Bhavini Shah 1 , Niveditha Kishore Srinivasan 2 , Ibrahim Saleem Mainaparambil 3
Authors affiliations:
Primary hyperparathyroidism (PHPT) can have disparate systemic manifestations, one being metabolic bone disease leading to pathological fractures. Ectopic mediastinal parathyroid adenomas present with special diagnostic and surgical challenges. We present the case of a 23-year-old female patient who developed a pathological fracture of the right femur secondary to hyperparathyroidism. Initial hypocalcemia was treated with intravenous calcium gluconate before definitive treatment. Ultrasonography showed the presence of an ectopic parathyroid adenoma in the mediastinum that was safely excised by video-assisted thoracoscopic surgery (VATS). Anesthetic care involved combined general anesthesia (GA) and thoracic epidural anesthesia, one-lung ventilation (OLV), and vigorous intraoperative monitoring. The postoperative course was uncomplicated with good pain management and restoration of metabolism. Definitive orthopedic stabilization was to be done after endocrine optimization. This case implies the requirement of early diagnosis, multidisciplinary treatment, and staged operation in PHPT patients with complex skeletal presentation.
Keywords: Ectopic parathyroid adenoma; general anesthesia; hypocalcemia; one-lung ventilation; pathological fracture
Citation: Shah B, Srinivasan NK, Mainaparambil IS. Bone hunger and broken bones: managing a mediastinal parathyroid adenoma with pathological fracture of a femur in a young female. Anaesth. pain intensive care 2025;29(9):xxxxxxxx. DOI: 10.35975/apic.v29i9.xxxx
Received: September 15, 2025; Revised: October 26, 2025; Accepted: November 06, 2025
Primary hyperparathyroidism (PHPT) is an endocrine disorder characterized by the inappropriate hypersecretion of parathyroid hormone, producing hypercalcemia, demineralization of bone, and multisystem disease. The majority of cases result from a single adenoma and pose complex diagnostic and surgical problems because of their unusual locations and for delayed diagnosis.1,2 Mediastinal ectopic parathyroid adenomas are most commonly secondary to dysmorphic embryologic migration and will cause recurrent or chronic hyperparathyroidism if they are not identified. Preoperative diagnosis and surgical removal of adenoma are essential to manage metabolic bone disease and for the prevention of systemic complications. Video-assisted thoracoscopic surgery (VATS) is a technique for mediastinal adenomas with lesser morbidity and quicker recovery compared with open surgery.3,4
We report the perioperative management of a symptomatic hyperparathyroidism in a young female complicated by pathological femoral fracture and ectopic mediastinal parathyroid adenoma, requiring staged surgical management by VATS resection before orthopedic stabilization.
A 23-year-old female, 45 kg, 150 cm, presented with a right femoral fracture following minor trauma. she had a two-year history of recurrent arthropathic pain, suggesting chronic metabolic bone disease. She previously underwent intramedullary nailing of the left femur under spinal anesthesia, complicated by a transfusion reaction in the form of rash and pruritus after packed red blood cell transfusion.
Preoperatively, serum calcium was 7.4 mg/dL, likely due to bone hunger, and was corrected with intravenous (IV) calcium gluconate to 12.8 mg/dL; vitamin D was low at 11.9 ng/mL.
Ultrasonography revealed a 19×20×24 mm parathyroid adenoma, anterior to the superior vena cava, beside the superior pulmonary veins. Magnetic resonance imaging revealed two small intrathyroidal lesions in the left thyroid lobe. Electrocardiography, echocardiogram, and chest X-ray (Figure 1) were normal and American Society of Anesthesiologists' (ASA) class II was assigned. With hyperparathyroidism considered the underlying cause, VATS adenomectomy was prioritised.
Figure 1: Pre-operative chest X-ray showing the ectopic mediastinal mass
The patient was kept nil per os for six hours before surgery. Standard ASA monitoring was employed in the operating room, and an 18-G intravenous catheter was inserted for intravenous access.
The plan of anesthesia was decided to be thoracic epidural followed by induction of general anesthesia. Perioperative analgesia was achieved by thoracic epidural catheter placement in the T7–T8 interspace and fixed at 11 cm on the skin level. Test dose of 3 mL of 2% lignocaine with adrenaline (1:200,000) was given.
Following this, the patient received glycopyrrolate 0.2 mg, midazolam 1 mg, and fentanyl 100 mcg IV. Anesthesia was induced with propofol 100 mg IV. Neuromuscular blockade was achieved with 8 mg of vecuronium. Airway management was achieved by placing a left-sided 35 Fr double-lumen endotracheal tube to facilitate lung isolation for VATS. Proper tube placement and positioning were confirmed by auscultation and fiberoptic bronchoscopy.
Post-induction, a 7 Fr triple-lumen central line (right subclavian) and 20G arterial line (left radial) were placed under ultrasound guidance.
Anesthesia was maintained with sevoflurane in a 50:50 oxygen-air mixture, supplemented intermittently with boluses of vecuronium. Ventilation was changed to OLV at the optimal surgical time, employing a lung-protective ventilation strategy with 5 mL/kg ideal body weight tidal volume, 5 cmH₂O positive end-expiratory pressure (PEEP), and peak airway pressures below 25 cmH₂O, thus maintaining hypoxic pulmonary vasoconstriction (HPV). The non-dependent lung was permitted to collapse to optimize surgical exposure passively.
An epidural bolus of 6 mL of 0.25% bupivacaine with 3 mg morphine was given for analgesia prior to the beginning of the surgery. Intraoperatively, epidural boluses of 6 mL of 0.25% bupivacaine were given as required to provide adequate analgesia. Hemodynamic variables were closely monitored during the procedure. Intraoperatively, blood loss was minimal, with urine output of 600 mL, managed using 1500 mL Ringer’s lactate. At the end of surgery, neuromuscular blockade was reversed with intravenous sugammadex 200 mg. The patient was extubated awake after confirming spontaneous ventilation, hemodynamic stability, and complete reversal of neuromuscular blockade. Post-operatively, the patient was transferred to the surgical intensive care unit for observation and continuation of epidural analgesia through a continuous infusion of 0.125% bupivacaine at 6 mL/hour.
PHPT is most caused by a single adenoma secreting excess parathyroid hormone and hypercalcemia with multisystem manifestations of bone resorption and skeletal weakness. Severe bone disease in the form of delayed diagnosis leading to pathological fractures can occur in young patients.1 Embryologic migration defects cause ectopic mediastinal parathyroid adenomas. Surgical excision is still the treatment of choice, and VATS provides a minimal invasive approach with acceptable results over open thoracotomy. 2,4
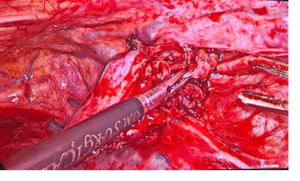
Figure 2: Intraoperative image showing ectopic mediastinal parathyroid adenoma
Anesthesia management in PHPT patients is challenging in more than one dimension. Hypercalcemia may lead to cardiac arrhythmia, hypertension, and neuromuscular dysfunction. Bone weakness demands meticulous care and stabilisation to avoid iatrogenic fracture during the perioperative time. The disease could occur as part of the clinical manifestation of multiple endocrine neoplasia type 1 (MEN1) or type 2a (MEN2a).5,6
The combination of GA with thoracic epidural analgesia (TEA) yielded many benefits. TEA provides superior perioperative pain control, minimizing systemic opioid usage and its resultant side effects of respiratory depression and sedation, enhances postoperative pulmonary function, attenuates stress response, and facilitates early mobilization, all key determinants in thoracic surgery patients. Epidural anesthesia can also blunt sympathetic responses, enabling intraoperative hemodynamic stability, essential in high-risk metabolic and cardiovascular patients.7,8
For VATS, OLV enabled optimal exposure by deflating the operative lung. Lung-protective ventilation preserved HPV and minimized ventilator-induced injury without extra interventions. Sevoflurane's anti-inflammatory and bronchodilator properties maximized optimal respiratory conditions during OLV.9
This case illustrates the complex association between endocrinopathy and orthopedic complications in PHPT, particularly from an ectopic mediastinal parathyroid adenoma. A pathological femoral fracture in a young adult highlights the importance of early recognition and comprehensive evaluation of metabolic bone disease in atypical fractures. Successful resection of the adenoma, aided by TEA and lung-protective ventilation, enabled smooth perioperative recovery. This case highlights the importance of multimodal treatment involving endocrinology, radiology, anesthesia, thoracic surgery, and orthopedics. Staged treatment with stress on metabolic correction and adenoma excision before orthopedic stabilization maximized clinical gain at low perioperative risk, emphasizing the value of multidisciplinary care and timely intervention.
NKS: Concept, conduction of the study work, literature search and manuscript editing
Authors affiliations:
- Bhavini Shah, Professor of Anesthesiology, Dr. D.Y. Patil Medical College, Hospital & Research Centre, Pimpri, Pune, India; Email: Drbhavinishah71@gmail.com
- Niveditha Kishore Srinivasan, Department of Anesthesiology, Dr. D.Y. Patil Medical College, Hospital & Research Centre, Pimpri, Pune, India; Email: niveditha2899@gmail.com
- Ibrahim Saleem Mainaparambil, Resident, Department of Anesthesiology, Dr. D.Y. Patil Medical College, Hospital & Research Centre, Pimpri, Pune, India; Email: ibrahimsaleem1997@gmail.com
ABSTRACT
Primary hyperparathyroidism (PHPT) can have disparate systemic manifestations, one being metabolic bone disease leading to pathological fractures. Ectopic mediastinal parathyroid adenomas present with special diagnostic and surgical challenges. We present the case of a 23-year-old female patient who developed a pathological fracture of the right femur secondary to hyperparathyroidism. Initial hypocalcemia was treated with intravenous calcium gluconate before definitive treatment. Ultrasonography showed the presence of an ectopic parathyroid adenoma in the mediastinum that was safely excised by video-assisted thoracoscopic surgery (VATS). Anesthetic care involved combined general anesthesia (GA) and thoracic epidural anesthesia, one-lung ventilation (OLV), and vigorous intraoperative monitoring. The postoperative course was uncomplicated with good pain management and restoration of metabolism. Definitive orthopedic stabilization was to be done after endocrine optimization. This case implies the requirement of early diagnosis, multidisciplinary treatment, and staged operation in PHPT patients with complex skeletal presentation.
Keywords: Ectopic parathyroid adenoma; general anesthesia; hypocalcemia; one-lung ventilation; pathological fracture
Citation: Shah B, Srinivasan NK, Mainaparambil IS. Bone hunger and broken bones: managing a mediastinal parathyroid adenoma with pathological fracture of a femur in a young female. Anaesth. pain intensive care 2025;29(9):xxxxxxxx. DOI: 10.35975/apic.v29i9.xxxx
Received: September 15, 2025; Revised: October 26, 2025; Accepted: November 06, 2025
1. INTRODUCTION
Primary hyperparathyroidism (PHPT) is an endocrine disorder characterized by the inappropriate hypersecretion of parathyroid hormone, producing hypercalcemia, demineralization of bone, and multisystem disease. The majority of cases result from a single adenoma and pose complex diagnostic and surgical problems because of their unusual locations and for delayed diagnosis.1,2 Mediastinal ectopic parathyroid adenomas are most commonly secondary to dysmorphic embryologic migration and will cause recurrent or chronic hyperparathyroidism if they are not identified. Preoperative diagnosis and surgical removal of adenoma are essential to manage metabolic bone disease and for the prevention of systemic complications. Video-assisted thoracoscopic surgery (VATS) is a technique for mediastinal adenomas with lesser morbidity and quicker recovery compared with open surgery.3,4
We report the perioperative management of a symptomatic hyperparathyroidism in a young female complicated by pathological femoral fracture and ectopic mediastinal parathyroid adenoma, requiring staged surgical management by VATS resection before orthopedic stabilization.
2. CASE REPORT
A 23-year-old female, 45 kg, 150 cm, presented with a right femoral fracture following minor trauma. she had a two-year history of recurrent arthropathic pain, suggesting chronic metabolic bone disease. She previously underwent intramedullary nailing of the left femur under spinal anesthesia, complicated by a transfusion reaction in the form of rash and pruritus after packed red blood cell transfusion.
Preoperatively, serum calcium was 7.4 mg/dL, likely due to bone hunger, and was corrected with intravenous (IV) calcium gluconate to 12.8 mg/dL; vitamin D was low at 11.9 ng/mL.
Ultrasonography revealed a 19×20×24 mm parathyroid adenoma, anterior to the superior vena cava, beside the superior pulmonary veins. Magnetic resonance imaging revealed two small intrathyroidal lesions in the left thyroid lobe. Electrocardiography, echocardiogram, and chest X-ray (Figure 1) were normal and American Society of Anesthesiologists' (ASA) class II was assigned. With hyperparathyroidism considered the underlying cause, VATS adenomectomy was prioritised.
Figure 1: Pre-operative chest X-ray showing the ectopic mediastinal mass
The patient was kept nil per os for six hours before surgery. Standard ASA monitoring was employed in the operating room, and an 18-G intravenous catheter was inserted for intravenous access.
The plan of anesthesia was decided to be thoracic epidural followed by induction of general anesthesia. Perioperative analgesia was achieved by thoracic epidural catheter placement in the T7–T8 interspace and fixed at 11 cm on the skin level. Test dose of 3 mL of 2% lignocaine with adrenaline (1:200,000) was given.
Following this, the patient received glycopyrrolate 0.2 mg, midazolam 1 mg, and fentanyl 100 mcg IV. Anesthesia was induced with propofol 100 mg IV. Neuromuscular blockade was achieved with 8 mg of vecuronium. Airway management was achieved by placing a left-sided 35 Fr double-lumen endotracheal tube to facilitate lung isolation for VATS. Proper tube placement and positioning were confirmed by auscultation and fiberoptic bronchoscopy.
Post-induction, a 7 Fr triple-lumen central line (right subclavian) and 20G arterial line (left radial) were placed under ultrasound guidance.
Anesthesia was maintained with sevoflurane in a 50:50 oxygen-air mixture, supplemented intermittently with boluses of vecuronium. Ventilation was changed to OLV at the optimal surgical time, employing a lung-protective ventilation strategy with 5 mL/kg ideal body weight tidal volume, 5 cmH₂O positive end-expiratory pressure (PEEP), and peak airway pressures below 25 cmH₂O, thus maintaining hypoxic pulmonary vasoconstriction (HPV). The non-dependent lung was permitted to collapse to optimize surgical exposure passively.
An epidural bolus of 6 mL of 0.25% bupivacaine with 3 mg morphine was given for analgesia prior to the beginning of the surgery. Intraoperatively, epidural boluses of 6 mL of 0.25% bupivacaine were given as required to provide adequate analgesia. Hemodynamic variables were closely monitored during the procedure. Intraoperatively, blood loss was minimal, with urine output of 600 mL, managed using 1500 mL Ringer’s lactate. At the end of surgery, neuromuscular blockade was reversed with intravenous sugammadex 200 mg. The patient was extubated awake after confirming spontaneous ventilation, hemodynamic stability, and complete reversal of neuromuscular blockade. Post-operatively, the patient was transferred to the surgical intensive care unit for observation and continuation of epidural analgesia through a continuous infusion of 0.125% bupivacaine at 6 mL/hour.
3. DISCUSSION
PHPT is most caused by a single adenoma secreting excess parathyroid hormone and hypercalcemia with multisystem manifestations of bone resorption and skeletal weakness. Severe bone disease in the form of delayed diagnosis leading to pathological fractures can occur in young patients.1 Embryologic migration defects cause ectopic mediastinal parathyroid adenomas. Surgical excision is still the treatment of choice, and VATS provides a minimal invasive approach with acceptable results over open thoracotomy. 2,4
Figure 2: Intraoperative image showing ectopic mediastinal parathyroid adenoma
Anesthesia management in PHPT patients is challenging in more than one dimension. Hypercalcemia may lead to cardiac arrhythmia, hypertension, and neuromuscular dysfunction. Bone weakness demands meticulous care and stabilisation to avoid iatrogenic fracture during the perioperative time. The disease could occur as part of the clinical manifestation of multiple endocrine neoplasia type 1 (MEN1) or type 2a (MEN2a).5,6
The combination of GA with thoracic epidural analgesia (TEA) yielded many benefits. TEA provides superior perioperative pain control, minimizing systemic opioid usage and its resultant side effects of respiratory depression and sedation, enhances postoperative pulmonary function, attenuates stress response, and facilitates early mobilization, all key determinants in thoracic surgery patients. Epidural anesthesia can also blunt sympathetic responses, enabling intraoperative hemodynamic stability, essential in high-risk metabolic and cardiovascular patients.7,8
For VATS, OLV enabled optimal exposure by deflating the operative lung. Lung-protective ventilation preserved HPV and minimized ventilator-induced injury without extra interventions. Sevoflurane's anti-inflammatory and bronchodilator properties maximized optimal respiratory conditions during OLV.9
4. CONCLUSION
This case illustrates the complex association between endocrinopathy and orthopedic complications in PHPT, particularly from an ectopic mediastinal parathyroid adenoma. A pathological femoral fracture in a young adult highlights the importance of early recognition and comprehensive evaluation of metabolic bone disease in atypical fractures. Successful resection of the adenoma, aided by TEA and lung-protective ventilation, enabled smooth perioperative recovery. This case highlights the importance of multimodal treatment involving endocrinology, radiology, anesthesia, thoracic surgery, and orthopedics. Staged treatment with stress on metabolic correction and adenoma excision before orthopedic stabilization maximized clinical gain at low perioperative risk, emphasizing the value of multidisciplinary care and timely intervention.
- Conflict of interest
- Ethical considerations
- Authors’ contribution
NKS: Concept, conduction of the study work, literature search and manuscript editing
8. REFERENCES
- Madkhali T, Alhefdhi A, Chen H, Elfenbein D. Primary hyperparathyroidism. Turk J Surg. 2016;32(1):58–66.
- Hu J, Ngiam K, Parameswaran R. Mediastinal parathyroid adenomas and their surgical implications. Ann R Coll Surg Engl. 2015;97(4):259–61. PMCID: PMC4473861 DOI: 1308/003588415X14181254789088
- Amer K, Khan AZ, Rew D, Lagattolla N, Singh N. Video assisted thoracoscopic excision of mediastinal ectopic parathyroid adenomas: A UK regional experience. Ann Cardiothorac Surg. 2015;4(6):527–34. PMCID: PMC4669253 DOI: 3978/j.issn.2225-319X.2015.09.04
- Chopra P, Mitra S. Patients with symptomatic primary hyperparathyroidism: An anaesthetic challenge. Indian J Anaesth. 2009;53(4):492–5. PMCID: PMC2894492
- Freise H, Van Aken HK. Risks and benefits of thoracic epidural anaesthesia. Br J Anaesth. 2011;107(6):859–68. DOI: 1093/bja/aer339
- Tay YZ, Balasubbiah N, Awang RR, Pandian BD, Sathiamurthy N, Tay Y. A Surgical Management of Mediastinal Parathyroid Adenoma: A Regional Experience in Malaysia. Cureus. 2024 Mar 23;16(3). PMCID: PMC11034996 DOI: 7759/cureus.56792
- Dhanure V, Bhalerao N, Paul A. Successful management of arachnoid cyst and syringomyelia using thoracic epidural anesthesia and general anesthesia: A case report. Multidiscip Sci J. 2025 May 23;7(11):2025544. https://doi.org/10.31893/multiscience.2025544
- Yang Y, Jia D, Cheng L, Jia K, Wang J. Continuous positive airway pressure combined with small-tidal-volume ventilation on arterial oxygenation and pulmonary shunt during one-lung ventilation in patients undergoing video-assisted thoracoscopic lobectomy: A randomized, controlled study. Ann Thorac Med. 2024;19(2):155–64. PMCID: PMC11100470 DOI: 4103/atm.atm_240_23
- Min SH, Yoon S, Choe HW, Seo JH, Bahk JH. An optimal protective ventilation strategy in lung resection surgery: A prospective, single-center, 3-arm randomized controlled trial. Updates Surg. 2025 Jun;77(3):925-935. PMCID: PMC12226653 DOI: 1007/s13304-025-02091-7