continue because the drug minimizes sympathetic overreactions and defends against hypertension while decreasing patients' need for pain medicines. The preoperative administration of clonidine to patients yielded enhanced examination outcomes without detrimental opioid usage after surgery according to Sung et al. (2000) as recorded in.9 High heart rate control from metoprolol treatment exists but this drug does not provide sedation thus patients usually need extra medications to manage surgery-related pain and anxiety.
Numerous research findings continue to exist in separate sections since researchers use diverse study plans which leads to varied sample counts and assessment approaches. Research on the comparison of these drugs mainly concentrates on particular types of operations while using non-unified measures for blood loss evaluation and surgical field condition assessments. Existing trials evaluate least both intraoperative and postoperative outcomes separately which makes it difficult to determine the best agent.
The research used a randomized controlled experimental design to directly measure the effects between preoperative use of oral clonidine in 0.15 mg doses versus oral metoprolol in 50 mg doses for patients receiving general anesthetic during scheduled surgical procedures. The main research targets evaluate intraoperative blood pressure management and blood loss amounts and surgical site condition after completion of surgical procedures. The study evaluates postoperative results including recovery time as well as visual analog pain scores and frequencies of nausea and time to first anesthetic requirements and duration of hospital stay. This investigation provides a direct comparison between clonidine and metoprolol through standardized measurements in order to deliver practical findings about perioperative utilization. Studies into the variations between clonidine and metoprolol pharmacodynamics will enable better decision-making for individual drug choices and improve the delivery of perioperative care to different patient groups.
The study obtained Institutional Ethics Committee authorization and the required Clinical Trials Registry of India (CTRI/2022/01/039572) registration to run for 15 months. Patients were enrolled following written informed consent. The study enrolled adults who met the requirements of belonging to between 18 years and 60 years of age with an American Society of Anesthesiologists (ASA) physical status classification at level I or II. The study excluded patients who had cardiovascular, renal, hepatic, respiratory conditions along with beta-blocker or clonidine usage within the past month and pregnant or breastfeeding women and those with contraindicated to general anesthesia. The necessary sample size resulted from power calculation which built upon an earlier research comparing clonidine and metoprolol effects on intraoperative blood loss. The determined minimum participant count for each group reached 26 individuals to establish significant statistical differences with these parameters: 80% power and 0.05 alpha error and 0.8 effect size. A total of 60 patients were recruited for this study to account for potential dropouts with equal numbers in each group (Group-C clonidine n=30 + Group-M metoprolol n=30). Randomization occurred through the use of computer-generated block methods. The allocation sequence remained hidden with sealed opaque envelopes that were opened during surgery times. The staff who gave premedication medications were absent from both intraoperative observation tasks and postoperative evaluation procedures. Double blinding between both data collectors and the treated subject enabled researchers to conduct a study design with blind conditions. Before surgical operations all patients received instructions to skip eating the night before. The participants received their assigned medications two hours prior to their scheduled surgery on the surgical day. The participants in Group-C received 0.15 mg of clonidine as an oral medication along with 30 mL of water while Group-M participants took 50 mg oral metoprolol with 30 mL water. All patients received intravenous administration of glycopyrrolate 0.2 mg combined with ondansetron 8 mg as standard premedication procedure before receiving anesthesia. Standard operating room monitor applications included electrocardiogram together with non-invasive blood pressure measurement and pulse oximetry. Baseline readings were recorded. The patient received a combination of intravenous medications including fentanyl 2 mcg/kg along with propofol 2 mg/kg and vecuronium 0.1 mg/kg so that endotracheal intubation could be accomplished. During maintenance anesthesia the patients received a 66% nitrous oxide mix with 33% oxygen and isoflurane 0.8–1.0%. The infiltration of Ringer lactate started at 10 mL/kg/hour for the first hour before reducing to 5 mL/kg/hour. Heart rate along with systolic pressure and diastolic pressure and respiratory rate and oxygen saturation received focused measurement points for baseline pre-induction then immediately upon induction and regularly from minutes 0 through 20 then at 60 and 120 and 180 minutes.
The measurement of intraoperative blood loss occurred through a specific method which used hemoglobin assessment. Surgery commenced with heparin (1:250,000) added to the suction canister to prevent clotting formation. Researchers recorded all fluid matter in the suction bottle after completing the surgical procedure. The estimation of blood loss involved using the patient's mean hemoglobin value and collected fluid hemoglobin concentration according to the standard calculation.
The operating surgeon rated surgical field quality independently through the surgical rating scale known as Average Category Scale (ACS) developed by From me and Boeza art. According to the Average Category Scale the operative field quality receives Good (ACS 0–1, minimal or no suction needed) grading or Fair (ACS 2–3, intermittent suction required) and Poor (ACS 4–5, continuous suction needed due to bleeding) ratings.
The study measured recovery time as well as VAS pain scores and both nausea frequency and requirement for postoperative analgesia and time-to-first analgesia and lasted until the hospital stay ended. Intravenous paracetamol 1 g functioned as rescue analgesia that doctors administered through an IV to patients when their VAS score reached 4 or more.
The data collected went into a master sheet designed before analysis while EPI Info version 7.2 performed the statistical analysis. Assessment of continuous variables for normal distribution occurred before statistical analysis with either the independent samples t-test or Mann–Whitney U test based on data characteristics. The analysis of categorical variables involved Chi-square or Yates' corrected Chi-square testing methods. The research determined significant statistical results from p-values that remained below 0.05.
The demographic and baseline characteristics of the study participants were comparable between Group-C and Group-M, as shown in Table 1. The mean age, gender distribution, ASA classification, height, weight, and preoperative laboratory parameters, including hemoglobin levels, random blood sugar, serum creatinine, and electrolytes, showed no statistically significant differences (P > 0.05 for all variables).
Preoperative screening assessments, such as ECG and chest X-ray findings, indicated a high percentage of normal results in both groups, with no significant between-group variation. These findings confirm that both study groups were well-matched at baseline, minimizing potential confounding effects on hemodynamic and recovery outcomes.
The similarity in demographic, physical, and biochemical characteristics between the two groups confirms a well-balanced randomization process, ensuring a valid comparison of perioperative hemodynamic and recovery outcomes.
The intraoperative hemodynamic and respiratory parameters were monitored at multiple time points, including preoperative (Preop), immediately after induction (0 min), and at subsequent intervals up to 180 minutes. As shown in Table 2, and Figure 1 both Group-C and Group-M maintained stable heart rates, systolic blood pressure, diastolic blood pressure, respiratory rates, and oxygen saturation levels throughout the surgical period.
No statistically significant differences were observed between the two groups for any hemodynamic or respiratory parameters at any time point (P > 0.05 for all comparisons). These results indicate that both clonidine and metoprolol provide comparable intraoperative cardiovascular stability, reinforcing their effectiveness in maintaining perioperative hemodynamic control.
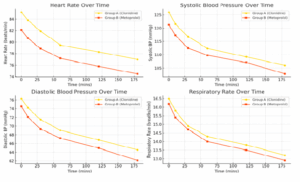
Figure 1: Hemodynamic parameters in both groups
Both groups exhibited a gradual reduction in heart rate and blood pressure over time, with no clinically significant variations between Group-C and Group-M. This indicates that both drugs effectively control intraoperative hemodynamics, ensuring stable cardiovascular function throughout surgery. Respiratory function remained stable in both groups, with no significant respiratory depression observed. Oxygen saturation levels were consistently above 98%, reinforcing the safety profile of both drugs in maintaining adequate oxygenation during the perioperative period. Overall, the findings in Table 2 confirm that clonidine and metoprolol provide stable intraoperative hemodynamic and respiratory parameters, ensuring adequate cardiovascular control without significant adverse fluctuations.
The figure demonstrates that both clonidine and metoprolol effectively maintain intraoperative hemodynamic stability. Heart rate, systolic and diastolic blood pressure, and respiratory rate show a gradual decline over time, with no significant differences between groups. Clonidine exhibited slightly higher heart rate and BP trends, while respiratory rates remained consistent in both groups. These findings confirm that both drugs provide comparable and safe perioperative hemodynamic control.
3.1. Hemoglobin and Blood Loss Indicators
As shown in Table 3, preoperative and postoperative hemoglobin levels, mean hemoglobin concentration, and haematocrit values were comparable between the two groups (P > 0.05), indicating similar overall hemoglobin stability. However, suction volume and total blood loss were significantly lower in Group-C than in Group-M, both before and after adjusting for haematocrit levels (P < 0.05).
Table 4 further supports these findings, demonstrating a higher percentage of "Good" surgical field conditions in the clonidine group (70%) compared to metoprolol (56.67%) (P = 0.041). This suggests that clonidine contributes to better operative visibility and reduced bleeding, reinforcing its potential advantage in managing intraoperative blood loss.
Clonidine resulted in lower blood loss, improved surgical field conditions, and better intraoperative visibility, while hemoglobin levels remained stable in both groups.
3.2. Hemodynamic Stability and Time-to-Event Analysis
The intraoperative hemodynamic stability was assessed through repeated measures ANOVA, correlation analysis, variability measures (CV), and time-to-event analysis for hemodynamic instability. As shown in Table 5, both clonidine (Group-C) and metoprolol (Group-M) maintained stable heart rate, systolic blood pressure, diastolic blood pressure, respiratory rate, and oxygen saturation over time, with no significant intraoperative fluctuations observed (P > 0.05). Correlation analysis revealed a moderate positive correlation between heart rate and blood pressure at different time points, with no statistically significant differences between the two groups (P > 0.05). This supports the predictable cardiovascular response under both treatment conditions. Similarly, the coefficient of variation (CV) for heart rate, systolic blood pressure, and diastolic blood pressure showed low variability, reinforcing the stability and reliability of both drugs in perioperative cardiovascular control (P > 0.05).
Time-to-event analysis demonstrated that the incidence of BP drops, heart rate spikes, respiratory rate changes, and oxygen saturation drops was comparable between the two groups, with no statistically significant differences (P > 0.05). These findings suggest that neither drug increases the risk of hemodynamic instability, supporting their clinical safety and efficacy in perioperative management.
The findings in Table 5 confirm that both clonidine and metoprolol provide consistent perioperative hemodynamic stability, with no significant differences in trends, correlation patterns, or variability measures. The similar time-to-event analysis results further reinforce the clinical reliability of both drugs in maintaining cardiovascular stability without increasing the risk of hemodynamic instability.
3.3. SubGroup-Cnalysis by Demographics
The subGroup-Cnalysis examined heart rate and systolic blood pressure variations across different demographic categories, including age (<40 vs. ≥40 years), gender, and ASA classification (I vs. II). As shown in Table 6, no statistically significant differences were observed between Group-C and Group-M across all subgroups (P > 0.05). Among participants younger than 40 years, the heart rate and systolic blood pressure values were slightly higher in the clonidine group compared to metoprolol, but the differences were not statistically significant (P = 0.15 and P = 0.18, respectively). Similarly, in participants aged 40 years or older, both parameters remained comparable between the two groups (P = 0.22 and P = 0.16, respectively). Gender-based comparisons revealed similar heart rate trends in both male and female participants, with no significant variations (P = 0.33 and P = 0.21, respectively). Additionally, ASA grade I and II patients exhibited similar systolic blood pressure values between the groups, indicating that both clonidine and metoprolol provide stable hemodynamic control across different ASA classifications.
These findings confirm that both drugs maintain consistent hemodynamic stability, irrespective of age, gender, or ASA classification, supporting their generalizability and safety for a diverse perioperative patient population.
The subGroup-Cnalysis in Table 6 reinforces that clonidine and metoprolol exhibit consistent hemodynamic effects across different demographic categories, with no statistically significant differences observed. This supports their widespread applicability and safety in perioperative hemodynamic management.
3.4. Postoperative Outcomes Analysis
The postoperative recovery parameters, including recovery time, pain scores, nausea incidence, and hospital stay duration, were assessed between Group-C and Group-M. As presented in Table 7, there were no significant differences in recovery time (P = 0.48), pain scores (P = 0.38), nausea incidence (P = 0.72), or hospital stay duration (P = 0.55) between the groups.
Additionally, postoperative analgesic requirements and time to first analgesia administration were evaluated, showing no significant variations between the groups (P > 0.05). The comparable analgesic consumption and similar timing of initial analgesia administration further suggest equivalent pain management effectiveness between clonidine and metoprolol. These findings indicate that both drugs provide similar postoperative recovery profiles, without adversely affecting pain control, nausea incidence, or length of hospital stay, and effective in differences in recovery time, pain management, nausea incidence, or hospital stay duration. These results reinforce that both drugs are equally safe and effective in perioperative pain control and recovery. Figure 3 illustrates the trend of oxygen saturation levels over time in both groups. Oxygen saturation perioperative pain control and recovery.
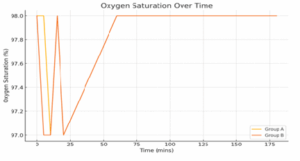
Figure 3: Line graph for oxygen saturation over time
Figure 3 illustrates the trend of oxygen saturation levels over time in both groups. Oxygen saturation remained consistently high throughout the intraoperative period, with no clinically significant desaturation observed in either group. These findings indicate that both clonidine and metoprolol maintain stable respiratory function and are safe with respect to preserving adequate oxygenation during supporting their clinical utility in perioperative care. The findings in Table 7 confirm that clonidine and metoprolol providecomparable postoperative outcomes, with no significant differences in recovery time, pain management, nausea incidence, or hospital stay duration. These results reinforce that both drugs are equally safe surgery.
An evaluation through randomized controlled trial examined the surgical effectiveness of clonidine pills and metoprolol for adult patients who underwent general anesthesia procedures. The administered drugs successfully stabilized the patient's intraoperative blood pressure levels and they recovered equally well postoperatively. The study showed that clonidine proved superior to other medications by reducing surgical field blood loss and producing better surgical conditions.
Results indicated that after blood pressure and heart rate and oxygen saturation stayed consistent both teams received better surgical field assessment but clonidine group experienced less bleeding during operations The research shows that clonidine effectively reduces intraoperative bleeding because it causes central sympatholysis and blocks catecholamine release.11 The study by Devendran et al. established that clonidine generated superior operative visibility and caused more effective bleeding reduction during FESS in comparison to metoprolol.12 The heart rate regulation benefits of metoprolol equated those of other β1-adrenergic blockers yet the drug proved ineffective in improving aurgical field condition variables similarly. The study results matched previous research by Choudhary et al. because clonidine provided superior field quality with lower anesthetic needs despite maintaining stable heart dynamics.13,14 Some research by Dhakne et al. revealed better blood loss reduction results showed clonidine produced better treatment outcomes in all respects including bleeding control and operative visibility and anesthetic efficiency for otolaryngological operations according to studies in Table 3.17-21 Menezes et al. demonstrated that clonidine stabilizes blood pressure after surgery while preventing hypertension rebound whereas metoprolol showed no such effect according to their report.The examined groups displayed equivalent postoperative results when measuring pain scores and recovery duration together with nausea frequency and hospitalization length. The analysis from Sung et al. confirmed that patients received less analgesics after surgery but their emergence time and hospital stay were not affected by clonidine administration.22 The study results showed no significant differences probably because the pain management protocol was uniform and surgeries were short in duration.
The subgroup evaluation demonstrated that the outcomes between the drugs remained equivalent for patients from all age categories and both genders and all ASA levels one through two. Consequently, both drugs proved secure and effective for this wide patient population range. Research by Wawrzyniak et al. confirmed that clonidine improves surgical field quality
The research encountered some limitations in its design. The research included only one medical facility and its participant numbers were limited while also omitting patients who demonstrated high surgical risk factors (ASA III–IV). The surgical field grade assessments used an established scoring method yet depended on subjective measurements. The study failed to evaluate the delayed cardiovascular outcomes together with sedation effects and functional recovery measurements.
The results of this randomized controlled trial proved that both oral clonidine (0.15 mg) and oral metoprolol (50 mg) showed effectiveness for maintaining intraoperative hemodynamic stability as well as guaranteeing secure postoperative recovery in elective surgery patients who were ASA I–II under general anesthesia. The main benefit of clonidine stood out by substantially decreasing blood loss during operations and improving surgery visibility without generating extra negative side effects. The study results endorse clonidine's selection over other options for medical procedures which depend on controlled bleeding. The clinical consequences of our study results have substantial importance. Clonidine provides threefold advantages during surgery because it reduces stress reactions while performing pain management and sedation functions particularly when visibility matters and blood conservation is essential. The affordability along with oral availability of clonidine makes this medication ideal for healthcare institutions serving the public sector or operating with resource restrictions.
SN: Patient Recruitment, Clinical Monitoring, Manuscript Review
BA: Study Design Supervision, Methodological Guidance
SS: Data Analysis, Interpretation, Correspondence, Final Manuscript Approval
AKC: Statistical Analysis, Pharmacological Input, Reference Validation
PP: Physiological Correlation, Data Interpretation, Proofreading
Authors affiliations:
- Baseeha Sereen V.a, Postgraduate, Dept. of Anesthesiology, VMMC & H, VMRF-DU, Salem, India; Email: sereenisma@gmail.com
- Swadika Natarajan, Senior Resident, Dept. of Anesthesiology, PSG IMS & R, Coimbatore, India; Email: swadika3895@gmail.com
- Balasubramanian Arunkumar, Professor of Anaesthesiology, VMMC & H, VMRF-DU, Salem, India.
- Shanu Shanmugasundaram, Assistant Professor, Dept. of Anesthesiology, VMMC & H, VMRF-DU, Salem, India; Email: shanushanmugasundaram@gmail.com
- Arbind Kumar Choudhary, Assistant Professor of Pharmacology, Govt. Erode Medical College, Tamil Nadu, India; Email: arbindkch@gmail.com
- Panneerselvam Periasamy, Assistant Professor of Physiology, Govt. Erode Medical College, Tamil Nadu, India; Email: pannphysio@gmail.com
ABSTRACT
Background & objective: Maintaining hemodynamic stability and minimizing blood loss are critical goals in perioperative care. Clonidine, an α2-adrenergic agonist, and metoprolol, a selective β1-blocker, are frequently used to modulate cardiovascular responses during surgery. However, their comparative efficacy in reducing intraoperative blood loss and supporting postoperative recovery remains a subject of clinical interest. This study compared the efficacy of the both to facilitate the choice.
Methodology: This prospective, randomized controlled trial included 60 ASA I–II patients aged 18–60 years undergoing elective surgery under general anesthesia. Participants were randomized to receive either oral clonidine (0.15 mg, Group-C, n = 30) or metoprolol (50 mg, Group-M, n = 30) two hours before surgery. Intraoperative hemodynamic parameters, estimated blood loss, surgical field quality, and postoperative outcomes including pain score, nausea incidence, recovery time, and hospital stay were recorded and statistically analyzed.
Results: Both groups maintained stable intraoperative heart rate, blood pressure, and oxygen saturation (P > 0.05). Clonidine significantly reduced intraoperative blood loss compared to metoprolol (137 ± 14.71 mL vs. 151 ± 9.94 mL, P = 0.0002) and achieved better surgical field visibility (Good field: 70% vs. 56.7%, P = 0.041). Postoperative outcomes, including pain scores, recovery time, and hospital stay, were comparable across groups (P > 0.05).
Conclusion: Clonidine and metoprolol are both effective for intraoperative hemodynamic control and safe postoperative recovery. However, clonidine demonstrates a distinct advantage in minimizing blood loss and improving surgical field quality. These findings support its preferential use in procedures where blood conservation is crucial. Larger multicentric studies are recommended to guide patient-specific drug selection in perioperative management.
Keywords: Blood loss; Clonidine; Elective surgery; Hemodynamic stability; Hospital stay; Metoprolol; Pain scores; Postoperative recovery
Citation: Sereen V.a B, Natarajan S, Arunkumar B, Shanmugasundaram S, Choudhary AK, Periasamy P. Comparative evaluation of clonidine and metoprolol for perioperative hemodynamic stability, blood loss control, and postoperative recovery in patients undergoing elective surgery: a prospective randomized controlled study. Anaesth. pain intensive care 2026;30(2):189-199. DOI: 10.35975/apic.v30i2.3126
Received: May 13, 2025; Revised: May 17, 2025; Accepted: June 07, 2025
1. INTRODUCTION
The surgical recovery duration represents a strenuous time in medical treatment where several elements from anesthetic drugs interact within surgical conditions and patient health complications. The development of elevated sympathetic activity increases heart rate together with blood pressure and vascular tone changes which represents essential concerns for this period. These pharmacological alterations lead to higher blood losses during operations and reduced exposure to the operating site and worsened post-surgical recovery times. Modern anesthesia practice depends heavily on medications that modify patients' blood pressure parameters. Clinicians use clonidine and metoprolol as standard perioperative medications but research continues regarding their specific effects on multiple aspects of surgical care. Surgeries activate two stress systems: the sympathetic nervous system and the hypothalamic-pituitary-adrenal (HPA) axis which causes elevated catecholamine release together with elevated systemic vascular resistance. Organizations which require crystal-clear operative fields and bloodless working environments face risks from these systemic vascular changes. Anesthesiologists look for pharmaceutical compounds which combine safety measures for patients with reliable blood pressure control and seamless postoperative recovery.
The central mechanism of clonidine action comes from stimulation of medullary α2-adrenergic receptors that decreases both sympathetic nerve signalling and norepinephrine concentration in plasma. The medication leads to heart rate reduction and decreased mean arterial pressure and decreased vascular tone. The oral administration of clonidine before surgery proved effective for improving intraoperative blood pressure stability while reducing surgical bleeding in functional endoscopic sinus surgery patients according to Puthenveettil et al. (2015).1 The research by Choudhary et al. (2024) demonstrated that clonidine administration produced better operative field views and maintained better blood pressure steady states in otolaryngology procedures.2
The sedative and analgesia-sparing qualities of clonidine help decrease opioid consumption thereby enhancing surgical anesthetic emergence while improving patient satisfaction. The clinical advantages of these effects work specifically well for patients undergoing day-care and ambulatory surgeries because they need early postoperative recovery before being discharged. The administration of clonidine before laparoscopic cholecystectomy led to decreased anesthetic requirements and better heart condition results than placebo according to Ahmed et al. (2016).3
The cardiac protective measures offered by metoprolol derive from its mechanism which blocks β1-adrenergic receptors specifically in heart muscle tissue. The pharmacodynamic properties of negative chronotropic and inotropic action decrease myocardial oxygen need which makes metoprolol a preferred medicine for patients with ischemic or arrhythmic risks in the perioperative period. More than 8,000 patients in the Devereaux et al. (2008) POISE trial underwent non-cardiac surgery and indicated that perioperative metoprolol decreased myocardial infarction occurrence. Stroke happened more frequently and patients faced increased mortality risk because hypotension and bradycardia occurred during treatment.4 The clinical application of beta-blockers in surgery now depends on patient risk level and medical history as well as specific medication requirements. The results from MaVS demonstrate that metoprolol administration effectively managed heart rate but incidents of hypotension as well as delayed recovery appeared more often in patients treated with metoprolol compared to controls.5 The interest has grown to study clonidine as an alternative agent because these studies discovered cardiovascular stability effects comparable to metoprolol with reduced complications.
Different studies measured the operation-based performance results between clonidine therapy and metoprolol treatment within controlled surgical settings. In a surgical experiment Gohil et al. (2013) documented that clonidine-treated patients presented both lower bleeding scores and superior field grading than patients who received metoprolol or diazepam treatment especially during minimally bleeding surgeries.6 The research by Meena et al. (2024) showed clonidine achieved two benefits during laparoscopic procedures because it enhanced visibility and decreased the need for volatile anesthetic drugs.7
The peripheral vasoconstriction property of clonidine which results from central sympatholysis successfully decreases surgical bleeding and suction volume during surgical interventions. Recent outcomes from Wawrzyniak et al. (2013) demonstrated that premedicating patients with clonidine produced superior operative visibility compared to control patients when using total intravenous anesthesia.8 Clonidine stands out as an ideal medication for performing successful surgeries in otolaryngology and neurosurgery departments because of its specific properties.
Postoperative benefits from clonidine treatment continue because the drug minimizes sympathetic overreactions and defends against hypertension while decreasing patients' need for pain medicines. The preoperative administration of clonidine to patients yielded enhanced examination outcomes without detrimental opioid usage after surgery according to Sung et al. (2000) as recorded in.9 High heart rate control from metoprolol treatment exists but this drug does not provide sedation thus patients usually need extra medications to manage surgery-related pain and anxiety.
Numerous research findings continue to exist in separate sections since researchers use diverse study plans which leads to varied sample counts and assessment approaches. Research on the comparison of these drugs mainly concentrates on particular types of operations while using non-unified measures for blood loss evaluation and surgical field condition assessments. Existing trials evaluate least both intraoperative and postoperative outcomes separately which makes it difficult to determine the best agent.
The research used a randomized controlled experimental design to directly measure the effects between preoperative use of oral clonidine in 0.15 mg doses versus oral metoprolol in 50 mg doses for patients receiving general anesthetic during scheduled surgical procedures. The main research targets evaluate intraoperative blood pressure management and blood loss amounts and surgical site condition after completion of surgical procedures. The study evaluates postoperative results including recovery time as well as visual analog pain scores and frequencies of nausea and time to first anesthetic requirements and duration of hospital stay. This investigation provides a direct comparison between clonidine and metoprolol through standardized measurements in order to deliver practical findings about perioperative utilization. Studies into the variations between clonidine and metoprolol pharmacodynamics will enable better decision-making for individual drug choices and improve the delivery of perioperative care to different patient groups.
2. METHODOLOGY
The study obtained Institutional Ethics Committee authorization and the required Clinical Trials Registry of India (CTRI/2022/01/039572) registration to run for 15 months. Patients were enrolled following written informed consent. The study enrolled adults who met the requirements of belonging to between 18 years and 60 years of age with an American Society of Anesthesiologists (ASA) physical status classification at level I or II. The study excluded patients who had cardiovascular, renal, hepatic, respiratory conditions along with beta-blocker or clonidine usage within the past month and pregnant or breastfeeding women and those with contraindicated to general anesthesia. The necessary sample size resulted from power calculation which built upon an earlier research comparing clonidine and metoprolol effects on intraoperative blood loss. The determined minimum participant count for each group reached 26 individuals to establish significant statistical differences with these parameters: 80% power and 0.05 alpha error and 0.8 effect size. A total of 60 patients were recruited for this study to account for potential dropouts with equal numbers in each group (Group-C clonidine n=30 + Group-M metoprolol n=30). Randomization occurred through the use of computer-generated block methods. The allocation sequence remained hidden with sealed opaque envelopes that were opened during surgery times. The staff who gave premedication medications were absent from both intraoperative observation tasks and postoperative evaluation procedures. Double blinding between both data collectors and the treated subject enabled researchers to conduct a study design with blind conditions. Before surgical operations all patients received instructions to skip eating the night before. The participants received their assigned medications two hours prior to their scheduled surgery on the surgical day. The participants in Group-C received 0.15 mg of clonidine as an oral medication along with 30 mL of water while Group-M participants took 50 mg oral metoprolol with 30 mL water. All patients received intravenous administration of glycopyrrolate 0.2 mg combined with ondansetron 8 mg as standard premedication procedure before receiving anesthesia. Standard operating room monitor applications included electrocardiogram together with non-invasive blood pressure measurement and pulse oximetry. Baseline readings were recorded. The patient received a combination of intravenous medications including fentanyl 2 mcg/kg along with propofol 2 mg/kg and vecuronium 0.1 mg/kg so that endotracheal intubation could be accomplished. During maintenance anesthesia the patients received a 66% nitrous oxide mix with 33% oxygen and isoflurane 0.8–1.0%. The infiltration of Ringer lactate started at 10 mL/kg/hour for the first hour before reducing to 5 mL/kg/hour. Heart rate along with systolic pressure and diastolic pressure and respiratory rate and oxygen saturation received focused measurement points for baseline pre-induction then immediately upon induction and regularly from minutes 0 through 20 then at 60 and 120 and 180 minutes.
The measurement of intraoperative blood loss occurred through a specific method which used hemoglobin assessment. Surgery commenced with heparin (1:250,000) added to the suction canister to prevent clotting formation. Researchers recorded all fluid matter in the suction bottle after completing the surgical procedure. The estimation of blood loss involved using the patient's mean hemoglobin value and collected fluid hemoglobin concentration according to the standard calculation.
The operating surgeon rated surgical field quality independently through the surgical rating scale known as Average Category Scale (ACS) developed by From me and Boeza art. According to the Average Category Scale the operative field quality receives Good (ACS 0–1, minimal or no suction needed) grading or Fair (ACS 2–3, intermittent suction required) and Poor (ACS 4–5, continuous suction needed due to bleeding) ratings.
The study measured recovery time as well as VAS pain scores and both nausea frequency and requirement for postoperative analgesia and time-to-first analgesia and lasted until the hospital stay ended. Intravenous paracetamol 1 g functioned as rescue analgesia that doctors administered through an IV to patients when their VAS score reached 4 or more.
The data collected went into a master sheet designed before analysis while EPI Info version 7.2 performed the statistical analysis. Assessment of continuous variables for normal distribution occurred before statistical analysis with either the independent samples t-test or Mann–Whitney U test based on data characteristics. The analysis of categorical variables involved Chi-square or Yates' corrected Chi-square testing methods. The research determined significant statistical results from p-values that remained below 0.05.
3. RESULTS
The demographic and baseline characteristics of the study participants were comparable between Group-C and Group-M, as shown in Table 1. The mean age, gender distribution, ASA classification, height, weight, and preoperative laboratory parameters, including hemoglobin levels, random blood sugar, serum creatinine, and electrolytes, showed no statistically significant differences (P > 0.05 for all variables).
Preoperative screening assessments, such as ECG and chest X-ray findings, indicated a high percentage of normal results in both groups, with no significant between-group variation. These findings confirm that both study groups were well-matched at baseline, minimizing potential confounding effects on hemodynamic and recovery outcomes.
The similarity in demographic, physical, and biochemical characteristics between the two groups confirms a well-balanced randomization process, ensuring a valid comparison of perioperative hemodynamic and recovery outcomes.
| Table 1: Hemodynamic and respiratory parameters during surgery: Group-C: Clonidine (N = 30), Group-M: metoprolol (N = 30) | ||||||||||
| HR (bpm) | SBP (mmHg) | DBP (mmHg) | RR (breaths/min) | SpO₂ (%) | ||||||
| Time Point (min) | Group-C | Group-M | Group-C | Group-M | Group-C | Group-M | Group-C | Group-M | Group-C | Group-M |
| Preoperative | 84.86 ± 12.07 | 81.13 ± 13.68 | 124.8 ± 13.8 | 119.7 ± 13.7 | 74.96 ± 10.01 | 72.13 ± 9.78 | 16.2 ± 1.8 | 16.5 ± 1.6 | 98.1 ± 1.2 | 98.0 ± 1.1 |
| 0 | 84.63 ± 14.05 | 78.83 ± 12.23 | 116.8 ± 14.11 | 109.8 ± 15.43 | 73.56 ± 11.07 | 70.46 ± 10.99 | 16.0 ± 1.7 | 16.3 ± 1.8 | 98.2 ± 1.1 | 98.1 ± 1.0 |
| 5 | 84.00 ± 14.73 | 79.16 ± 12.40 | 118.66 ± 20.2 | 104.3 ± 12.08 | 69.13 ± 13.1 | 66.84 ± 12.7 | 15.9 ± 1.9 | 16.1 ± 1.5 | 98.3 ± 1.0 | 98.2 ± 1.1 |
| 10 | 84.13 ± 12.70 | 78.86 ± 14.55 | 113.5 ± 18.58 | 103.0 ± 9.7 | 67.06 ± 15.81 | 65.92 ± 13.44 | 15.8 ± 1.8 | 16.0 ± 1.6 | 98.1 ± 1.2 | 98.1 ± 1.1 |
| 15 | 85.46 ± 11.47 | 80.53 ± 15.59 | 113.5 ± 18.86 | 109.56 ± 17.69 | 67.2 ± 13.61 | 66.1 ± 14.32 | 15.7 ± 1.6 | 15.9 ± 1.7 | 98.2 ± 1.2 | 98.1 ± 1.0 |
| 20 | 87.13 ± 10.51 | 80.50 ± 13.62 | 112.4 ± 16.99 | 105.1 ± 15.4 | 65.4 ± 12.73 | 64.8 ± 12.65 | 15.6 ± 1.8 | 15.8 ± 1.6 | 98.1 ± 1.2 | 98.0 ± 1.1 |
| 60 | 79.40 ± 10.6 | 76.83 ± 14.95 | 104.0 ± 19.37 | 97.9 ± 10.96 | 61.16 ± 15.2 | 59.92 ± 14.75 | 15.5 ± 1.7 | 15.6 ± 1.5 | 98.3 ± 1.0 | 98.2 ± 1.1 |
| 120 | 84.80 ± 12.7 | 81.13 ± 13.68 | 124.8 ± 13.48 | 119.7 ± 13.72 | 74.96 ± 10.01 | 72.18 ± 10.22 | 15.6 ± 1.9 | 15.8 ± 1.7 | 98.2 ± 1.1 | 98.1 ± 1.0 |
| 180 | 79.40 ± 10.6 | 76.80 ± 14.95 | 104.0 ± 19.37 | 97.9 ± 10.96 | 61.1 ± 15.2 | 59.4 ± 14.62 | 15.4 ± 1.6 | 15.7 ± 1.5 | 98.3 ± 1.0 | 98.2 ± 1.1 |
The intraoperative hemodynamic and respiratory parameters were monitored at multiple time points, including preoperative (Preop), immediately after induction (0 min), and at subsequent intervals up to 180 minutes. As shown in Table 2, and Figure 1 both Group-C and Group-M maintained stable heart rates, systolic blood pressure, diastolic blood pressure, respiratory rates, and oxygen saturation levels throughout the surgical period.
No statistically significant differences were observed between the two groups for any hemodynamic or respiratory parameters at any time point (P > 0.05 for all comparisons). These results indicate that both clonidine and metoprolol provide comparable intraoperative cardiovascular stability, reinforcing their effectiveness in maintaining perioperative hemodynamic control.
Figure 1: Hemodynamic parameters in both groups
Both groups exhibited a gradual reduction in heart rate and blood pressure over time, with no clinically significant variations between Group-C and Group-M. This indicates that both drugs effectively control intraoperative hemodynamics, ensuring stable cardiovascular function throughout surgery. Respiratory function remained stable in both groups, with no significant respiratory depression observed. Oxygen saturation levels were consistently above 98%, reinforcing the safety profile of both drugs in maintaining adequate oxygenation during the perioperative period. Overall, the findings in Table 2 confirm that clonidine and metoprolol provide stable intraoperative hemodynamic and respiratory parameters, ensuring adequate cardiovascular control without significant adverse fluctuations.
The figure demonstrates that both clonidine and metoprolol effectively maintain intraoperative hemodynamic stability. Heart rate, systolic and diastolic blood pressure, and respiratory rate show a gradual decline over time, with no significant differences between groups. Clonidine exhibited slightly higher heart rate and BP trends, while respiratory rates remained consistent in both groups. These findings confirm that both drugs provide comparable and safe perioperative hemodynamic control.
| Table 2: Demographic and baseline characteristics of study participants | |||
| Parameter | Group-C
(n = 30) |
Group-M
(n = 30) |
P-value |
| Mean Age (years) | 37.07 ± 11.62 | 35.83 ± 10.77 | 0.6785 |
| Gender (Female / Male) | 20 / 10 (66.67% / 33.33%) | 23 / 7 (76.67% / 23.33%) | 0.356 |
| ASA Grade I / II | 27 / 3 (90% / 10%) | 26 / 4 (86.67% / 13.33%) | > 0.05 |
| Height (cm) | 156.16 ± 7.12 | 155.86 ± 8.51 | 0.9941 |
| Weight (kg) | 62.09 ± 10.57 | 59.22 ± 9.69 | 0.1185 |
| Preoperative Hemoglobin (g%) | 11.86 ± 2.51 | 11.73 ± 2.08 | 0.922 |
| Random Blood Sugar (mg/dL) | 96.4 ± 14.2 | 98.1 ± 15.0 | 0.523 |
| Serum Creatinine (mg/dL) | 0.89 ± 0.12 | 0.91 ± 0.14 | 0.617 |
| Serum Sodium (mEq/L) | 138.2 ± 3.5 | 137.8 ± 3.8 | 0.752 |
| Serum Potassium (mEq/L) | 4.2 ± 0.4 | 4.1 ± 0.3 | 0.644 |
| ECG Normal / Abnormal | 28 / 2 (93.33% / 6.67%) | 27 / 3 (90% / 10%) | 0.482 |
| Chest X-ray Normal / Abnormal | 29 / 1 (96.67% / 3.33%) | 28 / 2 (93.33% / 6.67%) | 0.395 |
| Data presented as Mean ± SD or n (%); P < 0.05 is significant | |||
3.1. Hemoglobin and Blood Loss Indicators
As shown in Table 3, preoperative and postoperative hemoglobin levels, mean hemoglobin concentration, and haematocrit values were comparable between the two groups (P > 0.05), indicating similar overall hemoglobin stability. However, suction volume and total blood loss were significantly lower in Group-C than in Group-M, both before and after adjusting for haematocrit levels (P < 0.05).
| Table 3: Hemoglobin and blood loss indicators | |||
| Parameter | Group-C | Group-M | P-value |
| Preoperative Hemoglobin (g%) | 11.86 ± 2.51 | 11.73 ± 2.08 | 0.922 |
| Postoperative Hemoglobin (g%) | 11.4 ± 2.28 | 10.93 ± 2.09 | 0.3995 |
| Mean Hemoglobin (g%) | 11.32 ± 2.12 | 10.96 ± 2.15 | 0.425 |
| Hemoglobin in Canister (g%) | 8.16 ± 1.76 | 7.66 ± 1.68 | 0.292 |
| Suction Volume (ml) | 193.76 ± 34.53 | 219.33 ± 31.53 | 0.0011 |
| Blood Loss (ml) | 137 ± 14.71 | 151 ± 9.94 | 0.0002 |
| Haematocrit Preop (%) | 35.2 ± 3.1 | 34.8 ± 2.9 | 0.521 |
| Haematocrit Postop (%) | 33.8 ± 2.9 | 32.9 ± 3.0 | 0.486 |
| Estimated Blood Loss Adjusted for Haematocrit (ml) | 140.3 ± 12.8 | 155.7 ± 11.5 | 0.038 |
Table 4 further supports these findings, demonstrating a higher percentage of "Good" surgical field conditions in the clonidine group (70%) compared to metoprolol (56.67%) (P = 0.041). This suggests that clonidine contributes to better operative visibility and reduced bleeding, reinforcing its potential advantage in managing intraoperative blood loss.
Clonidine resulted in lower blood loss, improved surgical field conditions, and better intraoperative visibility, while hemoglobin levels remained stable in both groups.
| Table 4: Surgical Field Quality Assessment (ACS Grading) | |||
| ACS Grade | Group A (Clonidine) | Group B (Metoprolol) | P-value |
| Good (ACS 0-1) | 21 (70 | 17 (56.67) | 0.041 |
| Fair (ACS 2-3) | 8 (26.67) | 10 (33.33) | - |
| Poor (ACS 4-5) | 1 (3.33) | 3 (10 | - |
3.2. Hemodynamic Stability and Time-to-Event Analysis
The intraoperative hemodynamic stability was assessed through repeated measures ANOVA, correlation analysis, variability measures (CV), and time-to-event analysis for hemodynamic instability. As shown in Table 5, both clonidine (Group-C) and metoprolol (Group-M) maintained stable heart rate, systolic blood pressure, diastolic blood pressure, respiratory rate, and oxygen saturation over time, with no significant intraoperative fluctuations observed (P > 0.05). Correlation analysis revealed a moderate positive correlation between heart rate and blood pressure at different time points, with no statistically significant differences between the two groups (P > 0.05). This supports the predictable cardiovascular response under both treatment conditions. Similarly, the coefficient of variation (CV) for heart rate, systolic blood pressure, and diastolic blood pressure showed low variability, reinforcing the stability and reliability of both drugs in perioperative cardiovascular control (P > 0.05).
Time-to-event analysis demonstrated that the incidence of BP drops, heart rate spikes, respiratory rate changes, and oxygen saturation drops was comparable between the two groups, with no statistically significant differences (P > 0.05). These findings suggest that neither drug increases the risk of hemodynamic instability, supporting their clinical safety and efficacy in perioperative management.
The findings in Table 5 confirm that both clonidine and metoprolol provide consistent perioperative hemodynamic stability, with no significant differences in trends, correlation patterns, or variability measures. The similar time-to-event analysis results further reinforce the clinical reliability of both drugs in maintaining cardiovascular stability without increasing the risk of hemodynamic instability.
| Table 5: Hemodynamic stability and time-to-event analysis | |||
| Parameter / Time | Group-C | Group-M | P-value |
| Heart Rate (F-Statistic) | 1.53 | 1.53 | 0.14 |
| Systolic Blood Pressure (F-Statistic) | 1.11 | 1.11 | 0.22 |
| Diastolic Blood Pressure (F-Statistic) | 0.97 | 0.97 | 0.34 |
| Respiratory Rate (F-Statistic) | 1.18 | 1.18 | 0.21 |
| Oxygen Saturation (F-Statistic) | 0.76 | 0.76 | 0.42 |
| Preop Correlation (HR & BP) | 0.45 | 0.42 | 0.67 |
| 0 min Correlation | 0.48 | 0.43 | 0.62 |
| 10 mins Correlation | 0.52 | 0.49 | 0.59 |
| 30 mins Correlation | 0.46 | 0.44 | 0.64 |
| 120 mins Correlation | 0.51 | 0.53 | 0.73 |
| Heart Rate Variability (CV) | 0.13 | 0.14 | 0.31 |
| Systolic BP Variability (CV) | 0.11 | 0.12 | 0.27 |
| Diastolic BP Variability (CV) | 0.14 | 0.13 | 0.34 |
| BP Drop (>20% from Baseline) | 5 events | 7 events | 0.42 |
| Heart Rate Spike (>20 bpm) | 3 events | 4 events | 0.55 |
| Respiratory Rate Change | 2 events | 2 events | 1.00 |
3.3. SubGroup-Cnalysis by Demographics
The subGroup-Cnalysis examined heart rate and systolic blood pressure variations across different demographic categories, including age (<40 vs. ≥40 years), gender, and ASA classification (I vs. II). As shown in Table 6, no statistically significant differences were observed between Group-C and Group-M across all subgroups (P > 0.05). Among participants younger than 40 years, the heart rate and systolic blood pressure values were slightly higher in the clonidine group compared to metoprolol, but the differences were not statistically significant (P = 0.15 and P = 0.18, respectively). Similarly, in participants aged 40 years or older, both parameters remained comparable between the two groups (P = 0.22 and P = 0.16, respectively). Gender-based comparisons revealed similar heart rate trends in both male and female participants, with no significant variations (P = 0.33 and P = 0.21, respectively). Additionally, ASA grade I and II patients exhibited similar systolic blood pressure values between the groups, indicating that both clonidine and metoprolol provide stable hemodynamic control across different ASA classifications.
These findings confirm that both drugs maintain consistent hemodynamic stability, irrespective of age, gender, or ASA classification, supporting their generalizability and safety for a diverse perioperative patient population.
The subGroup-Cnalysis in Table 6 reinforces that clonidine and metoprolol exhibit consistent hemodynamic effects across different demographic categories, with no statistically significant differences observed. This supports their widespread applicability and safety in perioperative hemodynamic management.
| Table 6: Sub Group-C analysis by demographics | ||||
| Subgroup | Parameter | Group-C | Group-M | P-value |
| Age < 40 | Heart Rate (beats/min) | 83.5 ± 11.8 | 80.1 ± 12.3 | 0.15 |
| Systolic BP (mmHg) | 123.4 ± 14.2 | 118.5 ± 13.7 | 0.18 | |
| Age ≥ 40 | Heart Rate (beats/min) | 84.9 ± 12.5 | 82.6 ± 14.1 | 0.22 |
| Systolic BP (mmHg) | 125.7 ± 13.6 | 120.4 ± 13.2 | 0.16 | |
| Gender: Male | Heart Rate (beats/min) | 82.9 ± 10.4 | 81.2 ± 13.8 | 0.33 |
| Gender: Female | Heart Rate (beats/min) | 85.2 ± 12.9 | 82.1 ± 13.2 | 0.21 |
| ASA Grade I | Systolic BP (mmHg) | 122.6 ± 13.9 | 118.3 ± 14.4 | 0.24 |
| ASA Grade II | Systolic BP (mmHg) | 124.9 ± 14.1 | 121.4 ± 13.7 | 0.26 |
3.4. Postoperative Outcomes Analysis
The postoperative recovery parameters, including recovery time, pain scores, nausea incidence, and hospital stay duration, were assessed between Group-C and Group-M. As presented in Table 7, there were no significant differences in recovery time (P = 0.48), pain scores (P = 0.38), nausea incidence (P = 0.72), or hospital stay duration (P = 0.55) between the groups.
Additionally, postoperative analgesic requirements and time to first analgesia administration were evaluated, showing no significant variations between the groups (P > 0.05). The comparable analgesic consumption and similar timing of initial analgesia administration further suggest equivalent pain management effectiveness between clonidine and metoprolol. These findings indicate that both drugs provide similar postoperative recovery profiles, without adversely affecting pain control, nausea incidence, or length of hospital stay, and effective in differences in recovery time, pain management, nausea incidence, or hospital stay duration. These results reinforce that both drugs are equally safe and effective in perioperative pain control and recovery. Figure 3 illustrates the trend of oxygen saturation levels over time in both groups. Oxygen saturation perioperative pain control and recovery.
Figure 3: Line graph for oxygen saturation over time
Figure 3 illustrates the trend of oxygen saturation levels over time in both groups. Oxygen saturation remained consistently high throughout the intraoperative period, with no clinically significant desaturation observed in either group. These findings indicate that both clonidine and metoprolol maintain stable respiratory function and are safe with respect to preserving adequate oxygenation during supporting their clinical utility in perioperative care. The findings in Table 7 confirm that clonidine and metoprolol providecomparable postoperative outcomes, with no significant differences in recovery time, pain management, nausea incidence, or hospital stay duration. These results reinforce that both drugs are equally safe surgery.
| Table 7: Analysis of Postoperative Outcomes | ||||
| Outcome | Group A (Clonidine) | Group B (Metoprolol) | Statistical Analysis | P-Value |
| Recovery Time (mins) | 45.3 ± 10.5 | 46.8 ± 9.7 | T-test | 0.48 |
| Pain Score (VAS 0-10) | 3.2 ± 1.1 | 3.5 ± 1.0 | Mann-Whitney U | 0.38 |
| Postoperative Nausea (%) | 10% | 12% | Chi-square test | 0.72 |
| Length of Hospital Stay (days) | 2.5 ± 0.8 | 2.6 ± 0.7 | T-test | 0.55 |
| Postoperative Analgesic Requirement (mg) | 80.5 ± 12.3 | 85.2 ± 14.1 | T-test | 0.42 |
| Time to First Analgesia (hrs) | 4.2 ± 1.6 | 3.9 ± 1.8 | T-test | 0.47 |
4. DISCUSSION
An evaluation through randomized controlled trial examined the surgical effectiveness of clonidine pills and metoprolol for adult patients who underwent general anesthesia procedures. The administered drugs successfully stabilized the patient's intraoperative blood pressure levels and they recovered equally well postoperatively. The study showed that clonidine proved superior to other medications by reducing surgical field blood loss and producing better surgical conditions.
Results indicated that after blood pressure and heart rate and oxygen saturation stayed consistent both teams received better surgical field assessment but clonidine group experienced less bleeding during operations The research shows that clonidine effectively reduces intraoperative bleeding because it causes central sympatholysis and blocks catecholamine release.11 The study by Devendran et al. established that clonidine generated superior operative visibility and caused more effective bleeding reduction during FESS in comparison to metoprolol.12 The heart rate regulation benefits of metoprolol equated those of other β1-adrenergic blockers yet the drug proved ineffective in improving aurgical field condition variables similarly. The study results matched previous research by Choudhary et al. because clonidine provided superior field quality with lower anesthetic needs despite maintaining stable heart dynamics.13,14 Some research by Dhakne et al. revealed better blood loss reduction results showed clonidine produced better treatment outcomes in all respects including bleeding control and operative visibility and anesthetic efficiency for otolaryngological operations according to studies in Table 3.17-21 Menezes et al. demonstrated that clonidine stabilizes blood pressure after surgery while preventing hypertension rebound whereas metoprolol showed no such effect according to their report.The examined groups displayed equivalent postoperative results when measuring pain scores and recovery duration together with nausea frequency and hospitalization length. The analysis from Sung et al. confirmed that patients received less analgesics after surgery but their emergence time and hospital stay were not affected by clonidine administration.22 The study results showed no significant differences probably because the pain management protocol was uniform and surgeries were short in duration.
The subgroup evaluation demonstrated that the outcomes between the drugs remained equivalent for patients from all age categories and both genders and all ASA levels one through two. Consequently, both drugs proved secure and effective for this wide patient population range. Research by Wawrzyniak et al. confirmed that clonidine improves surgical field quality
5. LIMITATIONS
The research encountered some limitations in its design. The research included only one medical facility and its participant numbers were limited while also omitting patients who demonstrated high surgical risk factors (ASA III–IV). The surgical field grade assessments used an established scoring method yet depended on subjective measurements. The study failed to evaluate the delayed cardiovascular outcomes together with sedation effects and functional recovery measurements.
6. CONCLUSION
The results of this randomized controlled trial proved that both oral clonidine (0.15 mg) and oral metoprolol (50 mg) showed effectiveness for maintaining intraoperative hemodynamic stability as well as guaranteeing secure postoperative recovery in elective surgery patients who were ASA I–II under general anesthesia. The main benefit of clonidine stood out by substantially decreasing blood loss during operations and improving surgery visibility without generating extra negative side effects. The study results endorse clonidine's selection over other options for medical procedures which depend on controlled bleeding. The clinical consequences of our study results have substantial importance. Clonidine provides threefold advantages during surgery because it reduces stress reactions while performing pain management and sedation functions particularly when visibility matters and blood conservation is essential. The affordability along with oral availability of clonidine makes this medication ideal for healthcare institutions serving the public sector or operating with resource restrictions.
- Data availability
- Conflict of interest
- Funding
- Authors’ contribution
SN: Patient Recruitment, Clinical Monitoring, Manuscript Review
BA: Study Design Supervision, Methodological Guidance
SS: Data Analysis, Interpretation, Correspondence, Final Manuscript Approval
AKC: Statistical Analysis, Pharmacological Input, Reference Validation
PP: Physiological Correlation, Data Interpretation, Proofreading
11. REFERENCES
- Puthenveettil N, Rajan S, Kumar L, Nair SG. A comparison of effects of oral premedication with clonidine and metoprolol on intraoperative hemodynamics and surgical conditions during functional endoscopic sinus surgery.Anesth Essays Res. 2015;9(1):38-42.
- Choudhary A, Sharma K, Gupta R. Comparative evaluation of oral clonidine and metoprolol as premedication for FESS.Indian J Clin Anaesth. 2024;11(1):55-60.
- Ahmed AA, Mohamed SA. The effect of oral clonidine on hemodynamic changes during laparoscopic cholecystectomy.J Evid Based Med Healthc. 2016;3(12):432-6.
- Devereaux PJ, Yang H, Yusuf S, et al. Effects of extended-release metoprolol succinate in patients undergoing non-cardiac surgery (POISE trial): a randomised controlled trial.Lancet. 2008;371(9627):1839–47.
- Yang H, Raymer K, Butler R, Parlow J, Roberts R. The effects of perioperative beta-blockade: results of the Metoprolol after Vascular Surgery (MaVS) study.Am Heart J. 2006;152(5):983-90.
- Gohil M, Patel P, Patel V. Comparison of oral diazepam, clonidine, and metoprolol in functional endoscopic sinus surgery.Int J Basic Clin Pharmacol. 2013;2(5):589-93.
- Meena K, Bhargava AK, Sharma V. Hemodynamic effects of oral clonidine in laparoscopic surgery.Indian Anaesth Forum. 2024;25(1):24-30.
- Wawrzyniak K, Kusza K, Cywinski JB, Burduk PK. Premedication with clonidine before TIVA optimizes surgical field visualization.Rhinology. 2013;51(3):259–64.
- Sung CS, Lin SH, Chan KH, Chang WK, Chow LH, Lee TY. Effect of oral clonidine premedication on perioperative hemodynamic response and postoperative analgesic requirement.Acta Anaesthesiol Sin. 2000;38(1):23–9.
- Maze M, Tranquilli W. Alpha-2 adrenoceptor agonists: defining the role in clinical anesthesia.Anesthesiology. 1991;74(3):581–605.
- Filos KS, Goudas LC, Patroni O, Polyzou V. Hemodynamic and analgesic profile of clonidine as a premedication in general anesthesia.Anesth Analg. 1994;79(4):802–8.
- Wickham AJ, Highton DT, Clark S, et al. Treatment threshold for intra-operative hypotension in clinical practice—a prospective cohort study in older patients in the UK.Anaesthesia. 2022;77(2):153-163.
- Wesselink EM, Kappen TH, Torn HM, et al. Intraoperative hypotension and the risk of postoperative adverse outcomes: a systematic review.Br J Anaesth. 2018;121(4):706–721.
- Saugel B, Sessler DI. Perioperative blood pressure management.Anesthesiology. 2021;134(2):250–261.
- Ackland GL, Brudney CS, Cecconi M, et al. PeriOperative Quality Initiative consensus statement on the physiology of arterial blood pressure control in perioperative medicine.Br J Anaesth. 2019;122(5):542–551.
- Sanders RD, Hughes F, Shaw A, et al. PeriOperative Quality Initiative consensus statement on preoperative blood pressure, risk and outcomes for elective surgery.Br J Anaesth. 2019;122(5):552–562.
- Choudhary A, Sharma K, Gupta R. Comparative evaluation of oral clonidine and metoprolol as premedication for FESS.Indian J Clin Anaesth. 2024;11(1):55–60.
- Dhakne P, Jaiswal M, Mankar S. Role of clonidine versus metoprolol in controlling blood loss and surgical condition in FESS.Int J Med Anesth. 2023;6(1):12–7.
- Devendran K, Iyer SS, Vasudevan A. Clonidine premedication and its impact on intraoperative bleeding and visibility in nasal surgery.Indian J Otolaryngol Head Neck Surg. 2023;75(2):175–9.
- Menezes A, Pandit S, D’Souza D. Comparison of oral clonidine and metoprolol in ENT head and neck surgeries: a clinical study.J Clin Diagn Res. 2021;15(9):UC01–UC04.
- Keshari S, Rajput S, Meena K. Effectiveness of oral clonidine and metoprolol premedication on surgical field quality in FESS: a comparative study.Asian J Anaesth Clin Res. 2024;8(1):44–9.
- Sessler DI, Bloomstone JA, Aronson S, et al. PeriOperative Quality Initiative consensus statement on intraoperative blood pressure, risk and outcomes for elective surgery.Br J Anaesth. 2019;122(5):563–574.
- McEvoy MD, Gupta R, Koepke EJ, et al. PeriOperative Quality Initiative consensus statement on postoperative blood pressure, risk and outcomes for elective surgery.Br J Anaesth. 2019;122(5):575–586.
- Miller TE, Shaw AD, Mythen MG, et al. Evidence-based perioperative medicine comes of age: the PeriOperative Quality Initiative (POQI): the 1st consensus Conference of the PeriOperative Quality Initiative (POQI).Perioper Med (Lond). 2016;5:26.
- Prowle JR, Forni LG, Bell M, et al. Postoperative acute kidney injury in adult non-cardiac surgery: joint consensus report of the Acute Disease Quality Initiative and PeriOperative Quality Initiative.Nat Rev Nephrol. 2021;17:605–618.
- Alonso-Coello P, Schunemann HJ, Moberg J, et al. GRADE Evidence to Decision (EtD) frameworks: a systematic and transparent approach to making well informed healthcare choices. 1: Introduction.BMJ. 2016;353:i2016.