Rr Sinta Irina 1* , Arsil Radiansyah 2 , Heru Kurniawan 3
Authors affiliations:
Objective: Responses to stress following craniotomy can vary from elevated hemodynamics to elevated cortisol levels in the body. Intubation is a major factor that must be considered during the induction of neuroanesthesia. Magnesium sulfate has the advantage of maintaining the stability of brain autoregulation and is neuroprotective.
Methodology: The study was conducted after receiving ethical clearance from the Health Research Ethics Committee of the University of North Sumatra (No. 94/KEPK/USU/2024). The trial was registered at ClinicalTrials.gov under the identifier NCT06516861 on July 24, 2024. We included 30 patients, aged 18–65 years; body mass index (BMI) 18.5–29.9 kg/m², consecutively, undergoing craniotomy at our hospital. The patients were randomly divided into three equal groups; patients who received lidocaine, or MgSO4 and a control group, who received normal saline as a placebo. Post-induction and intubation, hemodynamic parameters, including systolic blood pressure, diastolic blood pressure, mean arterial pressure (MAP), and heart rate, were measured at 3, 5, 7, and 10 min (T1, T2, T3, and T4) following intubation. Serum cortisol levels were assessed at baseline (T0) and post-intubation.
Results: There were significant differences between the three groups with hemodynamic and serum cortisol levels found to be lower in the lidocaine group. (P = 0.001). Significant differences were observed among the three groups, with the lidocaine group showing lower hemodynamic parameters (systolic blood pressure, diastolic blood pressure, mean arterial pressure, heart rate) and serum cortisol levels (P = 0.001).
Conclusion: Intravenous administration of lidocaine 1.5 mg/kg is more effective in attenuating the stress response in the form of increased blood pressure, heart rate, and serum cortisol levels due to laryngoscopy and intubation in patients undergoing craniotomy than intravenous administration of MgSO4 30 mg/kg
Keywords: Craniotomy; Intubation; Lidocaine; MgSO4
Citation: Irina RS, Radiansyah A, Kurniawan H. Comparison of magnesium sulfate and lidocaine on hemodynamic response and cortisol levels after intubation in patients undergoing craniotomy. Anaesth. pain intensive care 2025;30(1):88-94. DOI: 10.35975/apic.v30i1.3107
Received: May 09, 2025; Revised: October 26, 2024; Accepted: January 01, 2025
Craniotomy, a neurosurgical procedure involving the opening or removal of parts of the skull, is performed to address various intracranial conditions.1 In craniotomies, maintaining cerebral perfusion pressure (CPP), cerebral blood flow (CBF), and cerebral metabolic rate of oxygen (CMRO2) is critical during neuro-anesthesia induction to prevent secondary brain injury.2 Under general anesthesia, the primary goals are to optimize brain metabolism and ensure adequate brain oxygenation, often achieved through endotracheal intubation.3
Laryngoscopy and tracheal intubation are critical steps in general anesthesia induction but are associated with significant physiological stress in the patient. These procedures stimulate somatic and visceral nociceptive afferent fibers, triggering a sympathetic adrenal reflex response. This response increases neural activity in the cervical sympathetic efferent fibers, leading to heightened hemodynamic responses, including hypertension, tachycardia, and dysrhythmia.4 In craniotomy patients, these hemodynamic changes are particularly concerning as they can elevate intracranial pressure (ICP), exacerbate cerebral edema, and increase the risk of secondary brain injury due to compromised cerebral autoregulation.5
Sympathetic stimulation also elevates plasma catecholamine concentrations (e.g., adrenaline and noradrenaline), which may precipitate left ventricular failure, intracranial hemorrhage, or myocardial infarction in anesthetized patients.4 Additionally, intubation activates the hypothalamic-pituitary-adrenal (HPA) axis, stimulating the hypothalamus to release corticotropin-releasing hormone (CRH) and arginine vasopressin. These peptides trigger the secretion of adrenocorticotropic hormone (ACTH) from the anterior pituitary, which in turn stimulates cortisol release from the adrenal cortex.5,6 Elevated cortisol levels during craniotomy may exacerbate cerebral edema, increase intracranial pressure, and impair neurological recovery, necessitating interventions to mitigate this stress response. Cortisol, a primary biomarker of HPA axis activation, alongside the sympathetic adrenomedullary (SAM) system, drives the hemodynamic stress response (HDSR), increasing myocardial workload, coronary perfusion demand, and the risk of myocardial ischemia due to inadequate oxygenation.4,5
Various pharmacological agents, including opioids, calcium channel blockers, beta-blockers, alpha-2 agonists, magnesium sulfate, and local anesthetics, have been employed to mitigate the stress response during intubation.7 Intravenous lidocaine has been widely studied for its efficacy in attenuating the hemodynamic responses during laryngoscopy and intubation. While generally safe, its use requires precise dosing and careful monitoring by experienced healthcare professionals.7 Magnesium sulfate (MgSO4) acts as a physiological calcium antagonist, competing with calcium at membrane channels and modulating calcium-mediated responses. It inhibits catecholamine release from the adrenal gland and peripheral adrenergic nerve terminals, reducing stress responses.8 Additionally, MgSO4 offers neuroprotective benefits by inhibiting NMDA receptors, reducing glutamate excitotoxicity, and supporting cerebral vasodilation, which helps maintain cerebral autoregulation and protects the blood-brain barrier. In the cardiovascular system, MgSO4 promotes arteriolar vasodilation, enhances cardiac output, and may improve diastolic dysfunction with minimal impact on venous circulation.8
Previous studies, including a systematic review and meta-analysis by Cantey and Neu (2022), have demonstrated that both magnesium sulfate and lidocaine effectively attenuate post-intubation stress responses in the general population.9 However, evidence specific to patients with cerebrovascular disorders, such as those undergoing craniotomies, remains limited. Given the unique physiological challenges in this population, particularly the need to control ICP and prevent secondary brain injury, further investigations are warranted.
Therefore, this study aimed to compare the efficacy of magnesium sulfate and lidocaine in attenuating hemodynamic responses and post-intubation cortisol levels in patients undergoing craniotomy, providing insights into optimal anesthesia management for this high-risk group.
This double-blind randomized controlled clinical trial with a pre- and post-test design, including a control group, aimed to compare hemodynamic responses and post-intubation cortisol levels following the administration of intravenous magnesium sulfate (MgSO₄) versus intravenous lidocaine. The study was conducted after receiving ethical clearance from the Health Research Ethics Committee of the University of North Sumatra (ethics number 94/KEPK/USU/2024). The trial was registered at ClinicalTrials.gov under the identifier NCT06516861 on July 24, 2024. The study population comprised all patients who underwent craniotomy at our institution.
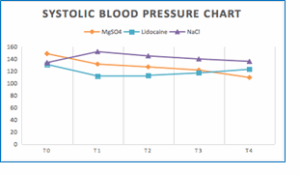
Figure 1: Comparative systolic blood pressure
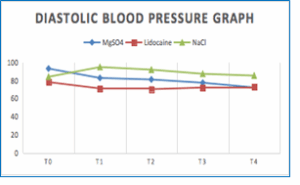
Figure 2: Comparative diastolic blood pressure
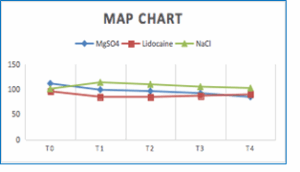
Figure 3: Comparative mean arterial pressure
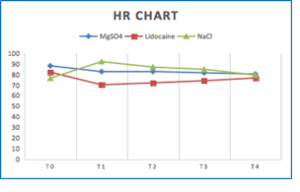
Figure 4: Comparative heart rate graph
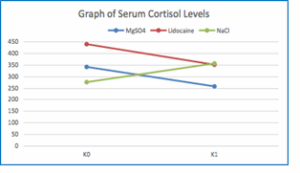
Figure 5: Comparative serum cortisol levels
The sample size was calculated using the formula for comparing two means, with an alpha of 0.05 and a power of 80%, resulting in a minimum requirement of 10 participants per group, for a total of 30 participants (10 each in the MgSO₄ group, 10 in the lidocaine group, and 10 in the control group). Subjects were selected using consecutive sampling until the required sample size was reached. Random allocation was performed using computer-based randomization via www.randomizer.org, ensuring an equal distribution across the three groups.
The study included patients who met the following inclusion criteria: aged 18–65 years; body mass index (BMI) 18.5–29.9 kg/m²; provided informed consent from the patient or their next of kin; and scheduled for elective non-traumatic craniotomy procedures, including supratentorial brain tumor evacuation, intracerebral hemorrhage evacuation, subdural hemorrhage evacuation, or cerebrovascular correction. The exclusion criteria were as follows: cardiac, hepatic, or renal disorders; pregnancy; pre-existing hypertension or hypotension before surgery; hypersensitivity to MgSO₄ or lidocaine; chronic use of corticosteroids, calcium channel blockers, magnesium-containing drugs, or opioids; high risk of difficult intubation or ventilation based on LEMON and MOANS score criteria; impaired cortisol secretion due to pituitary, hypothalamic, or adrenal gland disorders; and abnormal baseline cortisol levels (hypocortisolism or hypercortisolism) at T0 serum cortisol examination.
The participants were randomly assigned to one of three groups. Group 1 received MgSO₄ at a dose of 30 mg/kg, diluted in 20 mL of normal saline, administered over 5 min via a syringe pump and labeled as code A. Group 2 received lidocaine at a dose of 1.5 mg/kg, similarly diluted and administered, labeled as code B. The control group (code C) received 20 mL of normal saline as a placebo under identical conditions. The doses of MgSO4 and lidocaine were selected based on established clinical guidelines and prior studies demonstrating their safety and efficacy in attenuating hemodynamic responses during intubation.10,11 Specifically, the 30 mg/kg dose of MgSO₄ was chosen for its proven ability to reduce catecholamine release and maintain cerebral autoregulation in neurosurgical patients.10 The 1.5 mg/kg dose of lidocaine was selected based on its effectiveness in suppressing laryngoscopy-induced hemodynamic responses with minimal side effects.11
Post-induction and intubation, hemodynamic parameters, including systolic blood pressure, diastolic blood pressure, mean arterial pressure (MAP), and heart rate, were measured at 3, 5, 7, and 10 min (T1, T2, T3, and T4) following intubation. Serum cortisol levels were assessed at baseline (T0) and post-intubation. Patients who developed hypertension (systolic blood pressure >150 mmHg) at 5 min post-intubation were treated with titrated doses of nicardipine, starting at 0.25 mg/kg/h. Those with hypotension (systolic blood pressure < 80 mmHg) received 5–10 mg ephedrine. In cases of bradycardia (HR <50 beats/min), 0.5 mg atropine sulfate was administered.
2.1. Statistical Analysis
Data were analyzed using the SPSS version 25. Continuous variables, including hemodynamic parameters and cortisol levels, were compared across the three groups using one-way analysis of variance (ANOVA), followed by post-hoc Tukey tests for pairwise comparisons. Statistical significance was set at P < 0.05. The normality of the data distribution was assessed using the Shapiro-Wilk test, and non-parametric tests (e.g., Kruskal-Wallis test) were applied if the data were not normally distributed.
In this study, laryngoscopy and intubation were successfully performed on the first attempt in under one minute for all patients, with no intraoperative fatalities reported. The study included 30 participants, divided evenly into three groups: 10 patients in each group received either MgSO₄, lidocaine, or normal saline solution. The demographic characteristics of the groups were similar, with no significant differences in age, weight, height, or BMI (Table 1). Hemodynamic parameters showed significant differences among groups at various time points post-intubation. While MgSO4 demonstrated better control of mean arterial pressure (MAP) and heart rate (HR) at some early time points (e.g., 1-5 min, P < 0.05 vs lidocaine in select comparisons), overall attenuation of spikes and lower values in multiple parameters favored the lidocaine group (Figures 2-5). Serum cortisol levels decreased significantly in both treatment groups compared to control, with greater reduction in the lidocaine group. These findings indicate lidocaine's superior efficacy in blunting the overall intubation-induced stress response.
The mean arterial pressure (MAP) and heart rate (HR) were significantly different between the two groups at various time points. Specifically, the Magnesium group demonstrated a significantly lower MAP than the lidocaine group at 1-minute post-intubation (P = 0.02). This trend continued with significant differences observed at 3 min (0.01) and 5 min post-intubation (P = 0.03), indicating better control of MAP in the Magnesium group.
Heart rate followed a similar pattern, with the magnesium group showing a significantly lower HR at 1 min (P = 0.04), 3 min (P = 0.01), and 5 min (P = 0.02) post-intubation compared to the lidocaine group. These results suggest that magnesium sulfate is more effective n blunting the hemodynamic response to intubation in terms of both MAP and HR.
This study compared the effectiveness of MgSO4 (Group 1), lidocaine (Group 2), and NaCl 0.9% (Group 3) in attenuating the stress response in patients undergoing craniotomy. In this study, there were 30 samples divided into three groups: 10 samples in group 1, 10 samples in group 2, and 10 samples in group 3. This study analyzed the characteristics of the samples obtained based on age, height, weight, and BMI. During the study sampling, there were no respondents who met the dropout criteria, that is, patients who underwent intubation more than once, with intubation time of more than one minute, or patients who died on the operating table. This study showed that each laryngoscopy was effectively performed once in less than one minute, and there were no cases of death on the operating table.
In this study, the baseline systolic blood pressures of Groups 1, 2, and 3 did not differ significantly between the treatment groups. There were also statistical differences in the SBP at T1, T2, T3, and T4 measurements. In this study, we found that TDS decreased more in the lidocaine group from T1 to T3, and the decrease in TDS was greater in the MgSO4 group at T4. There are similarities with research conducted by Fabricio in 2017 who observed a tendency for lower Systolic blood pressure in patients given Lidocaine than MgSO4 administration.9 Similar findings by Jefri in 2018 which showed that there was a greater decrease in the Lidocaine group than the MgSO4 group.10 This is different from the research conducted by Sachin in 2016 which reported that there was a significantly higher average TDS in the lidocaine group compared to the MgSO4 group at 1, 3, 5 minutes after intubation.11
According to Prajakta (2022), magnesium has an antagonistic effect on calcium because it has a similar biomolecular form. This calcium receptor circulates in the human body. Inhibition of calcium receptors in the presynapse causes inhibition of catecholamine neurotransmitter release from the presynapse. In blood vessels, magnesium causes vasodilation by relaxing the vascular smooth muscle, resulting in hypotensive anesthesia. In the heart, calcium receptors are also inhibited, resulting in an antiarrhythmic effect. Inhibition of calcium receptors triggers relaxation and inhibition of shivering. Magnesium also directly inhibits NMDA receptors in neuronal networks.12 In this study, the superiority of lidocaine over MgSO4 in MAP was considered to be the result of lidocaine's various mechanisms that can inhibit sympathetic responses, increase the threshold of stimulation in the tracheal tract, stop sympathetic transmission to the center, and reduce cardiovascular responses directly. In addition, the dose of MgSO4 used in this study was lower than previous studies.13
To prevent sympathetic reflex responses to laryngoscopy and intubation stimuli, it is important to consider the incidence of tachycardia that can occur because of laryngoscopy and intubation. Therefore, this study also assessed the heart rate. In this study, we found that the baseline HR of Group 1 (MgSO4), Group 2 (lidocaine), and Group 3 (NaCl 0.9%) were not significantly different between the treatment groups. In this study, there were also statistical differences in HR between the T1 and T2 measurements. In this study, the lidocaine group had a lower HR than the MgSO4 and Control groups. This may be due to the effect of lidocaine which has properties including as a class 1 anti-arrhythmic which can cause inhibition of action potentials in the heart, then lidocaine also has an antagonistic mechanism of action against sodium channels, NMDA receptors, reduces the release of substance P and has a glycinergic action resulting in decreased airway reactivity which results in a greater decrease in HR in the lidocaine group.14
Magnesium levels before and after intubation at the beginning of the study all patients had were within normal limits. In the group of patients administered MgSO4, there was a statistically insignificant increase with the administration of MgSO4 30 mg/kg. This is also in line with Nandal's research in 2021, which compared hemodynamics in patients who were intubated by administering MgSO4 in different doses and found that at a dose of 30 mg/kg, there was no statistically significant difference. The following statement indicates that giving MgSO4 30 mg / kg does not cause toxic magnesium levels in patients, so it is safe to give it to patients with initial magnesium levels that are within normal limits.15
Hemodynamic changes were greater in the lidocaine group than in the control and MgSO4 groups, where the decrease in blood pressure was greater in the lidocaine group; however, both lidocaine and MgSO4 could inhibit hemodynamic spikes during laryngoscopy and intubation. The cortisol value also decreased in both treatment groups compared to the control group, indicating a decreased effect on the stress response from laryngoscopy and intubation. This study differs from previous studies due to differences in the type and dose of induction drugs administered before intubation.
This study had some limitations. First, intubation was performed by different personnel, which may have resulted in measurement bias. In addition, this study had a small sample size, which could affect the results. Sampling in this study was carried out based on the action, namely craniotomy surgery, including supratentorial tumors, intracranial hemorrhage, and cerebral vascular malformations. In this study, the measurement of serum cortisol levels was only carried out at two time points, at the beginning and at 10 minutes, so that it could not fully describe cortisol levels.
Intravenous administration of lidocaine 1.5 mg/kg is most effective in attenuating the stress response in the form of increased blood pressure, heart rate and serum cortisol levels due to laryngoscopy and intubation in patients undergoing craniotomy compared to intravenous administration of MgSO4 30 mg/kg.
AR: Conception and design, administrative support.
Authors affiliations:
- Rr Sinta Irina, Neuro-anesthesiologist, Anesthesiology & Intensive Care Department, Universitas Sumatera Utara, Indonesia; Email: sinta.irina@usu.ac.id
- Arsil Radiansyah, Medical Doctor, Anesthesiology Resident, Department of Anesthesiology & Intensive Care, Universitas Sumatera Utara, Indonesia; Email: ey2840021@gmail.com
- Heru Kurniawan, Cardiovascular Anesthesiologist, Anesthesiology & Intensive Care Department, Universitas Sumatera Utara, Indonesia; Email: rirmiya639@gmail.com
ABSTRACT
Objective: Responses to stress following craniotomy can vary from elevated hemodynamics to elevated cortisol levels in the body. Intubation is a major factor that must be considered during the induction of neuroanesthesia. Magnesium sulfate has the advantage of maintaining the stability of brain autoregulation and is neuroprotective.
Methodology: The study was conducted after receiving ethical clearance from the Health Research Ethics Committee of the University of North Sumatra (No. 94/KEPK/USU/2024). The trial was registered at ClinicalTrials.gov under the identifier NCT06516861 on July 24, 2024. We included 30 patients, aged 18–65 years; body mass index (BMI) 18.5–29.9 kg/m², consecutively, undergoing craniotomy at our hospital. The patients were randomly divided into three equal groups; patients who received lidocaine, or MgSO4 and a control group, who received normal saline as a placebo. Post-induction and intubation, hemodynamic parameters, including systolic blood pressure, diastolic blood pressure, mean arterial pressure (MAP), and heart rate, were measured at 3, 5, 7, and 10 min (T1, T2, T3, and T4) following intubation. Serum cortisol levels were assessed at baseline (T0) and post-intubation.
Results: There were significant differences between the three groups with hemodynamic and serum cortisol levels found to be lower in the lidocaine group. (P = 0.001). Significant differences were observed among the three groups, with the lidocaine group showing lower hemodynamic parameters (systolic blood pressure, diastolic blood pressure, mean arterial pressure, heart rate) and serum cortisol levels (P = 0.001).
Conclusion: Intravenous administration of lidocaine 1.5 mg/kg is more effective in attenuating the stress response in the form of increased blood pressure, heart rate, and serum cortisol levels due to laryngoscopy and intubation in patients undergoing craniotomy than intravenous administration of MgSO4 30 mg/kg
Keywords: Craniotomy; Intubation; Lidocaine; MgSO4
Citation: Irina RS, Radiansyah A, Kurniawan H. Comparison of magnesium sulfate and lidocaine on hemodynamic response and cortisol levels after intubation in patients undergoing craniotomy. Anaesth. pain intensive care 2025;30(1):88-94. DOI: 10.35975/apic.v30i1.3107
Received: May 09, 2025; Revised: October 26, 2024; Accepted: January 01, 2025
1. INTRODUCTION
Craniotomy, a neurosurgical procedure involving the opening or removal of parts of the skull, is performed to address various intracranial conditions.1 In craniotomies, maintaining cerebral perfusion pressure (CPP), cerebral blood flow (CBF), and cerebral metabolic rate of oxygen (CMRO2) is critical during neuro-anesthesia induction to prevent secondary brain injury.2 Under general anesthesia, the primary goals are to optimize brain metabolism and ensure adequate brain oxygenation, often achieved through endotracheal intubation.3
Laryngoscopy and tracheal intubation are critical steps in general anesthesia induction but are associated with significant physiological stress in the patient. These procedures stimulate somatic and visceral nociceptive afferent fibers, triggering a sympathetic adrenal reflex response. This response increases neural activity in the cervical sympathetic efferent fibers, leading to heightened hemodynamic responses, including hypertension, tachycardia, and dysrhythmia.4 In craniotomy patients, these hemodynamic changes are particularly concerning as they can elevate intracranial pressure (ICP), exacerbate cerebral edema, and increase the risk of secondary brain injury due to compromised cerebral autoregulation.5
Sympathetic stimulation also elevates plasma catecholamine concentrations (e.g., adrenaline and noradrenaline), which may precipitate left ventricular failure, intracranial hemorrhage, or myocardial infarction in anesthetized patients.4 Additionally, intubation activates the hypothalamic-pituitary-adrenal (HPA) axis, stimulating the hypothalamus to release corticotropin-releasing hormone (CRH) and arginine vasopressin. These peptides trigger the secretion of adrenocorticotropic hormone (ACTH) from the anterior pituitary, which in turn stimulates cortisol release from the adrenal cortex.5,6 Elevated cortisol levels during craniotomy may exacerbate cerebral edema, increase intracranial pressure, and impair neurological recovery, necessitating interventions to mitigate this stress response. Cortisol, a primary biomarker of HPA axis activation, alongside the sympathetic adrenomedullary (SAM) system, drives the hemodynamic stress response (HDSR), increasing myocardial workload, coronary perfusion demand, and the risk of myocardial ischemia due to inadequate oxygenation.4,5
Various pharmacological agents, including opioids, calcium channel blockers, beta-blockers, alpha-2 agonists, magnesium sulfate, and local anesthetics, have been employed to mitigate the stress response during intubation.7 Intravenous lidocaine has been widely studied for its efficacy in attenuating the hemodynamic responses during laryngoscopy and intubation. While generally safe, its use requires precise dosing and careful monitoring by experienced healthcare professionals.7 Magnesium sulfate (MgSO4) acts as a physiological calcium antagonist, competing with calcium at membrane channels and modulating calcium-mediated responses. It inhibits catecholamine release from the adrenal gland and peripheral adrenergic nerve terminals, reducing stress responses.8 Additionally, MgSO4 offers neuroprotective benefits by inhibiting NMDA receptors, reducing glutamate excitotoxicity, and supporting cerebral vasodilation, which helps maintain cerebral autoregulation and protects the blood-brain barrier. In the cardiovascular system, MgSO4 promotes arteriolar vasodilation, enhances cardiac output, and may improve diastolic dysfunction with minimal impact on venous circulation.8
Previous studies, including a systematic review and meta-analysis by Cantey and Neu (2022), have demonstrated that both magnesium sulfate and lidocaine effectively attenuate post-intubation stress responses in the general population.9 However, evidence specific to patients with cerebrovascular disorders, such as those undergoing craniotomies, remains limited. Given the unique physiological challenges in this population, particularly the need to control ICP and prevent secondary brain injury, further investigations are warranted.
Therefore, this study aimed to compare the efficacy of magnesium sulfate and lidocaine in attenuating hemodynamic responses and post-intubation cortisol levels in patients undergoing craniotomy, providing insights into optimal anesthesia management for this high-risk group.
2. METHODOLOGY
This double-blind randomized controlled clinical trial with a pre- and post-test design, including a control group, aimed to compare hemodynamic responses and post-intubation cortisol levels following the administration of intravenous magnesium sulfate (MgSO₄) versus intravenous lidocaine. The study was conducted after receiving ethical clearance from the Health Research Ethics Committee of the University of North Sumatra (ethics number 94/KEPK/USU/2024). The trial was registered at ClinicalTrials.gov under the identifier NCT06516861 on July 24, 2024. The study population comprised all patients who underwent craniotomy at our institution.
Figure 1: Comparative systolic blood pressure
Figure 2: Comparative diastolic blood pressure
Figure 3: Comparative mean arterial pressure
Figure 4: Comparative heart rate graph
Figure 5: Comparative serum cortisol levels
The sample size was calculated using the formula for comparing two means, with an alpha of 0.05 and a power of 80%, resulting in a minimum requirement of 10 participants per group, for a total of 30 participants (10 each in the MgSO₄ group, 10 in the lidocaine group, and 10 in the control group). Subjects were selected using consecutive sampling until the required sample size was reached. Random allocation was performed using computer-based randomization via www.randomizer.org, ensuring an equal distribution across the three groups.
The study included patients who met the following inclusion criteria: aged 18–65 years; body mass index (BMI) 18.5–29.9 kg/m²; provided informed consent from the patient or their next of kin; and scheduled for elective non-traumatic craniotomy procedures, including supratentorial brain tumor evacuation, intracerebral hemorrhage evacuation, subdural hemorrhage evacuation, or cerebrovascular correction. The exclusion criteria were as follows: cardiac, hepatic, or renal disorders; pregnancy; pre-existing hypertension or hypotension before surgery; hypersensitivity to MgSO₄ or lidocaine; chronic use of corticosteroids, calcium channel blockers, magnesium-containing drugs, or opioids; high risk of difficult intubation or ventilation based on LEMON and MOANS score criteria; impaired cortisol secretion due to pituitary, hypothalamic, or adrenal gland disorders; and abnormal baseline cortisol levels (hypocortisolism or hypercortisolism) at T0 serum cortisol examination.
The participants were randomly assigned to one of three groups. Group 1 received MgSO₄ at a dose of 30 mg/kg, diluted in 20 mL of normal saline, administered over 5 min via a syringe pump and labeled as code A. Group 2 received lidocaine at a dose of 1.5 mg/kg, similarly diluted and administered, labeled as code B. The control group (code C) received 20 mL of normal saline as a placebo under identical conditions. The doses of MgSO4 and lidocaine were selected based on established clinical guidelines and prior studies demonstrating their safety and efficacy in attenuating hemodynamic responses during intubation.10,11 Specifically, the 30 mg/kg dose of MgSO₄ was chosen for its proven ability to reduce catecholamine release and maintain cerebral autoregulation in neurosurgical patients.10 The 1.5 mg/kg dose of lidocaine was selected based on its effectiveness in suppressing laryngoscopy-induced hemodynamic responses with minimal side effects.11
Post-induction and intubation, hemodynamic parameters, including systolic blood pressure, diastolic blood pressure, mean arterial pressure (MAP), and heart rate, were measured at 3, 5, 7, and 10 min (T1, T2, T3, and T4) following intubation. Serum cortisol levels were assessed at baseline (T0) and post-intubation. Patients who developed hypertension (systolic blood pressure >150 mmHg) at 5 min post-intubation were treated with titrated doses of nicardipine, starting at 0.25 mg/kg/h. Those with hypotension (systolic blood pressure < 80 mmHg) received 5–10 mg ephedrine. In cases of bradycardia (HR <50 beats/min), 0.5 mg atropine sulfate was administered.
2.1. Statistical Analysis
Data were analyzed using the SPSS version 25. Continuous variables, including hemodynamic parameters and cortisol levels, were compared across the three groups using one-way analysis of variance (ANOVA), followed by post-hoc Tukey tests for pairwise comparisons. Statistical significance was set at P < 0.05. The normality of the data distribution was assessed using the Shapiro-Wilk test, and non-parametric tests (e.g., Kruskal-Wallis test) were applied if the data were not normally distributed.
3. RESULTS
In this study, laryngoscopy and intubation were successfully performed on the first attempt in under one minute for all patients, with no intraoperative fatalities reported. The study included 30 participants, divided evenly into three groups: 10 patients in each group received either MgSO₄, lidocaine, or normal saline solution. The demographic characteristics of the groups were similar, with no significant differences in age, weight, height, or BMI (Table 1). Hemodynamic parameters showed significant differences among groups at various time points post-intubation. While MgSO4 demonstrated better control of mean arterial pressure (MAP) and heart rate (HR) at some early time points (e.g., 1-5 min, P < 0.05 vs lidocaine in select comparisons), overall attenuation of spikes and lower values in multiple parameters favored the lidocaine group (Figures 2-5). Serum cortisol levels decreased significantly in both treatment groups compared to control, with greater reduction in the lidocaine group. These findings indicate lidocaine's superior efficacy in blunting the overall intubation-induced stress response.
| Table 1: Comparative demographic characteristics of the participants | ||||
| Characteristics
|
Group 1
MgSO4 (n= 10) |
Group 2
Lidocaine (n = 10) |
Group 3
NaCl 0.9% (n = 10) |
P-value |
| Age | 0.200a | |||
| Mean ± SD | 41.70 ± 12.658 | 48.30 ± 12.685 | 50.20 ± 13.485 | |
| Median | 39.50 | 50.00 | 52.50 | |
| Min-Max | 26-65 | 27-65 | 26-65 | |
| Weight | 0.997a | |||
| Mean ± SD | 60.57 ± 10.173 | 61.80 ± 9.998 | 61.40 ± 11.616 | |
| Median | 57.50 | 62.00 | 58.50 | |
| Min-Max | 48-80 | 50-80 | 48-75 | |
| Height | 0.094a | |||
| Mean ± SD | 168.40 ± 1.350 | 166.60 ± 1.506 | 168.00 ± 2.000 | |
| Median | 169.00 | 166.50 | 169.00 | |
| Min-Max | 166-170 | 164-170 | 165-170 | |
| BMI | 0.935a | |||
| Mean ± SD | 21.6040 ± 3.93959 | 22.2230 ± 3.26460 | 21.7080 ± 3.80464 | |
| Median | 19.2600 | 22.3700 | 20.6350 | |
| Min-Max | 18.21-28.65 | 18.14-27.68 | 17.63-25.95 | |
| aKruskal wallis test; P < 0.05 considered as significant | ||||
The mean arterial pressure (MAP) and heart rate (HR) were significantly different between the two groups at various time points. Specifically, the Magnesium group demonstrated a significantly lower MAP than the lidocaine group at 1-minute post-intubation (P = 0.02). This trend continued with significant differences observed at 3 min (0.01) and 5 min post-intubation (P = 0.03), indicating better control of MAP in the Magnesium group.
Heart rate followed a similar pattern, with the magnesium group showing a significantly lower HR at 1 min (P = 0.04), 3 min (P = 0.01), and 5 min (P = 0.02) post-intubation compared to the lidocaine group. These results suggest that magnesium sulfate is more effective n blunting the hemodynamic response to intubation in terms of both MAP and HR.
| Table 2: Comparison of serum cortisol levels | ||||
| Measuring time | Group 1
MgSO4 (n = 10) |
Group 2
Lidocaine (n = 10) |
Group 3
NaCl 0.9% (n = 10) |
P-valuea |
| T0 | 340.80 ± 163.91 | 439.61 ± 171.74 | 274.70 ± 30.53 | 0.224 |
| T4 | 256.33 ± 78.62 | 350.43 ± 121.23 | 355.85 ± 104.57 | 0.084 |
| aKruskal wallis test; P < 0.05 considered as significant | ||||
4. DISCUSSION
This study compared the effectiveness of MgSO4 (Group 1), lidocaine (Group 2), and NaCl 0.9% (Group 3) in attenuating the stress response in patients undergoing craniotomy. In this study, there were 30 samples divided into three groups: 10 samples in group 1, 10 samples in group 2, and 10 samples in group 3. This study analyzed the characteristics of the samples obtained based on age, height, weight, and BMI. During the study sampling, there were no respondents who met the dropout criteria, that is, patients who underwent intubation more than once, with intubation time of more than one minute, or patients who died on the operating table. This study showed that each laryngoscopy was effectively performed once in less than one minute, and there were no cases of death on the operating table.
In this study, the baseline systolic blood pressures of Groups 1, 2, and 3 did not differ significantly between the treatment groups. There were also statistical differences in the SBP at T1, T2, T3, and T4 measurements. In this study, we found that TDS decreased more in the lidocaine group from T1 to T3, and the decrease in TDS was greater in the MgSO4 group at T4. There are similarities with research conducted by Fabricio in 2017 who observed a tendency for lower Systolic blood pressure in patients given Lidocaine than MgSO4 administration.9 Similar findings by Jefri in 2018 which showed that there was a greater decrease in the Lidocaine group than the MgSO4 group.10 This is different from the research conducted by Sachin in 2016 which reported that there was a significantly higher average TDS in the lidocaine group compared to the MgSO4 group at 1, 3, 5 minutes after intubation.11
According to Prajakta (2022), magnesium has an antagonistic effect on calcium because it has a similar biomolecular form. This calcium receptor circulates in the human body. Inhibition of calcium receptors in the presynapse causes inhibition of catecholamine neurotransmitter release from the presynapse. In blood vessels, magnesium causes vasodilation by relaxing the vascular smooth muscle, resulting in hypotensive anesthesia. In the heart, calcium receptors are also inhibited, resulting in an antiarrhythmic effect. Inhibition of calcium receptors triggers relaxation and inhibition of shivering. Magnesium also directly inhibits NMDA receptors in neuronal networks.12 In this study, the superiority of lidocaine over MgSO4 in MAP was considered to be the result of lidocaine's various mechanisms that can inhibit sympathetic responses, increase the threshold of stimulation in the tracheal tract, stop sympathetic transmission to the center, and reduce cardiovascular responses directly. In addition, the dose of MgSO4 used in this study was lower than previous studies.13
To prevent sympathetic reflex responses to laryngoscopy and intubation stimuli, it is important to consider the incidence of tachycardia that can occur because of laryngoscopy and intubation. Therefore, this study also assessed the heart rate. In this study, we found that the baseline HR of Group 1 (MgSO4), Group 2 (lidocaine), and Group 3 (NaCl 0.9%) were not significantly different between the treatment groups. In this study, there were also statistical differences in HR between the T1 and T2 measurements. In this study, the lidocaine group had a lower HR than the MgSO4 and Control groups. This may be due to the effect of lidocaine which has properties including as a class 1 anti-arrhythmic which can cause inhibition of action potentials in the heart, then lidocaine also has an antagonistic mechanism of action against sodium channels, NMDA receptors, reduces the release of substance P and has a glycinergic action resulting in decreased airway reactivity which results in a greater decrease in HR in the lidocaine group.14
Magnesium levels before and after intubation at the beginning of the study all patients had were within normal limits. In the group of patients administered MgSO4, there was a statistically insignificant increase with the administration of MgSO4 30 mg/kg. This is also in line with Nandal's research in 2021, which compared hemodynamics in patients who were intubated by administering MgSO4 in different doses and found that at a dose of 30 mg/kg, there was no statistically significant difference. The following statement indicates that giving MgSO4 30 mg / kg does not cause toxic magnesium levels in patients, so it is safe to give it to patients with initial magnesium levels that are within normal limits.15
Hemodynamic changes were greater in the lidocaine group than in the control and MgSO4 groups, where the decrease in blood pressure was greater in the lidocaine group; however, both lidocaine and MgSO4 could inhibit hemodynamic spikes during laryngoscopy and intubation. The cortisol value also decreased in both treatment groups compared to the control group, indicating a decreased effect on the stress response from laryngoscopy and intubation. This study differs from previous studies due to differences in the type and dose of induction drugs administered before intubation.
5. LIMITATIONS
This study had some limitations. First, intubation was performed by different personnel, which may have resulted in measurement bias. In addition, this study had a small sample size, which could affect the results. Sampling in this study was carried out based on the action, namely craniotomy surgery, including supratentorial tumors, intracranial hemorrhage, and cerebral vascular malformations. In this study, the measurement of serum cortisol levels was only carried out at two time points, at the beginning and at 10 minutes, so that it could not fully describe cortisol levels.
6. CONCLUSION
Intravenous administration of lidocaine 1.5 mg/kg is most effective in attenuating the stress response in the form of increased blood pressure, heart rate and serum cortisol levels due to laryngoscopy and intubation in patients undergoing craniotomy compared to intravenous administration of MgSO4 30 mg/kg.
- Data availability
- Conflict of interest
- Funding
- Acknowledgements
- Authors’ contribution
AR: Conception and design, administrative support.
12. REFERENCES
- Saleh SC, Rehatta NM. Neuroanestesia dan critical care. Surabaya: Airlangga University Press; 2023.
- Silverman A, Petersen NH. Physiology, cerebral autoregulation. In: StatPearls. Treasure Island (FL): StatPearls Publishing; 2024. Available from: https://www.ncbi.nlm.nih.gov/books/NBK553183/
- Bousselmi R, Lebbi MA, Bargaoui A, Ben Romdhane M, Messaoudi A, Ben Gabsia A, et al. Lidocaine reduces endotracheal tube associated side effects when instilled over the glottis but not when used to inflate the cuff: a double blind, placebo-controlled, randomized trial. Tunis Med. 2014 Jan;92(1):29-33. PubMed: https://pubmed.ncbi.nlm.nih.gov/24879167/
- Silpa AR, Koshy KA, Subramanian A, Pradeep KK. Comparison of the efficacy of two doses of dexmedetomidine in attenuating the hemodynamic response to intubation in patients undergoing elective cardiac surgery: a randomized double-blinded study. J Anaesthesiol Clin Pharmacol. 2020 Jan-Mar;36(1):83-7. PMCID: PMC7047691 DOI: 4103/joacp.JOACP_235_18
- Kumar S, Rastogi S, Yadav S, Agarwal A, Malviya D. Biochemical markers and haemodynamic changes of stress response after intubation with direct laryngoscopy versus video laryngoscopy versus fiberoptic intubation: a comparative study. Indian J Clin Anaesth. 2020;7(4):681-6. doi: 10.18231/j.ijca.2020.126.
- Prete A, Yan Q, Al-Tarrah K, Akturk HK, Prokop LJ, Alahdab F, et al. The cortisol stress response induced by surgery: a systematic review and meta-analysis. Clin Endocrinol (Oxf). 2018 Nov;89(5):554-67. DOI: 1111/cen.13820 .
- Gil-Gouveia R, Goadsby PJ. Neuropsychiatric side-effects of lidocaine: examples from the treatment of headache and a review. Cephalalgia. 2009 May;29(5):496-508. DOI: 1111/j.1468-2982.2008.01800.x
- Do SH. Magnesium: a versatile drug for anesthesiologists. Korean J Anesthesiol. 2013 Jul;65(1):4-8. PMCID: PMC3726845 DOI: 4097/kjae.2013.65.1.4
- Cantey A, Neu T. Comparison of magnesium sulfate versus lidocaine and their efficacy in preventing sympathetic nervous system response to direct laryngoscopy [dissertation]. San Antonio (TX): Our Lady of the Lake University; 2022.
- Pane JA, Hanafie A, Nasution AH. Perbedaan respon hemodinamik akibat tindakan laringoskopi dan intubasi pada pemberian intravena fentanyl dan magnesium sulfat dibandingkan dengan fentanyl dan lidokain. Bul Farmatera. 2018;3(3):147-62.
- Padmawar S, Patil M. A comparative study of 2% lignocaine vs 50% magnesium sulphate for attenuation of stress responses to laryngoscopy and endotracheal intubation. Int J Contemp Med Res. 2016;3(8):2317-21.
- Kasar PN, Karhade S. Comparison of intravenous magnesium sulphate and lignocaine in attenuation of pressor response to laryngoscopy and endotracheal intubation. IJMA. 2022;5(3):21-6.
- Kiaee MM, Safari S, Movaseghi GR, Dolatabadi MRM, Ghorbanlo M, Etemadi M, et al. The effect of intravenous magnesium sulfate and lidocaine in hemodynamic responses to endotracheal intubation in elective coronary artery bypass grafting: a randomized controlled clinical trial. Anesth Pain Med. 2014 Aug;4(3):e15905. PMCID: PMC4164986 DOI: 5812/aapm.15905
- Mendonça FT, de Queiroz LM da GM, Guimarães CCR, Xavier ACD. Effects of lidocaine and magnesium sulfate in attenuating hemodynamic response to tracheal intubation: single-center, prospective, double-blind, randomized study. Rev Bras Anestesiol. 2017 Jan-Feb;67(1):50-6. DOI: 1016/j.bjane.2015.08.004
- Nandal S, Chatrath V, Kaur H. Dose response study of magnesium sulphate for attenuation of haemodynamic response to intubation. J Evol Med Dent Sci. 2021;10(13):956-62. DOI:10.14260/jemds/2021/206