Bassem Z. T. Wassef 1 , Khaled A. A. ElSamahy 2 , Raafat M. Rayad 3 , Hossam Z. Ghobrial 4
Authors affiliations:
Background & objectives: Perineal pain secondary to pelvic malignancies remains a big challenge to the pain specialists and clinicians. Various management modalities have been used to manage it. This study assessed the feasibility and effectiveness of selective super voltage pulsed radiofrequency (SVPRF) as a potential alternative to selective thermal radiofrequency (TRF) saddle rhizotomy in patients experiencing refractory perineal pain secondary to pelvic malignancies
Methodology: This prospective, randomized, single-blind comparative study included 60 patients (≥18 years, both sexes) with advanced pelvic malignancies and moderate to severe perineal pain. Patients were equally divided into two groups: Group A: selective saddle rhizotomy via TRF ablation of the S3 nerve root on one side and bilateral S4 and S5 ablation, while Group B: selective SVPRF targeting the saddle nerves at unilateral S3 and bilateral S4 and S5.
Results: Visual analogue scale (VAS) demonstrated a significant decrease at 1, 4, and 12 weeks in group TRF relative to SVPRF group (P < 0.05). The Oswestry disability index was significantly lower at (1 week and 4 weeks) in group TRF relative to group SVPRF (P < 0.05). Functional improvement was significantly higher at 1 week and 4 weeks in group TRF than group SVPRF.
Conclusions: TRF saddle rhizotomy demonstrated superior efficacy over SVPRF in reducing pain, opioid and pregabalin use, and enhancing function in patients with refractory malignant perineal pain, without increasing complications or impacting patient satisfaction.
Abbreviations: RF: radiofrequency, SVPRF: super voltage pulsed radiofrequency, TRF: thermal radiofrequency ,
Keywords: Super Voltage Pulsed Radio Frequency, Thermal Radiofrequency, Saddle Rhizotomy, Saddle Nerves, Refractory Malignant Perineal Pain
Citation: Wassef BZT, ElSamahy KAA, Rayad RM, Ghobrial HZ. Super voltage pulsed radiofrequency versus thermal radiofrequency for ablation of saddle nerves for treating refractory malignant perineal pain: a single-blind prospective, randomized study. Anaesth. pain intensive care 2025;30(1):xxxxxxxx. DOI: 10.35975/apic.v30i1.xxxx
Received: May 09, 2025; Revised: October 26, 2024; Accepted: January 01, 2025
Pelvic pain in general is a common entity (16 -25) and the prevalence of pain in patients with advanced pelvic cancer may reach approximately 85.1 Management of such pain is challenging due to confined features of this region.2
Anatomically there is diversity of visceral and somatic innervations of pelvi-perineum (T10-S5) whether autonomic nerves (superior hypogastric plexus, inferior hypogastric plexus and ganglion impar) or somatic nerves as pudendal nerve (S2, S3, S4), Nerve to levator ani (S3, S4, S5) and coccygeal plexus. Anatomically, also there is a role of interconvergence of somatic and visceral afferents in perpetuating and extending pelvi-perineal pain experience
(viscero- visceral, viscero- somatic and somato-somatic convergence).3
Besides that, the perineum receives bilateral innervations and hence necessitates bilateral intervention procedures. Of special concern at this point that pelvi-perineal innervation is important for sphincteric function and it is believed that preserving both S2 and S3 function, at least on one side is crucial for sphincteric control. Physiologically, pain generators in this region involve multiple systems such as gastrointestinal, genito-urinary, reproductive, neurological musculoskeletal systems. All of that aggravating this horrible pain experience.4
Pain management of this pain must be multidisciplinary passing through
behavioral, pharmacological and interventional treatments. Pharmacological treatment according to WHO stepladder includes nonopioids, weak opioids and strong opioids plus adjuvants as antidepressants, anticonvulsants and
corticosteroids.5 Interventional treatment includes chemical rhizotomy, thermal RF ablation [6], percutaneous cervical cordotomy, spinal cord stimulation, sacral root stimulation and intrathecal pampus. The last three options have technical and financial consideration, decreasing their use in developing countries.
The use of percutaneous cervical cordotomy is limited in treating pelviperineal pain because it can't be bilateral, so it is not effective in midline perineal pain. Rhizotomy is surgical, chemical or ablative (RF or cryoanalgesia) selective segmental destruction of the dorsal sensory root.
Preservation of sphincter function is a primary concern in patients with pelvic or rectal malignancies. Bladder dysfunction following chemical rhizotomy has been reported with an incidence ranging from 1.25 to 24.7 Selective sacral nerve root rhizotomy is safer in this issue.6 It is generally accepted that preserving sphincter control requires maintaining the integrity of the S2 and S3 nerve roots on at least one side.1
Selective rhizotomy employing radiofrequency (RF) or cryoanalgesia is favored over conventional chemical neurolysis due to its presumed advantages of enhanced safety, greater selectivity, and more precise lesion control.6
Pulsed RF is a neuro-modulating technique in pain therapy which has an over advantage in preserving the neurological function if compared to thermal RF ablation.8
The objective of this study was to assess the feasibility and effectiveness of selective super voltage pulsed RF as an alternative to selective thermal RF Saddle rhizotomy for the management of refractory perineal pain in patients with pelvic malignancies
This prospective, randomized, single-blind comparative study included 60 patients of both sexes, aged ≥18 years or older, classified as American Society of Anesthesiologists (ASA) physical status II–III, with a body mass index (BMI) ranging from 20 to 30 kg/m². All patients had advanced pelvic malignancies and reported moderate to severe perineal pain, defined as a visual analogue scale (VAS) score exceeding 40 out of 100, which was unresponsive to maximum tolerated doses of morphine sulfate for at least four weeks in addition to adjuvant therapy with pregabalin. The study received ethical approval from the National Cancer Institute’s Ethical Committee in Cairo, Egypt (Institutional Review Board Approval No. 201920017.3), and written informed consent was obtained from all participants or their legal guardians.
Exclusion criteria were patients having contraindications to pain interventions include coagulopathy, local or systemic infection, increased intracranial pressure, advanced malignancy causing anatomical distortion that renders the procedure technically challenging or unsafe, history of allergy to local anesthetic or dexamethasone, decompensated cardiac, respiratory, renal or endocrinal diseases and any patient who couldn’t complete follow up for 3 months post-Randomization was performed using an online tool (http://www.randomizer.org) to generate a random allocation sequence, with each patient’s assignment concealed in an opaque sealed envelope. Participants were randomly assigned in a 1:1 ratio into two parallel groups: Group A underwent selective saddle rhizotomy via TRF ablation of the S3 nerve root on one side and bilateral S4 and S5 ablation TRF group, while Group B received selective super voltage pulsed radiofrequency (SVPRF) ablation targeting the saddle nerves at unilateral S3 and bilateral S4 and S5 (SVPRF group). Outcome assessments were conducted by a blinded clinician who was not involved in the study’s execution.
A 1 g dose of cefazolin was administered intravenously 30 minutes before the procedure. Procedures were performed in the intervention room with continuous monitoring of electrocardiography, pulse oximetry, and non-invasive arterial blood pressure. Supplemental oxygen was provided through nasal prongs at 3 L/min. Conscious sedation was achieved using intravenous dexmedetomidine boluses (0.5–1.0 µg/kg) in combination with intravenous fentanyl boluses at 1.0 µg/kg (Figure 1).
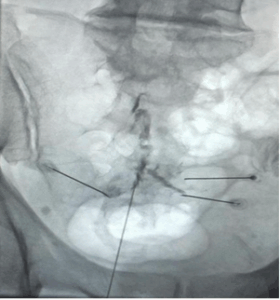
Figure 1: Anteroposterior projection of the sacrum post-injection of radio-opaque dye, illustrating the positioning of four radiofrequency needles. Upper needle: is on right S3 root, Lower needle: is targeting bilateral S5 roots, In between 2 needles: are on right & Lift S4 roots
2.1. TRF Rhizotomy Technique
The patient was positioned prone on a radiolucent table. Using fluoroscopic guidance, the L5-S1 interspace was aligned, and the C-arm was tilted 5–10 degrees ipsilaterally to visualize the sacral foramina. The S3 foramen was identified unilaterally on the side of predominant pain, while bilateral visualization of the S4 foramina was achieved. The S5 nerve root was located on a lateral sacral view by palpation of the sacral hiatus.
A curved, sharp-tipped 20-gauge radiofrequency needle with a 100 mm shaft and 10 mm active tip was inserted for thermal ablation of the targeted nerve roots. At each sacral root, 0.2 mL of iohexol contrast was injected, followed by anteroposterior and lateral fluoroscopic imaging to confirm adequate distribution of the contrast along the nerve root. Sensory stimulation (50 Hz, 0.5–0.7 V) and motor stimulation (2 Hz, 1–1.5 V) were used to verify proper needle placement. Subsequently, 0.75 mL of 2 lidocaine combined with 1 mg dexamethasone (total volume 1 mL) was administered prior to lesioning. Thermal radiofrequency was applied at 80°C for 180 seconds.
Following the procedure, patients were observed in the recovery room for 1–2 hours, with monitoring of vital signs, pain levels, and neurological status prior to discharge.
2.2. SVPRF Technique
The patient was positioned prone on a radiolucent table. Under fluoroscopic guidance, the L5-S1 interspace was aligned, and the C-arm was tilted 5–10 degrees ipsilaterally to visualize the sacral foramina. The S3 foramen was identified unilaterally on the side corresponding to the dominant pain, while the S4 foramina were visualized bilaterally. The S5 nerve root was located on a true lateral sacral view by palpation of the bony sacral hiatus.
A curved, sharp-tipped 20-gauge radiofrequency (RF) needle with a 100 mm shaft and 10 mm active tip was introduced for pulsed RF treatment of the targeted roots. At each sacral root, 0.2 mL of iohexol contrast medium was injected, followed by anteroposterior and lateral fluoroscopic imaging to confirm adequate spread of the radiopaque dye along the targeted nerve root. Sensory stimulation (50 Hz, 0.5–0.7 V) and motor stimulation (2 Hz, 1–1.5 V) were performed to verify accurate needle positioning. Subsequently, 0.75 mL of 2 lidocaine combined with 1 mg dexamethasone (total volume 1 mL) was administered prior to delivering the super voltage pulsed RF. The pulsed RF was applied at a needle tip temperature of 45°C, frequency of 5 Hz, pulse duration of 5 milliseconds, and super voltage of 50 volts for 5 minutes.
The primary outcome was determining the feasibility and effectiveness of using selective super voltage pulsed RF as an alternative to selective Thermal RF saddle rhizotomy among participants suffering from persistent perineal pain related to pelvic malignancies. The secondary outcome was to assess the degree of safety of using selective super voltage pulsed RF as an alternative to selective thermal RF saddle rhizotomy in patients with refractory perineal pain associated with pelvic malignancies.
Following the procedure, the patient was monitored in the recovery room for 1–2 hours, during which vital signs, pain levels, and neurological status were assessed prior to discharge.
2.3. Statistical analysis
Data analyses were performed using SPSS version 27 (IBM©, Armonk, NY, USA). The normality of data distribution was assessed using the Shapiro-Wilk test and visual inspection of histograms. Parametric quantitative data were expressed as mean ± standard deviation and compared using the unpaired Student’s t-test. Non-parametric quantitative data were presented as median with interquartile range (IQR) and analyzed via the Mann–Whitney U test. Categorical variables were summarized as frequencies and percentages, with comparisons conducted using the Chi-square test or Fisher’s exact test as appropriate. A two-tailed P < 0.05 was considered indicative of statistical significance.
Eighty-three patients were evaluated for eligibility, with 17 excluded due to not meeting inclusion criteria and 6 declining to participate. The remaining 60 patients were randomly allocated equally into two groups of 30 each. All participants were followed up and included in the statistical analysis Figure 2
There were no meaningful differences between the two groups regarding age, sex, weight, height, BMI, ASA physical status, and baseline VAS scores. However, VAS scores were markedly reduced in the TRF group compared to the SVPRF group at 1 week, 4 weeks, and 12 weeks post-intervention (P < 0.05) (Table 1).
Morphine sulphate consumption was significantly lower at (1 week, 4 weeks and 12 weeks) in group TRF relative to group PRF (P<0.05) and did not differ significantly at baseline between both groups (Table 2).
The Oswestry disability index was significantly lower at (1 week and 4 weeks) in group TRF relative to group SVPRF (P < 0.05) . Functional improvement was markedly elevated in 1 week and 4 weeks in group TRF relative to group SVPRF (P<0.05) and was insignificant 12 weeks different among both groups (Table 3).
Patients’ satisfaction, pain, hematoma, hypotension and numbness showed no significant differences among the groups (Table 4).
In cases of advanced pelvic cancer, pain prevalence can be as high as 85. Effective management of pain related to pelvic malignancies is frequently challenging due to the complex neuroanatomical structures and unique functional characteristics of the pelvic region.9
Our study revealed that VAS was significantly lower at (1 week, 4 weeks and 12 weeks) in group TRF relative to group SVPRF (P < 0.05) and showed no significant baseline differences among the groups.
This study is consistent with Usmani H et al. (2018), who reported significant pain relief at the time of discharge, with similar outcomes observed at 24 hours post-procedure.10 However, at the first, third, and sixth weeks of follow-up, patients in the CRF group demonstrated significantly greater pain relief compared to those in the PRF group.
Similarly, in the study by Reyad RM et al, who utilized mixed linear modeling to assess changes in pain scores. They reported that the estimated marginal mean ± SE
pain score for the RF group was 41.8 ± 1.04, providing further evidence of the impact of RF treatment on pain relief.6
In our results, Morphine sulphate consumption and Pregabalin consumption were significantly lower at (1 week, 4 weeks and 12 weeks) in group TRF compared to group SVPRF (P value<0.05) and showed no significant baseline differences among the groups. This notable reduction in both morphine and pregabalin consumption in the TRF group compared to SVPRF suggests that TRF may exert a more prolonged neuro-modulatory effect, potentially leading to a decreased reliance on opioid and neuropathic pain medications.
This aligns with the hypothesis that thermal RF achieves more sustained neural ablation, thereby reducing dependence on opioid and neuropathic pain medications. Supporting this notion Reyad RM et al. indicate that despite the application of RF, patients required an average morphine consumption of 49.0 ± 2.7 mg/day and pregabalin consumption of 145.9 ± 7.0 mg/day. This suggests that while RF provides pain relief, it may not completely eliminate the need for adjunctive analgesia.6
Similarly, Li Q et al. (2024) demonstrated that while RF therapy effectively alleviated perineal pain, oral morphine and pregabalin remained necessary for managing pain in other regions affected by cancer.11 Notably, no meaningful differences (P > 0.05) were observed in terms of daily morphine equivalent dose and pregabalin intake between the two groups before and six months post-treatment. These findings collectively suggest that while RF—particularly TRF—can significantly reduce analgesic requirements, a complete discontinuation of pain medications may not always be feasible, emphasizing the need for a multimodal pain management approach.
In our findings, the ODI was significantly lower at 1 week and 4 weeks in the TRF group versus the SVPRF group (P = 0.043 and 0.023, respectively), indicating reduced disability. Similarly, Functional improvement was significantly greater at the same time points in the TRF group versus the SVPRF group (P = 0.038 and 0.026, respectively), while no meaningful difference was observed among the groups at 12 weeks (P = 0.069).
In comparison, Reyad RM et al. (2018) documented a gradual decrease in disability levels over time in the RF group, with an increasing proportion of patients experiencing mild to moderate disability rather than severe impairment.6 However, the complete resolution of disability (no disability) was not achieved by week 12. Their findings also demonstrated that, despite some fluctuations, a substantial proportion of patients in the RF group attained at least moderate functional improvement by week 12.
Our study found that Patients satisfaction was showed no significant difference among both groups. Consistent with our findings, Reyad RM et al. (2018) found that in the RF group, patient satisfaction levels varied, with the majority reporting positive outcomes.6 A total of 60 of participants scored their improvement as either very much improved (30) or markedly improved (30). Additionally, 25 of patients reported minimal improvement, while 15 experienced no change in their condition. Notably, no patients in the RF group reported worsening symptoms. These findings suggest that RF treatment was generally well-received, with a substantial proportion of patients experiencing meaningful clinical improvement. The absence of negative outcomes further supports its role as a viable intervention for pain management.
However, our findings contrast consistent with those documented by Usmani H et al. (2018), observed that a significantly greater proportion of patients in the CRF group rated their satisfaction as excellent or good compared to those in the PRF group at the first, third, and sixth weeks of follow-up.10 Furthermore, overall patient satisfaction at the conclusion of the follow-up period was significantly higher in the CRF group than in the PRF group (P = 0.000). This discrepancy may be attributed to variations in patient selection criteria, procedural techniques, or post-procedural analgesic regimens between the studies. Additionally, the neuro-ablative effect of CRF, which results in more prolonged pain relief compared to PRF, could have contributed to the higher patient satisfaction observed in their study.
Our results showed that pain, hematoma, hypotension and numbness showed no significant differences among groups.
These findings are concordant with those reported by Usmani H et al. (2018) reported that participants were discharged from the hospital following four hours of observation without experiencing any adverse effects. No major neurological complications or untoward adverse effects were observed in either group throughout the follow-up period, except for minor infections at the skin puncture site. Infection occurred in three out of 34 patients in the CRF group and two out of 31 patients in the PRF group, with all affected patients responding well to oral antibiotics. The rate of this complication was similar between both groups, reinforcing the overall safety profile of both techniques. This alignment between our study and previous research supports the notion that both thermal and pulsed RF ablation are generally well-tolerated interventions with minimal procedural risks.
Moreover, our study is consistent with Reyad RM et al. (2018), who revealed that in the RF group, minor adverse events were observed in a small proportion of patients.6 Back pain was the most frequently reported minor complication, affecting 20 of patients. However, no cases of post-dural puncture headache, aseptic meningitis, or hypotension were reported in this group. Regarding major adverse events, no patients in the RF group encountered dysesthesia of the lower limbs, lower limb paresis, bladder dysfunction, or fecal incontinence. Consequently, the per-patient incidence of major adverse events in this group was 0. This suggests a favorable safety profile for RF treatment, with minimal risk of serious complications.
The limitations of the study included that study was performed at a single institution, which could constrain the applicability of the results to broader populations. Short-term follow-up: While significant differences were observed at 1-week and 4-week intervals, prolonged follow-up is essential to assess sustained pain relief and functional improvement, small sample size: The study included only 60 patients, which may not be fully representative of the larger patient population with malignant perineal pain, single-blind design: While patients were blinded to the intervention, clinicians were not, which may introduce potential bias in assessments, heterogeneous patient conditions: Variations in tumor type, stage, and prior pain management strategies might have influenced individual responses to treatment.
TRF was superior to SVPRF in terms of pain reduction (VAS scores), reduced opioid (morphine sulfate) and pregabalin consumption, and improved functional outcomes (Oswestry Disability Index and functional improvement scores) over short- and mid-term follow-ups (1 week, 4 weeks, and 12 weeks). However, no meaningful differences were observed among the two groups regarding patient satisfaction and the incidence of complications. These findings suggest that TRF may be superior in efficacy intervention for managing refractory malignant perineal pain compared to SVPRF while maintaining a similar safety profile.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
BZTW: Study concept and design.
KAAE: Analysis and interpretation of data.
RMR: Critical revision of the manuscript for important intellectual content.
HZG: Administrative, technical, and material support.
Authors affiliations:
- Bassem Z. T. Wassef, Assistant Lecturer of Anesthesiology, Surgical Intensive Care & Pain Management, Faculty of Medicine, Ain Shams University, Cairo, Egypt; Email: bassem_zaher@yahoo.com
- Khaled A. A. EL Samahy, Professor of Anesthesiology, Surgical Intensive Care & Pain Management, National Cancer Institute, Cairo, Egypt; Email: khaled_smahy@yahoo.com
- Raafat M. Reyad, Professor of Anesthesiology, Surgical Intensive Care & Pain Management, National Cancer Institute, Cairo, Egypt; Email: dr_raafat2006@hotmail.com
- Hossam Z. Ghobrial, Professor of Anesthesiology, Surgical Intensive Care & Pain Management, National Cancer Institute, Cairo, Egypt; Email: hossam_zarif@yahoo.com
ABSTRACT
Background & objectives: Perineal pain secondary to pelvic malignancies remains a big challenge to the pain specialists and clinicians. Various management modalities have been used to manage it. This study assessed the feasibility and effectiveness of selective super voltage pulsed radiofrequency (SVPRF) as a potential alternative to selective thermal radiofrequency (TRF) saddle rhizotomy in patients experiencing refractory perineal pain secondary to pelvic malignancies
Methodology: This prospective, randomized, single-blind comparative study included 60 patients (≥18 years, both sexes) with advanced pelvic malignancies and moderate to severe perineal pain. Patients were equally divided into two groups: Group A: selective saddle rhizotomy via TRF ablation of the S3 nerve root on one side and bilateral S4 and S5 ablation, while Group B: selective SVPRF targeting the saddle nerves at unilateral S3 and bilateral S4 and S5.
Results: Visual analogue scale (VAS) demonstrated a significant decrease at 1, 4, and 12 weeks in group TRF relative to SVPRF group (P < 0.05). The Oswestry disability index was significantly lower at (1 week and 4 weeks) in group TRF relative to group SVPRF (P < 0.05). Functional improvement was significantly higher at 1 week and 4 weeks in group TRF than group SVPRF.
Conclusions: TRF saddle rhizotomy demonstrated superior efficacy over SVPRF in reducing pain, opioid and pregabalin use, and enhancing function in patients with refractory malignant perineal pain, without increasing complications or impacting patient satisfaction.
Abbreviations: RF: radiofrequency, SVPRF: super voltage pulsed radiofrequency, TRF: thermal radiofrequency ,
Keywords: Super Voltage Pulsed Radio Frequency, Thermal Radiofrequency, Saddle Rhizotomy, Saddle Nerves, Refractory Malignant Perineal Pain
Citation: Wassef BZT, ElSamahy KAA, Rayad RM, Ghobrial HZ. Super voltage pulsed radiofrequency versus thermal radiofrequency for ablation of saddle nerves for treating refractory malignant perineal pain: a single-blind prospective, randomized study. Anaesth. pain intensive care 2025;30(1):xxxxxxxx. DOI: 10.35975/apic.v30i1.xxxx
Received: May 09, 2025; Revised: October 26, 2024; Accepted: January 01, 2025
1. INTRODUCTION
Pelvic pain in general is a common entity (16 -25) and the prevalence of pain in patients with advanced pelvic cancer may reach approximately 85.1 Management of such pain is challenging due to confined features of this region.2
Anatomically there is diversity of visceral and somatic innervations of pelvi-perineum (T10-S5) whether autonomic nerves (superior hypogastric plexus, inferior hypogastric plexus and ganglion impar) or somatic nerves as pudendal nerve (S2, S3, S4), Nerve to levator ani (S3, S4, S5) and coccygeal plexus. Anatomically, also there is a role of interconvergence of somatic and visceral afferents in perpetuating and extending pelvi-perineal pain experience
(viscero- visceral, viscero- somatic and somato-somatic convergence).3
Besides that, the perineum receives bilateral innervations and hence necessitates bilateral intervention procedures. Of special concern at this point that pelvi-perineal innervation is important for sphincteric function and it is believed that preserving both S2 and S3 function, at least on one side is crucial for sphincteric control. Physiologically, pain generators in this region involve multiple systems such as gastrointestinal, genito-urinary, reproductive, neurological musculoskeletal systems. All of that aggravating this horrible pain experience.4
Pain management of this pain must be multidisciplinary passing through
behavioral, pharmacological and interventional treatments. Pharmacological treatment according to WHO stepladder includes nonopioids, weak opioids and strong opioids plus adjuvants as antidepressants, anticonvulsants and
corticosteroids.5 Interventional treatment includes chemical rhizotomy, thermal RF ablation [6], percutaneous cervical cordotomy, spinal cord stimulation, sacral root stimulation and intrathecal pampus. The last three options have technical and financial consideration, decreasing their use in developing countries.
The use of percutaneous cervical cordotomy is limited in treating pelviperineal pain because it can't be bilateral, so it is not effective in midline perineal pain. Rhizotomy is surgical, chemical or ablative (RF or cryoanalgesia) selective segmental destruction of the dorsal sensory root.
Preservation of sphincter function is a primary concern in patients with pelvic or rectal malignancies. Bladder dysfunction following chemical rhizotomy has been reported with an incidence ranging from 1.25 to 24.7 Selective sacral nerve root rhizotomy is safer in this issue.6 It is generally accepted that preserving sphincter control requires maintaining the integrity of the S2 and S3 nerve roots on at least one side.1
Selective rhizotomy employing radiofrequency (RF) or cryoanalgesia is favored over conventional chemical neurolysis due to its presumed advantages of enhanced safety, greater selectivity, and more precise lesion control.6
Pulsed RF is a neuro-modulating technique in pain therapy which has an over advantage in preserving the neurological function if compared to thermal RF ablation.8
The objective of this study was to assess the feasibility and effectiveness of selective super voltage pulsed RF as an alternative to selective thermal RF Saddle rhizotomy for the management of refractory perineal pain in patients with pelvic malignancies
2. METHODOLOGY
This prospective, randomized, single-blind comparative study included 60 patients of both sexes, aged ≥18 years or older, classified as American Society of Anesthesiologists (ASA) physical status II–III, with a body mass index (BMI) ranging from 20 to 30 kg/m². All patients had advanced pelvic malignancies and reported moderate to severe perineal pain, defined as a visual analogue scale (VAS) score exceeding 40 out of 100, which was unresponsive to maximum tolerated doses of morphine sulfate for at least four weeks in addition to adjuvant therapy with pregabalin. The study received ethical approval from the National Cancer Institute’s Ethical Committee in Cairo, Egypt (Institutional Review Board Approval No. 201920017.3), and written informed consent was obtained from all participants or their legal guardians.
Exclusion criteria were patients having contraindications to pain interventions include coagulopathy, local or systemic infection, increased intracranial pressure, advanced malignancy causing anatomical distortion that renders the procedure technically challenging or unsafe, history of allergy to local anesthetic or dexamethasone, decompensated cardiac, respiratory, renal or endocrinal diseases and any patient who couldn’t complete follow up for 3 months post-Randomization was performed using an online tool (http://www.randomizer.org) to generate a random allocation sequence, with each patient’s assignment concealed in an opaque sealed envelope. Participants were randomly assigned in a 1:1 ratio into two parallel groups: Group A underwent selective saddle rhizotomy via TRF ablation of the S3 nerve root on one side and bilateral S4 and S5 ablation TRF group, while Group B received selective super voltage pulsed radiofrequency (SVPRF) ablation targeting the saddle nerves at unilateral S3 and bilateral S4 and S5 (SVPRF group). Outcome assessments were conducted by a blinded clinician who was not involved in the study’s execution.
A 1 g dose of cefazolin was administered intravenously 30 minutes before the procedure. Procedures were performed in the intervention room with continuous monitoring of electrocardiography, pulse oximetry, and non-invasive arterial blood pressure. Supplemental oxygen was provided through nasal prongs at 3 L/min. Conscious sedation was achieved using intravenous dexmedetomidine boluses (0.5–1.0 µg/kg) in combination with intravenous fentanyl boluses at 1.0 µg/kg (Figure 1).
Figure 1: Anteroposterior projection of the sacrum post-injection of radio-opaque dye, illustrating the positioning of four radiofrequency needles. Upper needle: is on right S3 root, Lower needle: is targeting bilateral S5 roots, In between 2 needles: are on right & Lift S4 roots
2.1. TRF Rhizotomy Technique
The patient was positioned prone on a radiolucent table. Using fluoroscopic guidance, the L5-S1 interspace was aligned, and the C-arm was tilted 5–10 degrees ipsilaterally to visualize the sacral foramina. The S3 foramen was identified unilaterally on the side of predominant pain, while bilateral visualization of the S4 foramina was achieved. The S5 nerve root was located on a lateral sacral view by palpation of the sacral hiatus.
A curved, sharp-tipped 20-gauge radiofrequency needle with a 100 mm shaft and 10 mm active tip was inserted for thermal ablation of the targeted nerve roots. At each sacral root, 0.2 mL of iohexol contrast was injected, followed by anteroposterior and lateral fluoroscopic imaging to confirm adequate distribution of the contrast along the nerve root. Sensory stimulation (50 Hz, 0.5–0.7 V) and motor stimulation (2 Hz, 1–1.5 V) were used to verify proper needle placement. Subsequently, 0.75 mL of 2 lidocaine combined with 1 mg dexamethasone (total volume 1 mL) was administered prior to lesioning. Thermal radiofrequency was applied at 80°C for 180 seconds.
Following the procedure, patients were observed in the recovery room for 1–2 hours, with monitoring of vital signs, pain levels, and neurological status prior to discharge.
2.2. SVPRF Technique
The patient was positioned prone on a radiolucent table. Under fluoroscopic guidance, the L5-S1 interspace was aligned, and the C-arm was tilted 5–10 degrees ipsilaterally to visualize the sacral foramina. The S3 foramen was identified unilaterally on the side corresponding to the dominant pain, while the S4 foramina were visualized bilaterally. The S5 nerve root was located on a true lateral sacral view by palpation of the bony sacral hiatus.
A curved, sharp-tipped 20-gauge radiofrequency (RF) needle with a 100 mm shaft and 10 mm active tip was introduced for pulsed RF treatment of the targeted roots. At each sacral root, 0.2 mL of iohexol contrast medium was injected, followed by anteroposterior and lateral fluoroscopic imaging to confirm adequate spread of the radiopaque dye along the targeted nerve root. Sensory stimulation (50 Hz, 0.5–0.7 V) and motor stimulation (2 Hz, 1–1.5 V) were performed to verify accurate needle positioning. Subsequently, 0.75 mL of 2 lidocaine combined with 1 mg dexamethasone (total volume 1 mL) was administered prior to delivering the super voltage pulsed RF. The pulsed RF was applied at a needle tip temperature of 45°C, frequency of 5 Hz, pulse duration of 5 milliseconds, and super voltage of 50 volts for 5 minutes.
The primary outcome was determining the feasibility and effectiveness of using selective super voltage pulsed RF as an alternative to selective Thermal RF saddle rhizotomy among participants suffering from persistent perineal pain related to pelvic malignancies. The secondary outcome was to assess the degree of safety of using selective super voltage pulsed RF as an alternative to selective thermal RF saddle rhizotomy in patients with refractory perineal pain associated with pelvic malignancies.
Following the procedure, the patient was monitored in the recovery room for 1–2 hours, during which vital signs, pain levels, and neurological status were assessed prior to discharge.
2.3. Statistical analysis
Data analyses were performed using SPSS version 27 (IBM©, Armonk, NY, USA). The normality of data distribution was assessed using the Shapiro-Wilk test and visual inspection of histograms. Parametric quantitative data were expressed as mean ± standard deviation and compared using the unpaired Student’s t-test. Non-parametric quantitative data were presented as median with interquartile range (IQR) and analyzed via the Mann–Whitney U test. Categorical variables were summarized as frequencies and percentages, with comparisons conducted using the Chi-square test or Fisher’s exact test as appropriate. A two-tailed P < 0.05 was considered indicative of statistical significance.
3. RESULTS
Eighty-three patients were evaluated for eligibility, with 17 excluded due to not meeting inclusion criteria and 6 declining to participate. The remaining 60 patients were randomly allocated equally into two groups of 30 each. All participants were followed up and included in the statistical analysis Figure 2
There were no meaningful differences between the two groups regarding age, sex, weight, height, BMI, ASA physical status, and baseline VAS scores. However, VAS scores were markedly reduced in the TRF group compared to the SVPRF group at 1 week, 4 weeks, and 12 weeks post-intervention (P < 0.05) (Table 1).
| Table 1: Demographic profile of the enrolled groups | ||||
| Parameters | Group TRF
(n = 30) |
Group SVPRF
(n = 30) |
P-value | |
| Age (years) | 45.6 ± 13.6 | 48.1 ± 15.64 | 0.511 | |
| Gender | Male | 17 (56.67)) | 14 (46.67) | 0.438 |
| Female | 13 (43.33) | 16 (53.33) | ||
| Weight (kg) | 77.63 ± 9.49 | 76.47 ± 11.77 | 0.674 | |
| Height (cm) | 171.13 ± 5.51 | 172.2 ± 6.14 | 0.482 | |
| BMI (kg/m²) | 26.49 ± 2.84 | 25.7 ± 3.1 | 0.306 | |
| ASA physical status | I | 18 (60.0) | 14 (46.67) | 0.581 |
| II | 8 (26.67) | 11 (36.67) | ||
| III | 4 (13.33) | 5 (16.67) | ||
| VAS | Baseline | 70 (62.5 - 80) | 80 (60 - 80) | 0.659 |
| 1 week | 30 (20 - 40) | 50 (40 - 60) | <0.001* | |
| 4 weeks | 20 (10 - 30) | 40 (30 - 40) | <0.001* | |
| 12 weeks | 20 (10 - 20) | 20 (10 - 30) | 0.044* | |
| Data are shown as mean ± SD or frequency (%). TRF: Thermo coagulation Radiofrequency, SVPRF: super voltage pulsed radio frequency, BMI: Body mass index. ASA: American Society of Anesthesiologists, VAS: Visual Analogue Scale. | ||||
Morphine sulphate consumption was significantly lower at (1 week, 4 weeks and 12 weeks) in group TRF relative to group PRF (P<0.05) and did not differ significantly at baseline between both groups (Table 2).
| Table 2: Morphine sulphate and pregabalin consumption of the studied groups | |||
| Record Time | Group TRF
(n = 30) |
Group SVPRF
(n = 30) |
P-value |
| Morphine sulphate consumption (mg/day) | |||
| Baseline | 91 ± 17.29 | 92.33 ± 17.55 | 0.768 |
| 1 week | 65 ± 19.07 | 78.67 ± 18.52 | 0.007* |
| 4 weeks | 57.33 ± 16.6 | 66.67 ± 17.49 | 0.038* |
| 12 weeks | 41.33 ± 13.58 | 54.33 ± 20.46 | 0.005* |
| Pregabalin consumption (mg/day) | |||
| 1 week | 126.33 ± 14.97 | 137.67 ± 16.54 | 0.007* |
| 4 weeks | 109.67 ± 13.26 | 128.33 ± 16.83 | <0.001* |
| 12 weeks | 77 ± 9.15 | 108 ± 20.41 | <0.001* |
| 1 week | 126.33 ± 14.97 | 137.67 ± 16.54 | 0.007* |
| Data are presented as mean ± SD; *:Significant when P ≤ 0.05; TRF: Thermo coagulation Radiofrequency, SVPRF: super voltage pulsed radio frequency | |||
The Oswestry disability index was significantly lower at (1 week and 4 weeks) in group TRF relative to group SVPRF (P < 0.05) . Functional improvement was markedly elevated in 1 week and 4 weeks in group TRF relative to group SVPRF (P<0.05) and was insignificant 12 weeks different among both groups (Table 3).
| Table 3: Oswestry disability index and functional improvement of the studied groups | ||||
| Record Time | Intensity | Group TRF
(n = 30) |
Group SVPRF
(n = 30) |
P |
| Oswestry disability index | ||||
| Baseline | No disability | 3 (10) | 2 (6.67.) | 0.106 |
| Mild disability | 14 (46.67) | 6 (20) | ||
| Moderate disability | 12 (40) | 16 (53.33) | ||
| Severe disability | 1 (3.33) | 5 (16.67) | ||
| Crippled | 0 (0) | 1 (3.33) | ||
| 1 week | No disability | 2 (6.67) | 2 (6.67) | 0.043* |
| Mild disability | 18 (60) | 8 (26.67) | ||
| Moderate disability | 10 (33.33) | 15 (50) | ||
| Severe disability | 0 (0) | 4 (13.33) | ||
| Crippled | 0 (0) | 1 (3.33) | ||
| 4 weeks | No disability | 2 (6.67) | 2 (6.67) | 0.023* |
| Mild disability | 22 (73.33) | 10 (33.33) | ||
| Moderate disability | 6 (20) | 15 (50) | ||
| Severe disability | 0 (0) | 2 (6.67) | ||
| Crippled | 0 (0) | 1 (3.33) | ||
| 12 weeks | No disability | 4 (13.33) | 3 (10) | 0.122 |
| Mild disability | 24 (80) | 17 (56.67) | ||
| Moderate disability | 2 (6.67) | 8 (26.67) | ||
| Severe disability | 0 (0) | 0 (0) | ||
| Crippled | 0 (0) | 1 (3.33) | ||
| Functional improvement | ||||
| 1 week | Minimal | 4 (13.33) | 14 (46.67) | 0.038* |
| Mild | 10 (33.33) | 6 (20) | ||
| Moderate | 9 (30) | 7 (23.33) | ||
| Marked | 7 (23.33) | 3 (10) | ||
| 4 weeks | Minimal | 1 (3.33) | 5 (16.67) | 0.026* |
| Mild | 4 (13.33) | 11 (36.67) | ||
| Moderate | 11 (36.67) | 5 (16.67) | ||
| Marked | 14 (46.67) | 9 (30) | ||
| 12 weeks | Minimal | 0 (0) | 1 (3.33) | 0.069 |
| Mild | 1 (3.33) | 7 (23.33) | ||
| Moderate | 11 (36.67) | 6 (20) | ||
| Marked | 18 (60) | 16 (53.33) | ||
| Data presented as frequency (%). TRF: Thermo coagulation Radiofrequency; SVPRF: super voltage pulsed radio frequency; P < 0.05 considered as significant | ||||
Patients’ satisfaction, pain, hematoma, hypotension and numbness showed no significant differences among the groups (Table 4).
| Table 4: Patients satisfaction and complications of the studied groups | ||||
| Parameters | Group TRF
(n = 30) |
Group SVPRF
(n = 30) |
P | |
| Patients’
satisfaction |
Very much improved | 12 (40.0) | 9 (30.0) | 0.248 |
| Much improved | 9 (30.0) | 8 (26.67) | ||
| Minimally improved | 8 (26.67) | 7 (23.33) | ||
| No change | 1 (3.33) | 6 (20.0) | ||
| Worse | 0 (0.0) | 0 (0.0) | ||
| Much worse | 0 (0.0) | 0 (0.0) | ||
| Very much worse | 0 (0.0) | 0 (0.0) | ||
| Complications | Pain | 6 (20.0) | 1 (3.33) | 0.103 |
| Hematoma | 3 (10.0) | 0 (0.0) | 0.237 | |
| Hypotension | 2 (6.67) | 1 (3.33) | 1 | |
| Numbness | 4 (13.33) | 0 (0.0) | 0.112 | |
| Data presented as frequency (%). TRF: Thermo coagulation Radiofrequency;
SVPRF: super voltage pulsed radio frequency; P < 0.05 considered as significant |
||||
4. DISCUSSION
In cases of advanced pelvic cancer, pain prevalence can be as high as 85. Effective management of pain related to pelvic malignancies is frequently challenging due to the complex neuroanatomical structures and unique functional characteristics of the pelvic region.9
Our study revealed that VAS was significantly lower at (1 week, 4 weeks and 12 weeks) in group TRF relative to group SVPRF (P < 0.05) and showed no significant baseline differences among the groups.
This study is consistent with Usmani H et al. (2018), who reported significant pain relief at the time of discharge, with similar outcomes observed at 24 hours post-procedure.10 However, at the first, third, and sixth weeks of follow-up, patients in the CRF group demonstrated significantly greater pain relief compared to those in the PRF group.
Similarly, in the study by Reyad RM et al, who utilized mixed linear modeling to assess changes in pain scores. They reported that the estimated marginal mean ± SE
pain score for the RF group was 41.8 ± 1.04, providing further evidence of the impact of RF treatment on pain relief.6
In our results, Morphine sulphate consumption and Pregabalin consumption were significantly lower at (1 week, 4 weeks and 12 weeks) in group TRF compared to group SVPRF (P value<0.05) and showed no significant baseline differences among the groups. This notable reduction in both morphine and pregabalin consumption in the TRF group compared to SVPRF suggests that TRF may exert a more prolonged neuro-modulatory effect, potentially leading to a decreased reliance on opioid and neuropathic pain medications.
This aligns with the hypothesis that thermal RF achieves more sustained neural ablation, thereby reducing dependence on opioid and neuropathic pain medications. Supporting this notion Reyad RM et al. indicate that despite the application of RF, patients required an average morphine consumption of 49.0 ± 2.7 mg/day and pregabalin consumption of 145.9 ± 7.0 mg/day. This suggests that while RF provides pain relief, it may not completely eliminate the need for adjunctive analgesia.6
Similarly, Li Q et al. (2024) demonstrated that while RF therapy effectively alleviated perineal pain, oral morphine and pregabalin remained necessary for managing pain in other regions affected by cancer.11 Notably, no meaningful differences (P > 0.05) were observed in terms of daily morphine equivalent dose and pregabalin intake between the two groups before and six months post-treatment. These findings collectively suggest that while RF—particularly TRF—can significantly reduce analgesic requirements, a complete discontinuation of pain medications may not always be feasible, emphasizing the need for a multimodal pain management approach.
In our findings, the ODI was significantly lower at 1 week and 4 weeks in the TRF group versus the SVPRF group (P = 0.043 and 0.023, respectively), indicating reduced disability. Similarly, Functional improvement was significantly greater at the same time points in the TRF group versus the SVPRF group (P = 0.038 and 0.026, respectively), while no meaningful difference was observed among the groups at 12 weeks (P = 0.069).
In comparison, Reyad RM et al. (2018) documented a gradual decrease in disability levels over time in the RF group, with an increasing proportion of patients experiencing mild to moderate disability rather than severe impairment.6 However, the complete resolution of disability (no disability) was not achieved by week 12. Their findings also demonstrated that, despite some fluctuations, a substantial proportion of patients in the RF group attained at least moderate functional improvement by week 12.
Our study found that Patients satisfaction was showed no significant difference among both groups. Consistent with our findings, Reyad RM et al. (2018) found that in the RF group, patient satisfaction levels varied, with the majority reporting positive outcomes.6 A total of 60 of participants scored their improvement as either very much improved (30) or markedly improved (30). Additionally, 25 of patients reported minimal improvement, while 15 experienced no change in their condition. Notably, no patients in the RF group reported worsening symptoms. These findings suggest that RF treatment was generally well-received, with a substantial proportion of patients experiencing meaningful clinical improvement. The absence of negative outcomes further supports its role as a viable intervention for pain management.
However, our findings contrast consistent with those documented by Usmani H et al. (2018), observed that a significantly greater proportion of patients in the CRF group rated their satisfaction as excellent or good compared to those in the PRF group at the first, third, and sixth weeks of follow-up.10 Furthermore, overall patient satisfaction at the conclusion of the follow-up period was significantly higher in the CRF group than in the PRF group (P = 0.000). This discrepancy may be attributed to variations in patient selection criteria, procedural techniques, or post-procedural analgesic regimens between the studies. Additionally, the neuro-ablative effect of CRF, which results in more prolonged pain relief compared to PRF, could have contributed to the higher patient satisfaction observed in their study.
Our results showed that pain, hematoma, hypotension and numbness showed no significant differences among groups.
These findings are concordant with those reported by Usmani H et al. (2018) reported that participants were discharged from the hospital following four hours of observation without experiencing any adverse effects. No major neurological complications or untoward adverse effects were observed in either group throughout the follow-up period, except for minor infections at the skin puncture site. Infection occurred in three out of 34 patients in the CRF group and two out of 31 patients in the PRF group, with all affected patients responding well to oral antibiotics. The rate of this complication was similar between both groups, reinforcing the overall safety profile of both techniques. This alignment between our study and previous research supports the notion that both thermal and pulsed RF ablation are generally well-tolerated interventions with minimal procedural risks.
Moreover, our study is consistent with Reyad RM et al. (2018), who revealed that in the RF group, minor adverse events were observed in a small proportion of patients.6 Back pain was the most frequently reported minor complication, affecting 20 of patients. However, no cases of post-dural puncture headache, aseptic meningitis, or hypotension were reported in this group. Regarding major adverse events, no patients in the RF group encountered dysesthesia of the lower limbs, lower limb paresis, bladder dysfunction, or fecal incontinence. Consequently, the per-patient incidence of major adverse events in this group was 0. This suggests a favorable safety profile for RF treatment, with minimal risk of serious complications.
5. LIMITATIONS
The limitations of the study included that study was performed at a single institution, which could constrain the applicability of the results to broader populations. Short-term follow-up: While significant differences were observed at 1-week and 4-week intervals, prolonged follow-up is essential to assess sustained pain relief and functional improvement, small sample size: The study included only 60 patients, which may not be fully representative of the larger patient population with malignant perineal pain, single-blind design: While patients were blinded to the intervention, clinicians were not, which may introduce potential bias in assessments, heterogeneous patient conditions: Variations in tumor type, stage, and prior pain management strategies might have influenced individual responses to treatment.
6. CONCLUSION
TRF was superior to SVPRF in terms of pain reduction (VAS scores), reduced opioid (morphine sulfate) and pregabalin consumption, and improved functional outcomes (Oswestry Disability Index and functional improvement scores) over short- and mid-term follow-ups (1 week, 4 weeks, and 12 weeks). However, no meaningful differences were observed among the two groups regarding patient satisfaction and the incidence of complications. These findings suggest that TRF may be superior in efficacy intervention for managing refractory malignant perineal pain compared to SVPRF while maintaining a similar safety profile.
7. Data availability
The numerical data generated during this research is available with the authors.
8. Conflict of interest
All authors declare that there was no conflict of interest.
9. Funding
The study utilized the hospital resources only, and no external or industry funding was involved.
10. Authors’ contribution
BZTW: Study concept and design.
KAAE: Analysis and interpretation of data.
RMR: Critical revision of the manuscript for important intellectual content.
HZG: Administrative, technical, and material support.
11. REFERENCES
- Joshi M. Textbook of Pain Management-Muralidhar Joshi 2nd Edition2009. [FullText]
- Apte G, Nelson P, Brismée JM, Dedrick G, Justiz III R, Sizer Jr PS. Chronic female pelvic pain—part 1: clinical pathoanatomy and examination of the pelvic region.[PubMed] DOI: 1111/j.1533-2500.2011.00465.x
- Bielefeldt K, Lamb K, Gebhart GF. Convergence of sensory pathways in the development of somatic and visceral hypersensitivity. Am J Physiol Gastrointest Liver Physiol. [PubMed] DOI: 1152/ajpgi.00585.2005
- Adams N, Poole H, Richardson C. Psychological approaches to chronic pain management: part 1. J Clin Nurs. [PubMed] DOI: 1111/j.1365-2702.2006.01304.x
- Anekar AA, Hendrix JM, Cascella M. WHO analgesic ladder. StatPearls [Internet]: StatPearls Publishing. [PubMed] PMID: 32119322
- Reyad RM, Hakim SM, Abbas DN, Ghobrial HZ, Mansour E. A novel technique of saddle rhizotomy using thermal radiofrequency for intractable perineal pain in pelvic malignancy: a pilot study. Pain physician. [PubMed] PMID: 30508996
- Steinbok P, Schrag C. Complications after selective posterior rhizotomy for spasticity in children with cerebral palsy. Pediatr Neurosurg. [PubMed] DOI: 1159/000028668
- Byrd D, Mackey S. Pulsed radiofrequency for chronic pain. Curr Pain Headache Rep. [PubMed] DOI: 1007/s11916-008-0008-3
- Cascella M, Muzio MR, Viscardi D, Cuomo A. Features and role of minimally invasive palliative procedures for pain management in malignant pelvic diseases: A review. Am J Hosp Palliat Care. [PubMed] DOI: 1177/1049909116636374
- Usmani H, Dureja GP, Andleeb R, Tauheed N, Asif N. Conventional radiofrequency thermocoagulation vs pulsed radiofrequency neuromodulation of ganglion impar in chronic perineal pain of nononcological origin. Pain Med. [PubMed] DOI: 1093/pm/pnx244
- Li Q, Wang H, Zhong B, Zhang T, Wang Z, Tao P, et al. Conventional versus high-voltage, long-term pulse Radiofrequency of ganglion impar in perineal pain with advanced rectal cancer: a Randomized, double-blind controlled trial. BMC Anesthesiol. [PubMed] DOI: 1186/s12871-024-02717-0