Mohammed Mahmood Ali 1 , Naveen Kumar 2 , Omar Mohamed Alahmed 3 ,
Hamad E. Alshamsi 4
Authors affiliations;
Anatomical variations of peripheral nerves are of great significance to anesthesiologists and pain specialists, as they can impact the safety and efficacy of interventional pain therapies, perioperative analgesia, and regional anesthesia. We report here an abnormal communication between the median nerve (MN) and the musculocutaneous nerve (MCN) in the left arm of an elderly male cadaver. The MCN, following its normal exit after piercing the coracobrachialis muscle and providing the branches to the biceps brachii muscle, joined the trunk of the MN proximal to the branch given off to the brachialis muscle. On its further course, it continued as the lateral cutaneous nerve of the forearm, supplying the skin of the lateral part of the forearm. Precise knowledge of variations in MCN and MN communications is vital during treatment of the traumatology of the shoulder joint, in plastic and reconstructive repair operations, as well as to the anesthetist performing pain management therapies on the upper limb.
Abbreviations: CB: Coracobrachialis, MCN: musculocutaneous nerve, MN: median nerve,
Keywords: Median nerve; Musculocutaneous nerve; Communication; Electroneurography
Citation: Ali MM, Kumar N, Alahmed OM, Alshamsi HE. Unilateral communication between the median and musculocutaneous nerves: implications for regional anesthesia. Anaesth. pain intensive care 2025;29(9):1317-20. DOI: 10.35975/apic.v29i9.3073
Received: August 20, 2025; Accepted: September 29, 2025
In the clinical and surgical fields, variations like an abnormal communication between the branches of the brachial plexus or their aberrant branching pattern are of enormous significance. The median nerve (MN) generally communicates with the ulnar nerve in the arm. However, communication between MN and MCN is among the rare variations. These variations may constitute a major concern in the clinical and surgical fields. Seldom are reports found in scientific literature on the possible reasons for abnormal communication between the median and musculocutaneous nerves. Though the exact cause of communication is not clear, it is believed that the overlapping of a few common fibers (C6-C7) between the aforementioned peripheral nerves is one of the incidental causes 1.
Many researchers have attempted to establish the categorization of the MN-MCN communication pattern using various standards. However, no single classification is currently standardized. Venieratos and Anagnostopoulou (1998) introduced the simplified pattern of aberrant communications into three types;2 over the existing Le Minor (1992) classification of five types.3 Later, distinct classification was introduced by Choi et al. (2000) and Guerri-Guttengerg (2002).4.5 Venieratos and Anagnostopoulou's (VA) classification was based on whether the communication occurred prior to or following the MCN penetrating the coracobrachialis (CB) muscle. According to VA classification, the communication between the nerves is proximal to the MCN piercing the CB muscle in type I, distal to the CB muscle in type II, and neither the nerve nor the communicating branch pierces the CB muscle in type III.
During the routine cadaveric dissection of the upper limb for undergraduate students, we noticed an aberrant communication between the median and musculocutaneous nerves on the front of the left arm of an elderly male cadaver with an approximate age of 70 years. The formation of the cords of the brachial plexus was normal as observed in the axilla. The medial and lateral cords' contributions to the median nerve formation and its progression through the arm were also found to be normal. The musculocutaneous nerve, originating from the lateral cord of the brachial plexus, passes through the coracobrachialis muscle and supplies it. After is exits from the muscle, it provides two divisions. While its lateral division supplied the biceps brachii muscle, the prominent medial division provided a branch to the brachialis muscle. Before its supply to the brachialis, the nerve fibers were found to be communicating with the trunk of the median nerve. The branch supplying the brachialis muscle proceeded further as lateral cutaneous nerve of forearm. (Figure 1). No further nervous anomalies were observed in the cadaver.
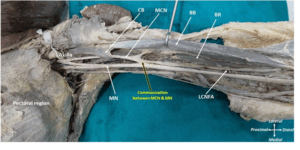
Figure 1: Dissection of left axilla and front of the arm showing the communicating branch extends from the musculocutaneous nerve (MCN) to the median nerve (MN) after the former pierces the coracobrachialis muscle (CB). BB- Biceps brachii, BR—brachioradialis, LCNFA—lateral cutaneous nerve of the forearm
Although rare, the communication between the median and musculocutaneous nerves can change the expected sensory and motor blocking that occurs with peripheral nerve or brachial plexus blocks. Unexpected neurological reactions, insufficient analgesia, or incomplete anesthesia could arise from a failure to notice such variances.
The mechanism of embryological development of limb muscle and peripheral nerves is influenced by arbitrary circumstances, which might be the cause of abnormal communication between peripheral nerves. Altered signaling between mesenchymal cells and neuronal growth cones mostly attributes to the abnormal communication between the nerves of the brachial plexus6.
According to Venieratos and Anagnostopoulou's classification,2 there were three types, based on the sites of communication;
Type I: The communication was proximal to the entrance of the musculocutaneous nerve into coracobrachialis (9/22);
Type II: The communication was distal to the muscle (10/22), and
Type III: The nerve as well as the communicating branch did not pierce the muscle (3/22).
According to this categorization, the present pattern is classified as Type II. The overall incidence of the current pattern is 7.7% according to Guerri-Guttenberg (2009),5 35% according to Loukas & Aqueelah (2005),7 45% according to Venieratos and Anagnostopoulou, and 14% according to Kumar et al. (2013).8 This demonstrates the global diversity of communication between MN and MCN. Ballesteros et al. (2014) observed an overall 19.8% occurrence of communication with an almost similar number of cases of bilateral and unilateral existence.9
Anatomical variations exhibiting nerve communications may aggravate or improve the symptoms, causing motor and sensory changes compared to the usual distribution pattern.
Following its motor distribution, the MCN continues as the lateral cutaneous nerve of the forearm. Presence of a connection band with the neighboring nerves: forced flexion of the forearm may cause painful and paresthetic symptoms in the anterolateral part of the forearm.10 Electroneurography examinations to identify the specific functions of the communicating branch of the median nerve are useful in surgical procedures. Therefore, prior knowledge of such variations helps the clinician properly understand the case and reduces the risk of complications during surgical procedures in its area of distribution.
Recognizing these variations would also emphasize their immediate practical relevance to the practice of anesthesia and pain management.
Precise knowledge of variations in MCN and MN communications is vital during the treatment of trauma of the shoulder joint, in plastic and reconstructive repair operations, and for the anesthetist performing pain management therapies on the upper limb.
OMA, HEA, NK: Analysis and interpretation:
NK: Final approval of the article
Hamad E. Alshamsi 4
Authors affiliations;
- Mohammed Mahmood Ali, RAK College of Medical Sciences, RAK Medical & Health Sciences University, Ras Al Khaimah, UAE; Email: mohammed.23901054@rakmhsu.ac.ae
- Naveen Kumar, RAK College of Medical Sciences, RAK Medical & Health Sciences University, Ras Al Khaimah, UAE; Email: aveentonse@gmail.com; {ORCID:0000-0003-2805-779X
- Omar Mohamed Alahmed. RAK College of Medical Sciences, RAK Medical & Health Sciences University, Ras Al Khaimah, UAE; Email: omar.23901109@rakmhsu.ac.ae
- Hamad E Alshamsi, RAK College of Medical Sciences, RAK Medical & Health Sciences University, Ras Al Khaimah, UAE; Email: hamad.23901126@rakmhsu.ac.ae
ABSTRACT
Anatomical variations of peripheral nerves are of great significance to anesthesiologists and pain specialists, as they can impact the safety and efficacy of interventional pain therapies, perioperative analgesia, and regional anesthesia. We report here an abnormal communication between the median nerve (MN) and the musculocutaneous nerve (MCN) in the left arm of an elderly male cadaver. The MCN, following its normal exit after piercing the coracobrachialis muscle and providing the branches to the biceps brachii muscle, joined the trunk of the MN proximal to the branch given off to the brachialis muscle. On its further course, it continued as the lateral cutaneous nerve of the forearm, supplying the skin of the lateral part of the forearm. Precise knowledge of variations in MCN and MN communications is vital during treatment of the traumatology of the shoulder joint, in plastic and reconstructive repair operations, as well as to the anesthetist performing pain management therapies on the upper limb.
Abbreviations: CB: Coracobrachialis, MCN: musculocutaneous nerve, MN: median nerve,
Keywords: Median nerve; Musculocutaneous nerve; Communication; Electroneurography
Citation: Ali MM, Kumar N, Alahmed OM, Alshamsi HE. Unilateral communication between the median and musculocutaneous nerves: implications for regional anesthesia. Anaesth. pain intensive care 2025;29(9):1317-20. DOI: 10.35975/apic.v29i9.3073
Received: August 20, 2025; Accepted: September 29, 2025
1. INTRODUCTION
In the clinical and surgical fields, variations like an abnormal communication between the branches of the brachial plexus or their aberrant branching pattern are of enormous significance. The median nerve (MN) generally communicates with the ulnar nerve in the arm. However, communication between MN and MCN is among the rare variations. These variations may constitute a major concern in the clinical and surgical fields. Seldom are reports found in scientific literature on the possible reasons for abnormal communication between the median and musculocutaneous nerves. Though the exact cause of communication is not clear, it is believed that the overlapping of a few common fibers (C6-C7) between the aforementioned peripheral nerves is one of the incidental causes 1.
Many researchers have attempted to establish the categorization of the MN-MCN communication pattern using various standards. However, no single classification is currently standardized. Venieratos and Anagnostopoulou (1998) introduced the simplified pattern of aberrant communications into three types;2 over the existing Le Minor (1992) classification of five types.3 Later, distinct classification was introduced by Choi et al. (2000) and Guerri-Guttengerg (2002).4.5 Venieratos and Anagnostopoulou's (VA) classification was based on whether the communication occurred prior to or following the MCN penetrating the coracobrachialis (CB) muscle. According to VA classification, the communication between the nerves is proximal to the MCN piercing the CB muscle in type I, distal to the CB muscle in type II, and neither the nerve nor the communicating branch pierces the CB muscle in type III.
2. CASE REPORT
During the routine cadaveric dissection of the upper limb for undergraduate students, we noticed an aberrant communication between the median and musculocutaneous nerves on the front of the left arm of an elderly male cadaver with an approximate age of 70 years. The formation of the cords of the brachial plexus was normal as observed in the axilla. The medial and lateral cords' contributions to the median nerve formation and its progression through the arm were also found to be normal. The musculocutaneous nerve, originating from the lateral cord of the brachial plexus, passes through the coracobrachialis muscle and supplies it. After is exits from the muscle, it provides two divisions. While its lateral division supplied the biceps brachii muscle, the prominent medial division provided a branch to the brachialis muscle. Before its supply to the brachialis, the nerve fibers were found to be communicating with the trunk of the median nerve. The branch supplying the brachialis muscle proceeded further as lateral cutaneous nerve of forearm. (Figure 1). No further nervous anomalies were observed in the cadaver.
Figure 1: Dissection of left axilla and front of the arm showing the communicating branch extends from the musculocutaneous nerve (MCN) to the median nerve (MN) after the former pierces the coracobrachialis muscle (CB). BB- Biceps brachii, BR—brachioradialis, LCNFA—lateral cutaneous nerve of the forearm
3. DISCUSSION
Although rare, the communication between the median and musculocutaneous nerves can change the expected sensory and motor blocking that occurs with peripheral nerve or brachial plexus blocks. Unexpected neurological reactions, insufficient analgesia, or incomplete anesthesia could arise from a failure to notice such variances.
The mechanism of embryological development of limb muscle and peripheral nerves is influenced by arbitrary circumstances, which might be the cause of abnormal communication between peripheral nerves. Altered signaling between mesenchymal cells and neuronal growth cones mostly attributes to the abnormal communication between the nerves of the brachial plexus6.
According to Venieratos and Anagnostopoulou's classification,2 there were three types, based on the sites of communication;
Type I: The communication was proximal to the entrance of the musculocutaneous nerve into coracobrachialis (9/22);
Type II: The communication was distal to the muscle (10/22), and
Type III: The nerve as well as the communicating branch did not pierce the muscle (3/22).
According to this categorization, the present pattern is classified as Type II. The overall incidence of the current pattern is 7.7% according to Guerri-Guttenberg (2009),5 35% according to Loukas & Aqueelah (2005),7 45% according to Venieratos and Anagnostopoulou, and 14% according to Kumar et al. (2013).8 This demonstrates the global diversity of communication between MN and MCN. Ballesteros et al. (2014) observed an overall 19.8% occurrence of communication with an almost similar number of cases of bilateral and unilateral existence.9
Anatomical variations exhibiting nerve communications may aggravate or improve the symptoms, causing motor and sensory changes compared to the usual distribution pattern.
Following its motor distribution, the MCN continues as the lateral cutaneous nerve of the forearm. Presence of a connection band with the neighboring nerves: forced flexion of the forearm may cause painful and paresthetic symptoms in the anterolateral part of the forearm.10 Electroneurography examinations to identify the specific functions of the communicating branch of the median nerve are useful in surgical procedures. Therefore, prior knowledge of such variations helps the clinician properly understand the case and reduces the risk of complications during surgical procedures in its area of distribution.
Recognizing these variations would also emphasize their immediate practical relevance to the practice of anesthesia and pain management.
4. CONCLUSION
Precise knowledge of variations in MCN and MN communications is vital during the treatment of trauma of the shoulder joint, in plastic and reconstructive repair operations, and for the anesthetist performing pain management therapies on the upper limb.
- Conflict of Interest
- Source of funding
- Ethical considerations
- Authors’ contribution
OMA, HEA, NK: Analysis and interpretation:
NK: Final approval of the article
9. REFERENCES
- Clarissa Ann Elisabeth Gelmi, Francesca Alice Pedrini, Communication between median and musculocutaneous nerve at the level of cubital fossa - A case report Translational Research in Anatomy 2018;11: 1–4
- Venieratos D, Anagnostopoulou S. Classification of communications between the musculocutaneous and median nerves. Clin Anat 1998; 11:327–31. PMID: 9725577 DOI: 1002/(SICI)1098-2353(1998)11:5<327::AID-CA6>3.0.CO;2-M
- Le Minor JM. [A rare variation of the median and musculocutaneous nerves in man]. Arch Anat Histol Embryol 1990; 73: 33–42.
- Choi D, Rodriguez-Niedenfuhr M, Vazquez T, Parkin I, Sanudo JR. Patterns of connections between the musculocutaneous and median nerves in the axilla and arm. Clin Anat 2002; 15: 11–7.
- Guerri-Guttenberg RA, Ingolotti M. Classifying musculocutaneous nerve variations. Clin Anat 2009; 22: 671–83.
- Abhaya A, Bhardwaj R, Prakash R. Dual origin of musculocutaneous nerve. J Anat Society India 2003; 52: 94.
- Loukas M, Aqueelah H. Musculocutaneous and median nerve connections within, proximal and distal to the coracobrachialis muscle. Folia Morphol (Warsz) 2005; 64: 101–8.
- N Kumar, A Guru, MR D’Souza, J Patil, S Nayak B. Incidences and Clinical Implications of communications between Musculocutaneous Nerve and Median Nerve in the Arm – A Cadaveric Study. West Indian Med J 2013; 62 (8): 744
- Ballesteros LE, Forero PL, Buitrago ER. Communication between the musculocutaneous and median nerves in the arm: an anatomical study and clinical implications. Rev Bras Ortop. 2014; 27;50(5):567-72. doi: 10.1016/j.rboe.2014.08.009. PMID: 26535190; PMCID: PMC4610987.
- Caetano EB, Vieira LÂ, Cavalheiro CS, Razuk M Filho, Almargo MA, Caetano MF. Anatomic study of the nervous communication between the median and musculocutaneous nerve. Acta Ortop Bras. 2016;24(4):200-203. doi:10.1590/1413-78522016240415